4681
Differences in Myocardial Strain at End-Inspiration versus End-Expiration with Remote Exposure to Secondhand Tobacco Smoke1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Divisions of Pulmonary, Critical Care, Allergy, and Sleep Medicine and Occupational and Environmental Medicine, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Myocardium, Myocardium, Cardiopulmonary; Second-Hand Smoker
Prolonged exposure to secondhand tobacco smoke (SHS) is associated with abnormal pulmonary function and cardiovascular response. In this study, we examined cardiac function in SHS-exposed participants using cardiac MR (CMR) and displacement encoding with stimulated echoes (DENSE) to determine whether the cardiac function is affected by air trapping-a hallmark of heavy past SHS exposure. We found that SHS-exposed participants had lower myocardial radial strain than unexposed participants at both end-inspiration and end-expiration imaging. Neither stroke volume nor cardiac output exhibited the decrease seen in unexposed participants at end-inspiration, but radial strain was significantly lower compared to end-expiration in SHS-exposed participants.1. Introduction
Prolonged exposure to secondhand tobacco smoke (SHS), even when remote, is associated with abnormal pulmonary function including air trapping (an abnormal increase in volume of air remaining in the lungs at the end of exhalation) and an abnormal cardiovascular response to exercise including limited exercise-induced rise in oxygen-pulse, which may implicate an occult insufficiency in cardiac stroke volume with SHS exposure1.2. Objective
To thoroughly examine cardiac function in participants with history of SHS exposure using cardiac MR (CMR) and determine whether the cardiac function is affected by air trapping, as it is manifested by end-expiration versus end-inspiration breath holding.3. Methods
We examined 4 commercial aircrew members with history of heavy occupational SHS exposure and 4 healthy volunteers (never-smoker, no significant history of SHS exposure, cardiovascular disease, asthma or COPD). Participants were imaged with standard cine CMR in short-axis and 4-chamber views, and with Displacement Encoding with Stimulated Echoes (DENSE) at 1 to 2 mid-apical short-axis slices as well as a 4-chamber view. Imaging was performed at both end-inspiration and end-expiration. Left ventricular function was measured from cine CMR using commercial software (Circle, cvi42) and included end-systolic/diastolic volumes (ESV, EDV), stroke volume (SV), ejection fraction (EF) and cardiac output (CO). DENSE images were analyzed using DENSEanalysis (version 0.5.2). Peak longitudinal strain (ELL) was calculated from 4-chamber DENSE images and peak circumferential (ECC) and radial (ERR) strains were calculated from short-axis DENSE images. As an ancillary measurement to DENSE-measured strains, we manually measured myocardial thickness and myocardial circumference at end-systole and end-diastole in 2 mid-apical short axis slices and in 2 4-chamber views in the standard cine CMRs. From these measurements we calculated longitudinal, circumferential and radial myocardial stretch between systole and diastole (SLL, SCC, SRR, respectively). Parameters measured from end-inspiration (end-expiration) breath-holds are denoted by the subscript as “insp” (“exp”), e.g., EFinsp. We finally compared each parameter between SHS and normal volunteers using the unpaired t-test, and also between end-inspiration and end-expiration acquisitions for SHS and normal subjects independently using the paired t-test.4. Results
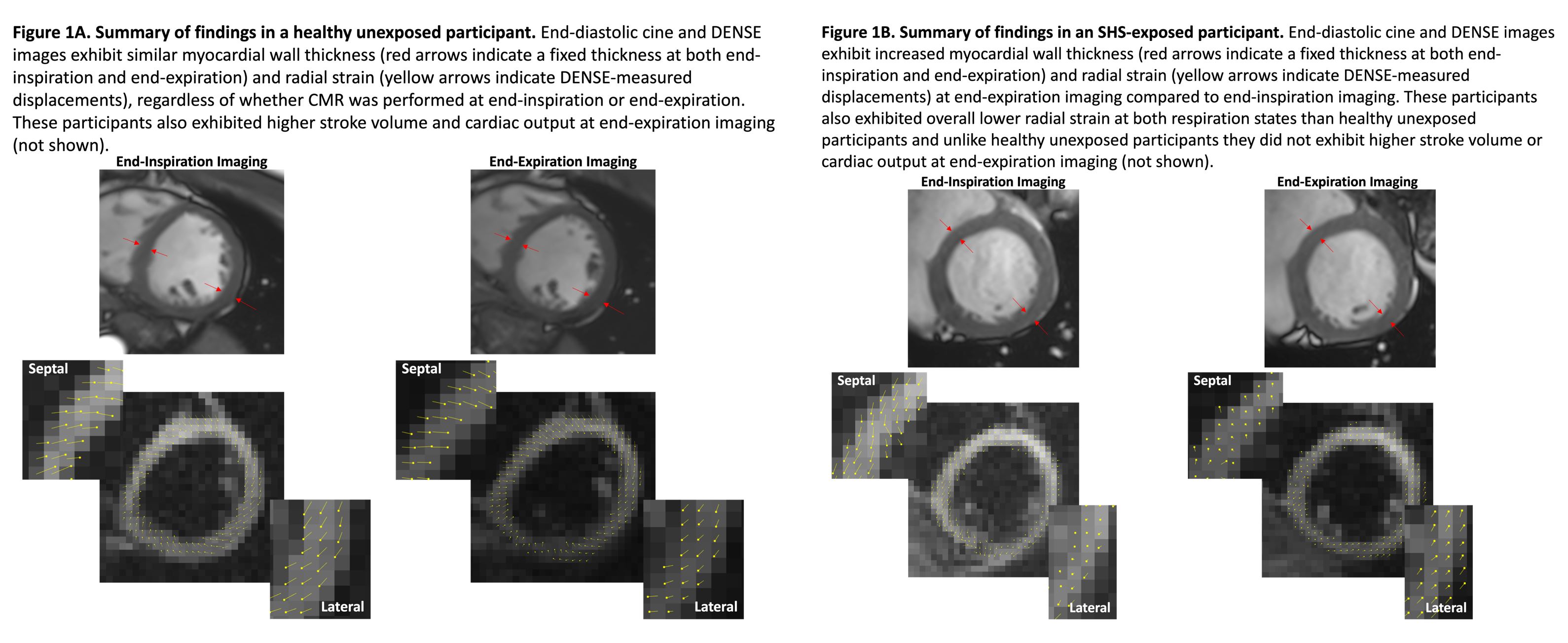
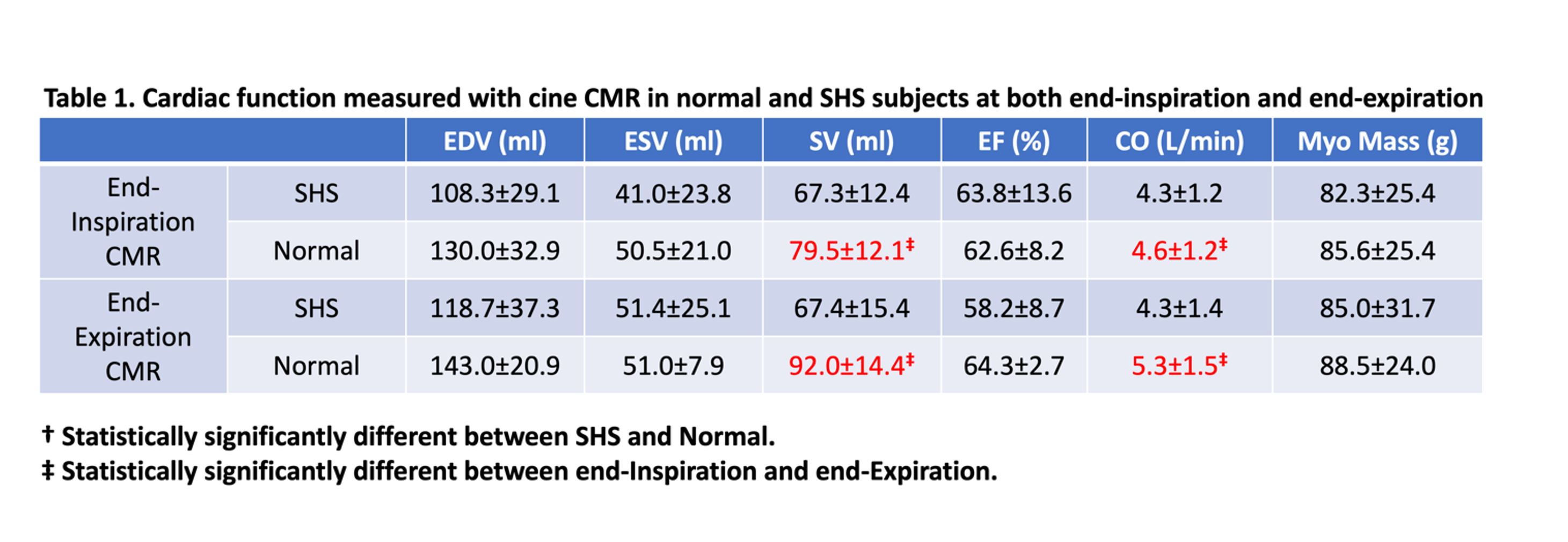
SHS-exposed versus Healthy unexposed Participants Measurements:SHS-exposed participants had a nearly significantly smaller stroke volume at end-expiration imaging than unexposed participants (SVexp=67.4±15.4 ml in exposed versus SVexp=92.0±14.4 ml in unexposed; P=0.058). No other cardiac function parameters differed between SHS-exposed and unexposed participants at either end-inspiration or end-expiration (Table 1).
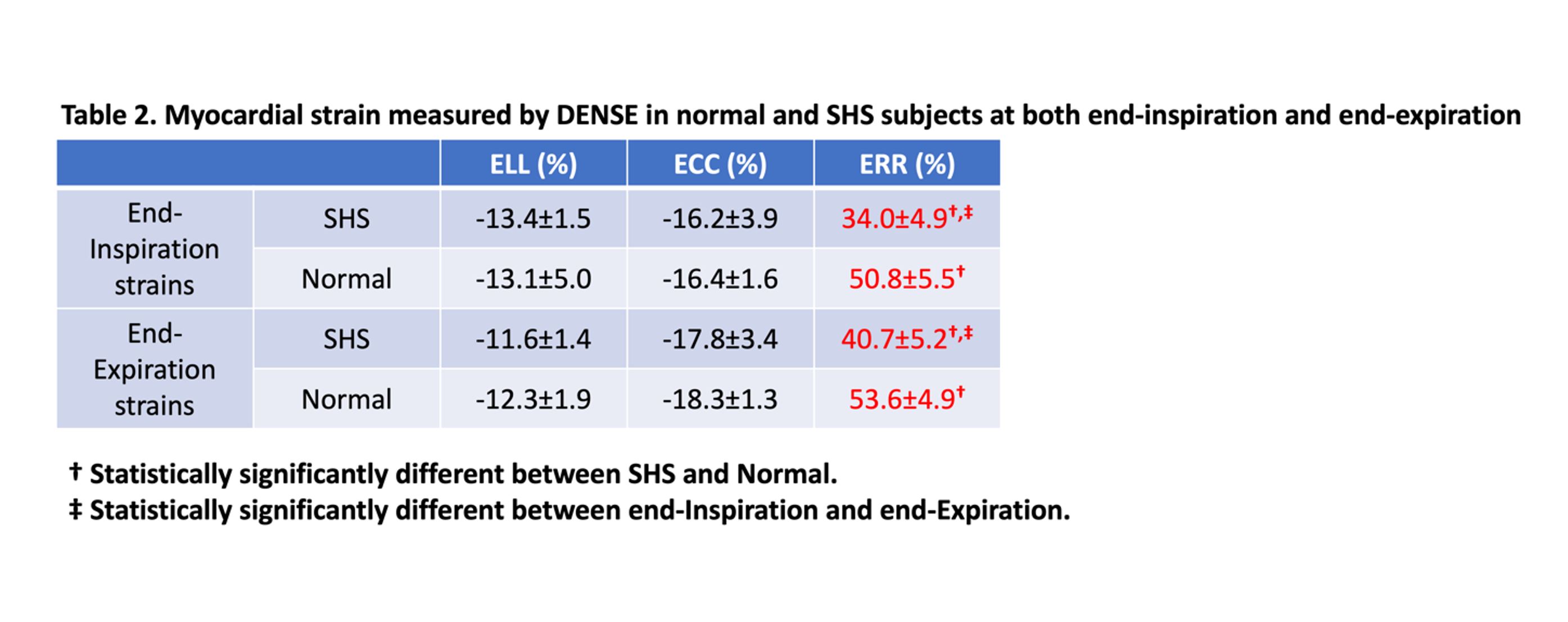
In terms of myocardial strain (Table 2), radial strain was significantly smaller in SHS-exposed (Figure 1B) than unexposed participants (Figure 1A) at both end-inspiration (ERRinsp=34.0±4.9 for exposed versus ERRinsp=50.8±5.5 for unexposed, P=0.004) and end-expiration (ERRexp=40.7±5.2 for exposed versus ERRexp=53.6±4.9 for unexposed, P=0.012). Longitudinal, circumferential and radial stretches calculated from the manual measurements of the myocardium in cine CMR followed the same trends as exhibited by DENSE strain measurements. No other differences between SHS-exposed and unexposed participants in longitudinal or circumferential strain at either end-inspiration or end-expiration was found.
End-Inspiration versus End-Expiration Measurements for SHS-exposed and Healthy Unexposed Participants:
In unexposed participants, both stroke volume and cardiac output were higher for end-expiration compared to end-inspiration imaging (SVinsp=62.6±8.2 versus SVexp=92.0±14.4 ml, P=0.022; and COinsp=4.6±1.2 versus COexp=5.3±1.5 L/min, P=0.035), with no other cardiac function parameters exhibiting a significant difference (Table 1). In contrast, in SHS-exposed participants, no difference was observed for any cardiac function parameters between end-inspiration and end-expiration, including stroke volume (SVinsp=67.3±12.4 versus SVexp=67.4±15.4 ml, P=0.982) or cardiac output (COinsp=4.3±1.2 versus COexp=4.3±1.4 L/min, P=0.904).
Longitudinal and circumferential strain did not differ between end-inspiration and end-expiration DENSE imaging for either healthy unexposed (P=0.691 for ELL and P=0.127 for ECC) or SHS-exposed participants (P=0.338 for ELL and P=0.154 for ECC; Table 2). However, while radial strain did not differ between end-inspiration and end-expiration for healthy participants as demonstrated in Figure 1A (ERRinsp=50.8±5.5% and ERRexp=53.6±4.9%, P=0.069), it markedly differed between end-inspiration and end-expiration in SHS-exposed participants as demonstrated in Figure 1B (ERRinsp=34.0±4.9% and ERRexp=40.7±5.2%, P=0.001; Table 2). Stretches calculated from manual measurements of the myocardium in cine CMR again reproduced these findings.
5. Discussion
Cardiac function does not exhibit any difference between SHS-exposed and healthy unexposed participants when measured at either end-inspiration or end-expiration by either standard cine CMR indices or DENSE longitudinal and circumferential strains, reflecting the absence of overt LV dysfunction. However, SHS-exposed participants had lower myocardial radial strain than healthy unexposed participants at both end-inspiration and end-expiration imaging.Moreover, in healthy unexposed participants, stroke volume and cardiac output were decreased when measured at end-inspiration compared to when measured at end-expiration, as often observed2, but this was not associated with any change in radial strain. In contrast, in SHS-exposed participants, neither stroke volume nor cardiac output exhibited the decrease seen in healthy participants at end-inspiration, but radial strain was significantly lower compared to end-expiration. Radial strain is known to be reduced in heart failure3.
In summary, SHS-exposed participants appear to exhibit marked differences in cardiopulmonary interactions compared to healthy unexposed participants. Cardiorespiratory interactions and their impact on cardiac function during the respiratory cycle are well-described4 and vary in different health and disease states. Our findings suggest differences exist in cardiorespiratory interactions due to SHS exposure that should be further explored to determine if they represent some form of subclinical dysfunction.
Acknowledgements
This work was supported by a research grant from the Flight Attendant Medical Research Institute (https://famri.org).References
1. Zeng S, Dunn M, Gold WM, Kizer JR, Arjomandi M. Remote exposure to secondhand tobacco smoke is associated with lower exercise capacity through effects on oxygen pulse, a proxy of cardiac stroke volume. BMJ Open Respir Res. 2022;9(1):e001217. doi:10.1136/bmjresp-2022-001217
2. Claessen G, Claus P, Delcroix M, Bogaert J, Gerche A La, Heidbuchel H. Interaction between respiration and right versus left ventricular volumes at rest and during exercise: a real-time cardiac magnetic resonance study. Am J Physiol Circ Physiol. 2014;306(6):H816-H824. doi:10.1152/ajpheart.00752.2013
3. Zhang KW, French B, May Khan A, et al. Strain Improves Risk Prediction Beyond Ejection Fraction in Chronic Systolic Heart Failure. J Am Heart Assoc. 2014;3(1). doi:10.1161/JAHA.113.000550
4. Robotham JL, Lixfeld W, Holland L, MacGregor D, Bryan AC, Rabson J. Effects of respiration on cardiac performance. J Appl Physiol. 1978;44(5):703-709. doi:10.1152/jappl.1978.44.5.703
Figures