4679
Assessment of early anthracycline-induced cardiotoxicity using segmental strain of cardiac magnetic resonance : an animal study
junqi liu1, qianfeng luo1, wanyin qi1, zhengyuan xiao1, xiaoyong zhang2, xingyuan kou1, and jing chen1
1The Affiliated Hospital of Southwest Medical University, Luzhou, China, 2Clinical Science, Philips Healthcare, Chengdu, China, Chengdu, China
1The Affiliated Hospital of Southwest Medical University, Luzhou, China, 2Clinical Science, Philips Healthcare, Chengdu, China, Chengdu, China
Synopsis
Keywords: Cardiomyopathy, Cardiomyopathy
This study investigated segmental strain to evaluate early anthracycline-induced cardiotoxicity on a 1.5T MR system in New Zealand rabbits models. The apical lateral wall and the anterior apical wall have a statistical difference corresponding to the pathological results in the second week. The ejection fraction showed statistical difference at the eighth week, while the global strain was not even statistically significant. The result showed that the peak segmental strain was earlier than the peak global strain and cardiac function, which may provide an effective and convenient monitoring method for chemotherapy patients.introduction
As one of the most effective and widely used chemotherapeutic drug groups, anthracycline antibiotics are essentially cytotoxic drugs. They inevitably cause different adverse effects while killing cancer cells, such as serious cardiotoxicity, which leads to heart failure [1,2]. The 5-year survival rate of anthracycline-induced cardiomyopathy is less than 50% [3]. Strain assessment (either ultrasonic or magnetic resonance strain) may be a promising method to evaluate subclinical myocardial dysfunction and could monitor the acute, early, and late stages of cardiotoxicity [4-8]. The focus of a study of cardiotoxicity with tissue tracking was the global peak myocardial strain, particularly global longitudinal strain (GLS), which is used to predict the occurrence of clinical events (heart failure, hospitalization, and death) [9-11]. However, cardiac movement occurs differently in each segment of the left ventricle, and global myocardial strain may lag. In addition, segmental strain is likely more sensitive than global strain, which is expected to become an early means of cardiotoxicity detection. The aim of this study was to explore the value of segmental strain by cardiac magnetic resonance (CMR) in diagnosing early cardiotoxicity.Methods
This study was approved by the institutional ethics committee. Serial CMR scans were performed on a 1.5T MR system (Achieva, Philips Medical System, Netherlands) in New Zealand rabbits (weight 2kg-3kg) at baseline (n = 15), week 2 (n = 15), week 4 (n = 9), week 6 (n = 6), and week 8 (n = 5) after each week’s anthracycline injection. The standard segmented steady-state free-precession (SSFP) cine images were acquired using the scan parameters listed as follows: TE = 1.84 ms, TR = 3.7 ms, field of view = 180 mm x 180 mm, matrix = 144 x 144, slice thickness = 5 mm, acquisition voxel size = 1.67 x 1.67 mm2, and recon voxel size = 1.25 x 1.25 mm2., 20 – 30 slices. Then, after every CMR scan for pathological comparison, one to three rabbits were killed. Cardiac functional parameters, global peak strain parameters, segmental peak strain parameters of the left ventricle, and damaged state of myocardial cells were obtained. The earliest MRI diagnostic time and parameter threshold of cardiac toxicity were analyzed by a mixed linear model and receiver operating characteristic (ROC) analysis.Results
The left ventricular ejection fraction decreased at week 8 (p < 0.05). There were no statistical differences in global strain during the experiment (p > 0.05). The peak segmental radial strain of the apical lateral wall and peak segmental circumferential strain of the anterior apical wall changed at week 2 (p < 0.05). With ROC analysis, the cutoff strain value for these two walls were 46.285 and -16.920, respectively. In addition, the respective areas under the curve (AUROC) were 0.593 and 0.764, respectively. Peak segmental longitudinal strain of the anterior apical and lateral apical wall changed relatively late in the fourth week (p < 0.05). In addition, the cutoff values were -12.415 and -15.960, respectively, and AUROC was 0.646 and 0.717, respectively. Last, myocardial injury occurred at the corresponding periods.Conclusions
The peak segmental strain of the tissue tracking technique detected anthracycline-induced cardiotoxicity earlier than peak global strain and cardiac function in the second week, based on experimental evidence.Acknowledgements
Jun-Qi Liu and Qian-Feng Luo participated in the study design, contributed to data analysis and interpretation, performed the statistical analysis, and drafted the manuscript. Jing Chen contributed to study design, and contributed to preparation, editing and review of the manuscript. Wan-Yin Qi and Zheng-Yuan Xiao contributed to quantitative data analysis and preparation of the manuscript. Xiao-Yong Zhang and Xing-Yuan Kou contributed to quality control of data and editing and review of the manuscript. All authors read and approved the final.References
[1] Yu J, Wang C, Kong Q, et al. Recent progress in doxorubicin-induced cardiotoxicity and protective potential of natural products[J]. Phytomedicine, 2018,40:125-139.[2] Kremer L C, van Dalen E C, Offringa M, et al. Anthracycline-induced clinical heart failure in a cohort of 607 children: long-term follow-up study[J]. J Clin Oncol, 2001,19(1):191-196.[3] Felker G M, Thompson R E, Hare J M, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy[J]. N Engl J Med, 2000,342(15):1077-1084.[4] Ong G, Brezden-Masley C, Dhir V, et al. Myocardial strain imaging by cardiac magnetic resonance for detection of subclinical myocardial dysfunction in breast cancer patients receiving trastuzumab and chemotherapy[J]. Int J Cardiol, 2018,261:228-233.[5] Houbois C P, Nolan M, Somerset E, et al. Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer: Comparison With Echocardiography[J]. JACC Cardiovasc Imaging, 2021,14(5):962-974.[6] Scatteia A, Baritussio A, Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance[J]. Heart Fail Rev, 2017,22(4):465-476.[7] Thavendiranathan P, Negishi T, Somerset E, et al. Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy[J]. J Am Coll Cardiol, 2021,77(4):392-401.[8] Egashira K, Sueta D, Tomiguchi M, et al. Cardiac computed tomography-derived extracellular volume fraction in late anthracycline-induced cardiotoxicity[J]. Int J Cardiol Heart Vasc, 2021,34:100797.[9] Fischer K, Obrist S J, Erne S A, et al. Feature Tracking Myocardial Strain Incrementally Improves Prognostication in Myocarditis Beyond Traditional CMR Imaging Features[J]. JACC Cardiovasc Imaging, 2020,13(9):1891-1901.[10] Wang R, Zhou Z, Schoepf U J, et al. Monitoring of anthracycline-induced myocardial injury using serial cardiac magnetic resonance: An animal study[J]. Int J Cardiol, 2021,328:111-116.[11] Houbois C P, Nolan M, Somerset E, et al. Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer: Comparison With Echocardiography[J]. JACC Cardiovasc Imaging, 2021,14(5):962-974.Figures
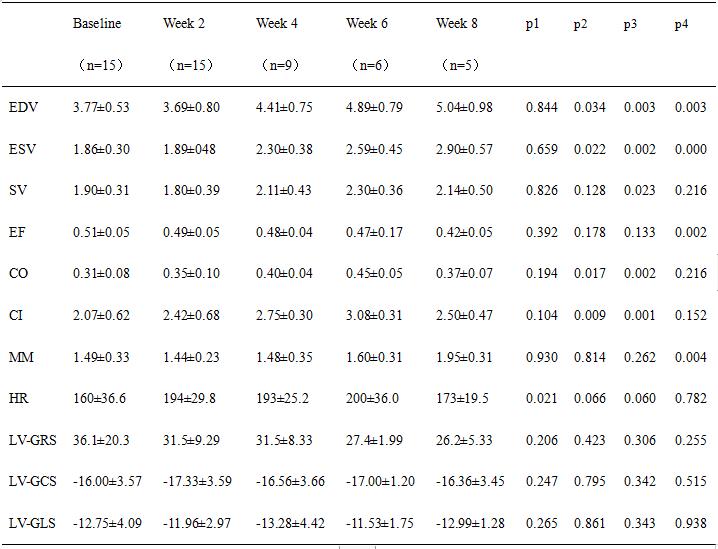
Values are means ± SD, p1 = p of baseline and week 2, p2 = p of baseline and week 4, p3 = p of baseline and week 6, p4 = p of baseline and 8 week
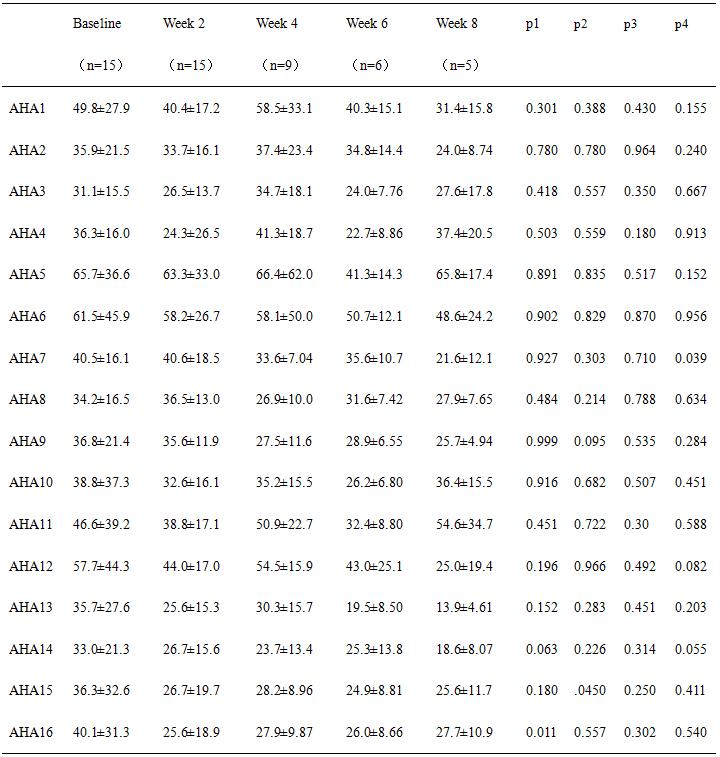
Values are means ± SD, p1 = p of baseline and week 2, p2 = p of baseline and week 4, p3 = p of baseline and week 6, p4 = p of baseline and week 8. AHA1 = basal anterior, AHA2 = basal anteroseptal, AHA3 = basal inferoseptal, AHA4 = basal inferior, AHA5 = basal inferolateral, AHA6 = basal anterolateral, AHA7 = mid anterior, AHA8 = mid anteroseptal, AHA9 = mid anteroseptal, AHA10 = mid inferior, AHA11 = mid inferolateral, AHA12 = mid anterolateral, AHA13 = apical anterior, AHA14 = apical septal; AHA15 = apical inferior, AHA16=apical lateral.
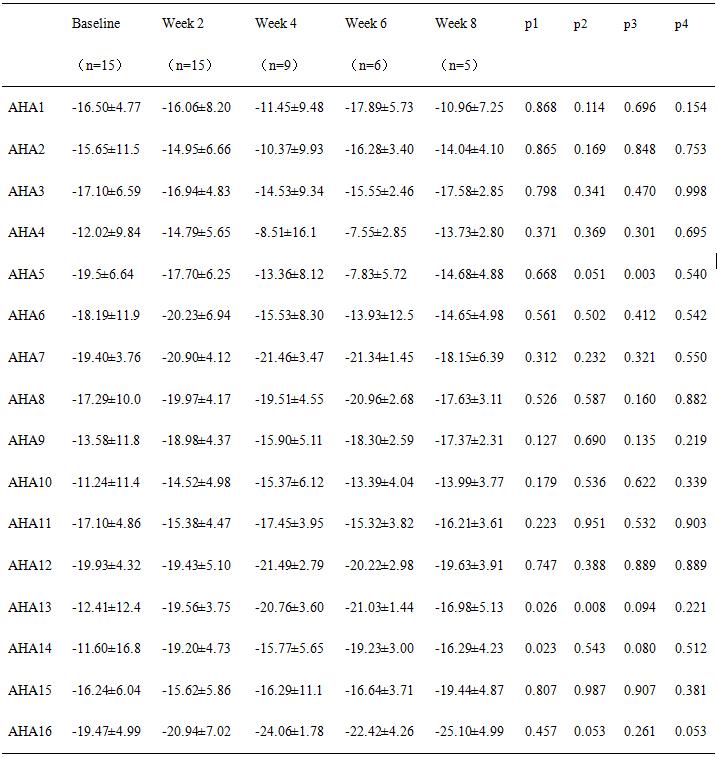
Values are means ± SD, p1 = p of baseline and week 2, p2 = p of baseline and week 4, p3 = p of baseline and week 6, p4 = p of baseline and 8 week
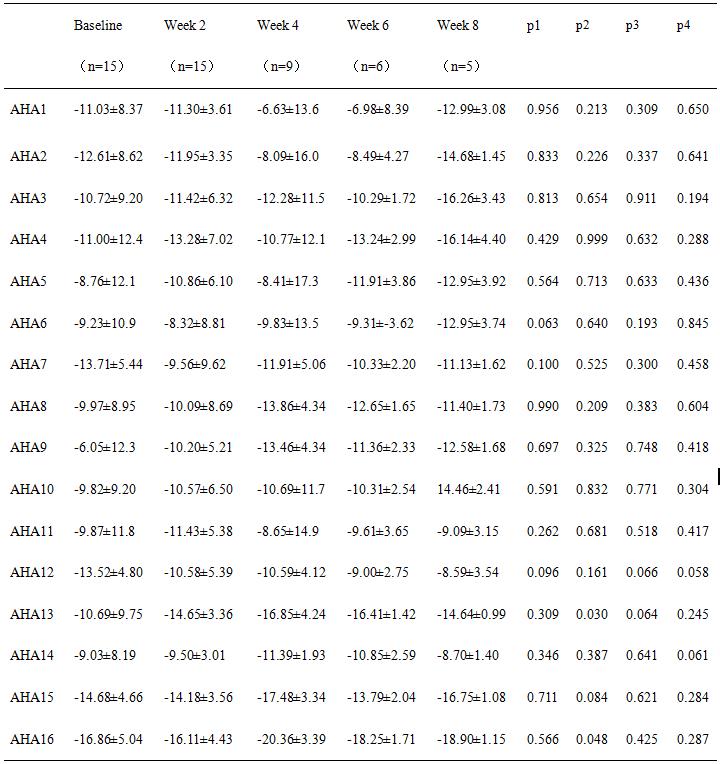
Values are means ± SD, p1 = p of baseline and week 2, p2 = p of baseline and week 4, p3 = p of baseline and week 6, p4 = p of baseline and 8 week
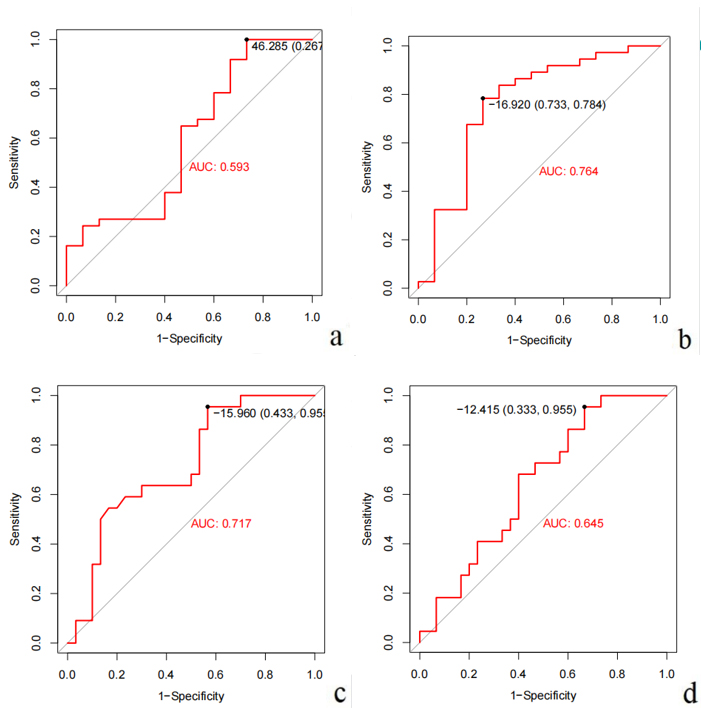
Receiver operating characteristic (ROC) curves for diagnosis. The area under the ROC curves (AUC) for AHA16 at week 2 in peak segmental radial strain was 0.593 (Panel 1). AUC for AHA13 at week 2 in peak segmental Circumferential Strain was 0.764 (Panel 2). AUC for AHA16 at week 4 in peak segmental longitudinal strain was 0.717 (Panel 3). AUC for AHA13 at week 4 in peak segmental longitudinal strain was 0.645 (Panel 4).
DOI: https://doi.org/10.58530/2023/4679