4677
Application of CMR-FT technique in the assessment of cardiac function and prognosis in patients with myocardial amyloidosis
Jianing Cui1, Tao Li1, Xiuzheng Yue2, and Chuncai Luo1
1Radiology, the First Medical center, PLA General Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
1Radiology, the First Medical center, PLA General Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Heart, MR Value, cardiac magnetic resonance-feature tracking
Early diagnosis of cardiac amyloidosis (CA) and accurate assessment of cardiac function is important for CA patients. LV strain and strain rate obtained by cardiac magnetic resonance-featured tracking (CMR-FT) have been developed as sensitive indicators of myocardial function. This study aimed to evaluate myocardial function in patients with CA by strain and strain rate to assess their prognostic value in patients with CA. Our data showed that strain rate could be used to assess the degree of cardiac impairment in CA and the difference with HCM providing prognostic information for all-cause mortality in CA patients.Introduction
Cardiac amyloidosis (CA) is a form of restrictive cardiomyopathy due to abnormal amyloid deposition in the heart 1. The diagnosis of CA should be difficult due to the presence of left ventricular (LV) myocardial hypertrophy in both CA and hypertrophic cardiomyopathy (HCM). Therefore, early diagnosis of CA and accurate assessment of cardiac function are important for patients with CA2. Recently, LV strain and strain rate obtained by cardiac magnetic resonance-featured tracking (CMR-FT) have been developed as sensitive indicators of myocardial function. CMR-FT has been used to assess myocardial function in patients with CA3. Until now, studies regarding relationship between myocardial strain rate and all-cause mortality in patients with CA are lacking. This study aimed to evaluate myocardial function in patients with CA and HCM by strain and strain rate, assessing their prognostic value in patients with CA.Materials and Methods
Thirty-one patients with CA (mean age: 54±11 years, 20 males) who underwent CMR scanning on 1.5-T scanners(Multiva, Philips Healthcare, Netherlands) at our hospital were retrospectively collected from March 2013 to June 2021. Comparisons were made with 31 age and gender-matched patients with HCM (mean age: 55±12 years, 22 males) and 31 normal controls (NC) (mean age: 54±11 years, 20 males). Cardiac function was evaluated by balanced turbo field echo (BTFE) cine sequence at the continuous short-axis covering the whole LV and the long-axis (2/3/4 chamber) views under breath-holding. Imaging parameters included TR/TE 3.7/1.8ms, in-plane resolution 1.4 × 1.4mm2, flip angle 60° and slice thickness 8mm with 8 to 12 slices gathered on the short-axis. The parameters of LV volumes and function were calculated using CVI42 (Circle Cardiovascular Imaging, Calgary, Canada), including LV end-diastolic volume (LVEDV), LV end-systolic volume (LVESV), LV ejection fraction (LVEF), LV systolic myocardial mass (LVSMM)、LV diastolic myocardial mass(LVDMM), and cardiac output (CO). Radial, circumferential and longitudinal strains and strain rates of LV at global and each myocardial segment (basal, middle, and apical) were obtained with the CMR-FT technique, and the differences in parameters among 3 groups were analyzed. Clinical follow-ups were initiated from the CMR scan. The primary outcome was defined as all-cause death. The predictive value of myocardial strains and strain rates on all-cause mortality in CA patients was analyzed with the stepwise COX regression model.Results
The differences in left ventricular volume, myocardial mass, ejection fraction, and cardiac output were statistically significant in all three groups (P < 0.05). Except for the apical longitudinal strain, global and segmental strains were significantly lower in the CA group than in the HCM group (P < 0.05). The global and segmental strains were significantly lower in the CA group than in the NC group (P < 0.05). The basal strain rates in three directions were significantly lower in the CA group than in the NC group (P< 0.05), but the difference in apical strain rates between the two groups was not statistically significant. Multivariate stepwise COX analysis showed that troponin T (HR = 1.05, 95% CI: 1.01-1.10, P = 0.017) and middle peak diastolic circumferential strain rate (HR = 6.87, 95% CI: 1.52-31.06, P = 0.012) were strong predictors of death.Discussion
In the present study, we found that the global and all segmental strain rates in three directions were significantly lower in the CA group compared with the NC group. The global and all segmental longitudinal strain rate were significantly lower in the HCM group compared with the NC group, indicating that myocardial function was reduced in both the CA and HCM groups. In addition, the basal strain rates in three directions were significantly lower in the CA group compared with the NC group, but the number of strain rates that were significantly different between the two groups gradually decreased from the base to the apex of LV, indicating that the severity of impaired myocardial function in the CA group gradually decreased from the base to the apex of LV. For the clinic, the prognosis of patients with CA is often a major concern. In our study, troponin T and middle peak diastolic circumferential strain rate were independent predictors of death even after adjustment for other parameters. A previous study reported that the contraction of subendocardial fibers of the myocardium contributes to longitudinal shortening, while the contraction of subepicardial fibers contributes to circumferential shortening, both of which lead to radial thickening4. Amyloid deposition tends to move from the endocardium to the epicardium 5, so decreased circumferential strain rate represents whole myocardial injury, suggesting a poor prognosis.Conclusions
Strain and strain rate parameters derived from CMR-FT based on cine sequences are new noninvasive imaging markers that can be used to assess the degree of cardiac impairment in CA and the difference in cardiac function with HCM providing independent prognostic information for all-cause mortality in CA patients.Acknowledgements
No acknowledegments in this abstract.References
[1]Esplin BL, Gertz MA. Current trends in diagnosis and management of cardia camyloidosis[J]. Curr Probl Cardiol, 2013;38(2):53-96. [2] Wan K, Sun J, Yang D, et al. Left Ventricular Myocardial Deformation on Cine MR Images: Relationship to Severity of Disease and Prognosis in Light-Chain Amyloidosis[J]. Radiology. 2018;288(1):73-80. [3]Jung HN, Kim SM, Lee JH, et al. Comparison of tissue tracking assessment by cardiovascular magnetic resonance for cardiac amyloidosis and hypertrophic cardiomyopathy. Acta Radiol. 2020 Jul;61:885-893. [4]Claus P, Omar AMS, Pedrizzetti G, et al. Tissue Tracking Technology for Assessing Cardiac Mechanics: Principles, Normal Values, and Clinical Applications[J]. JACC Cardiovasc Imaging 2015; 8(12):1444–1460. [5]Li R, Yang ZG, Xu HY, et al. Myocardial Deformation in Cardiac Amyloid Light-chain Amyloidosis: Assessed with 3T Cardiovascular Magnetic Resonance Feature Tracking[J]. Sci Rep. 2017;7(1):3794. Published 2017 Jun 19.Figures
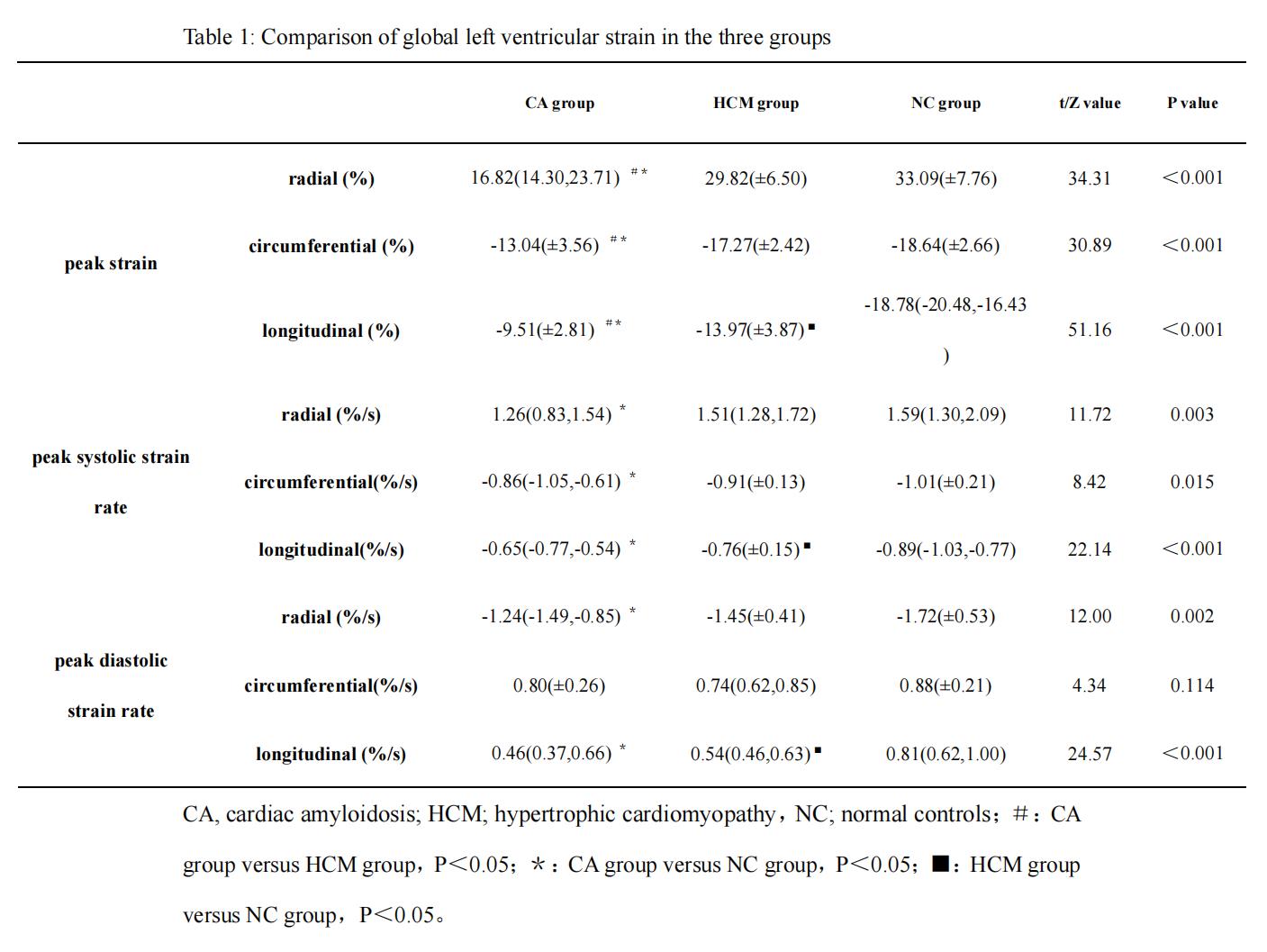
Table 1: Comparison of global
left ventricular strain in the three groups
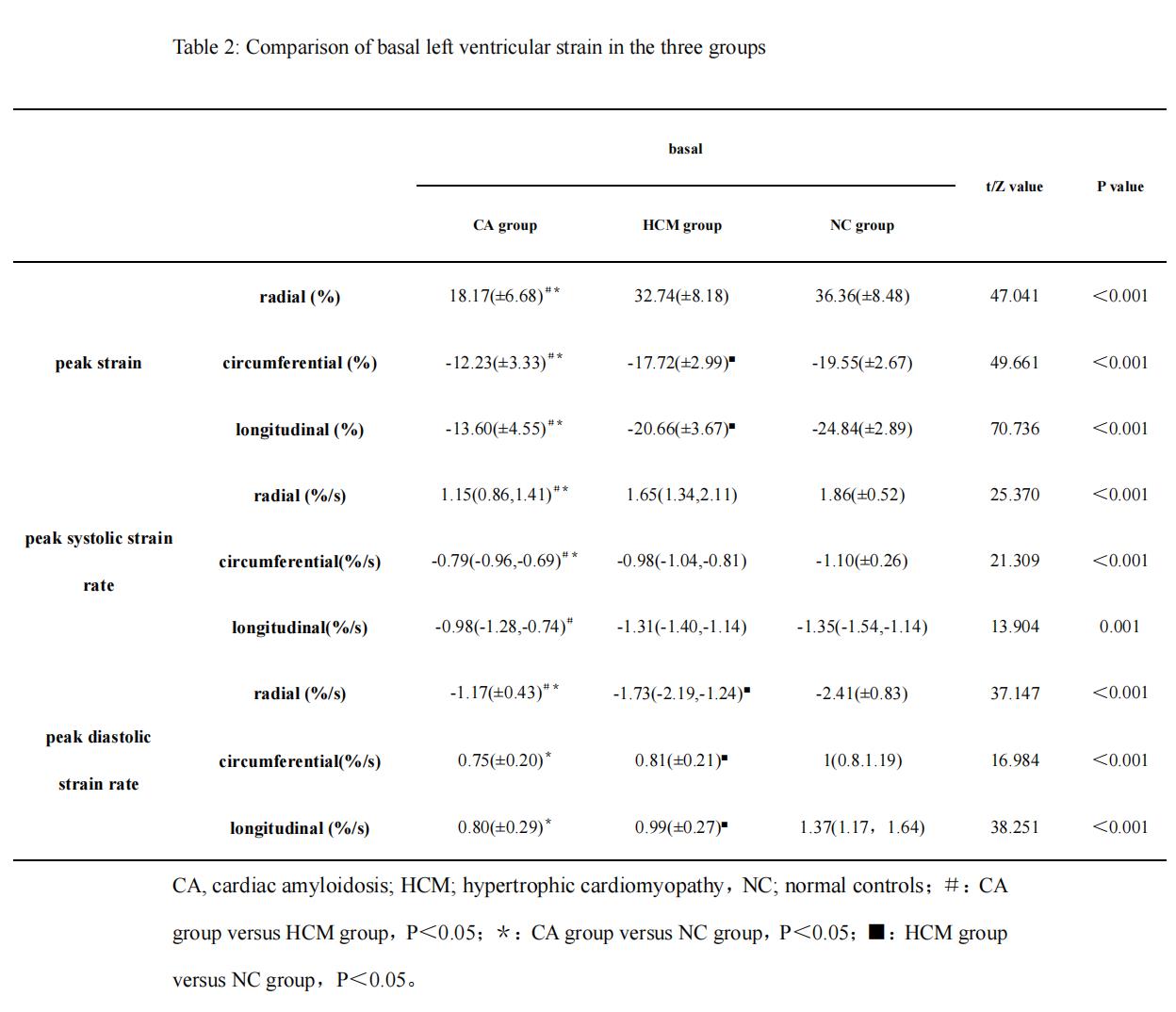
Table 2: Comparison of basal
left ventricular strain in the three groups
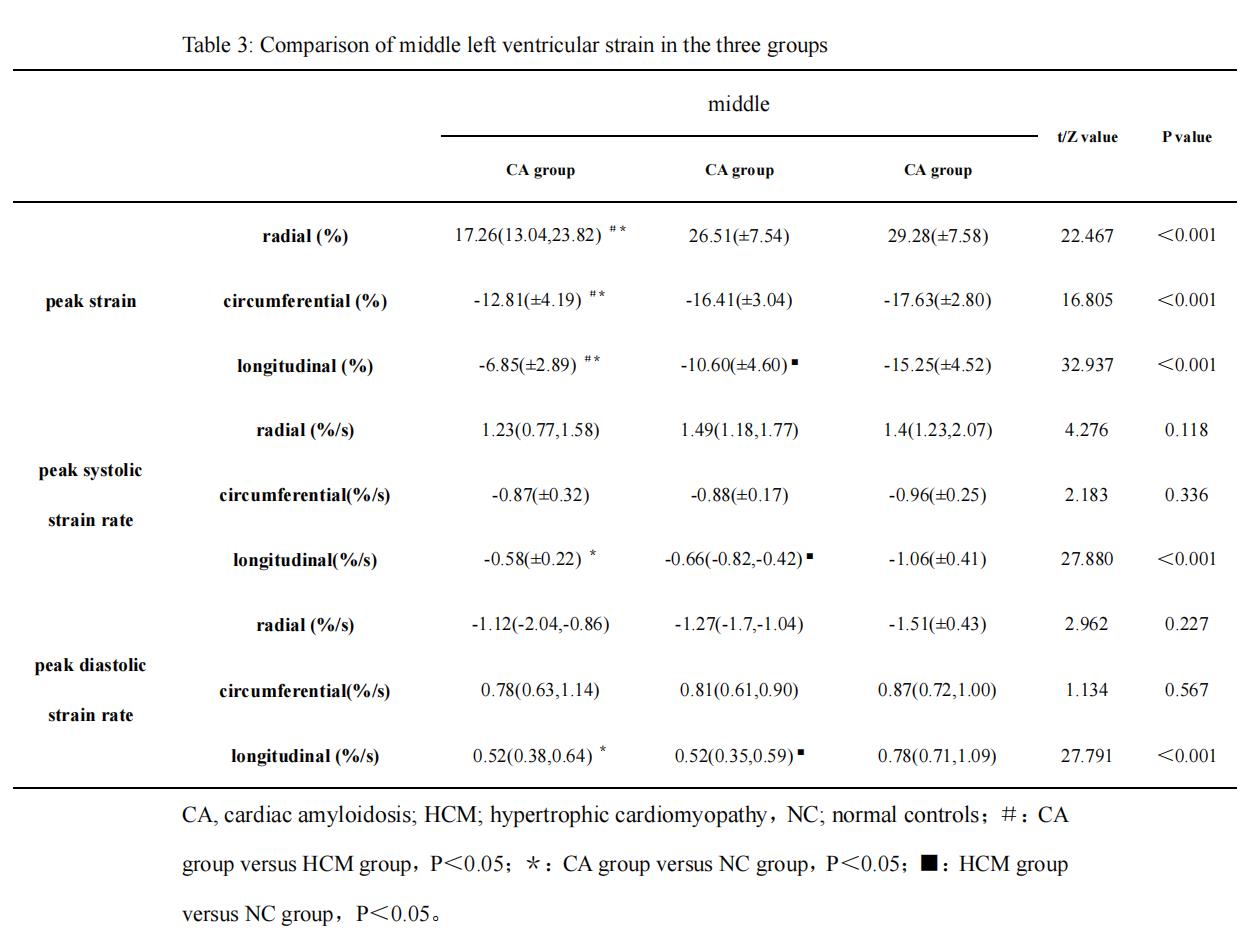
Table 3: Comparison of middle
left ventricular strain in the three groups
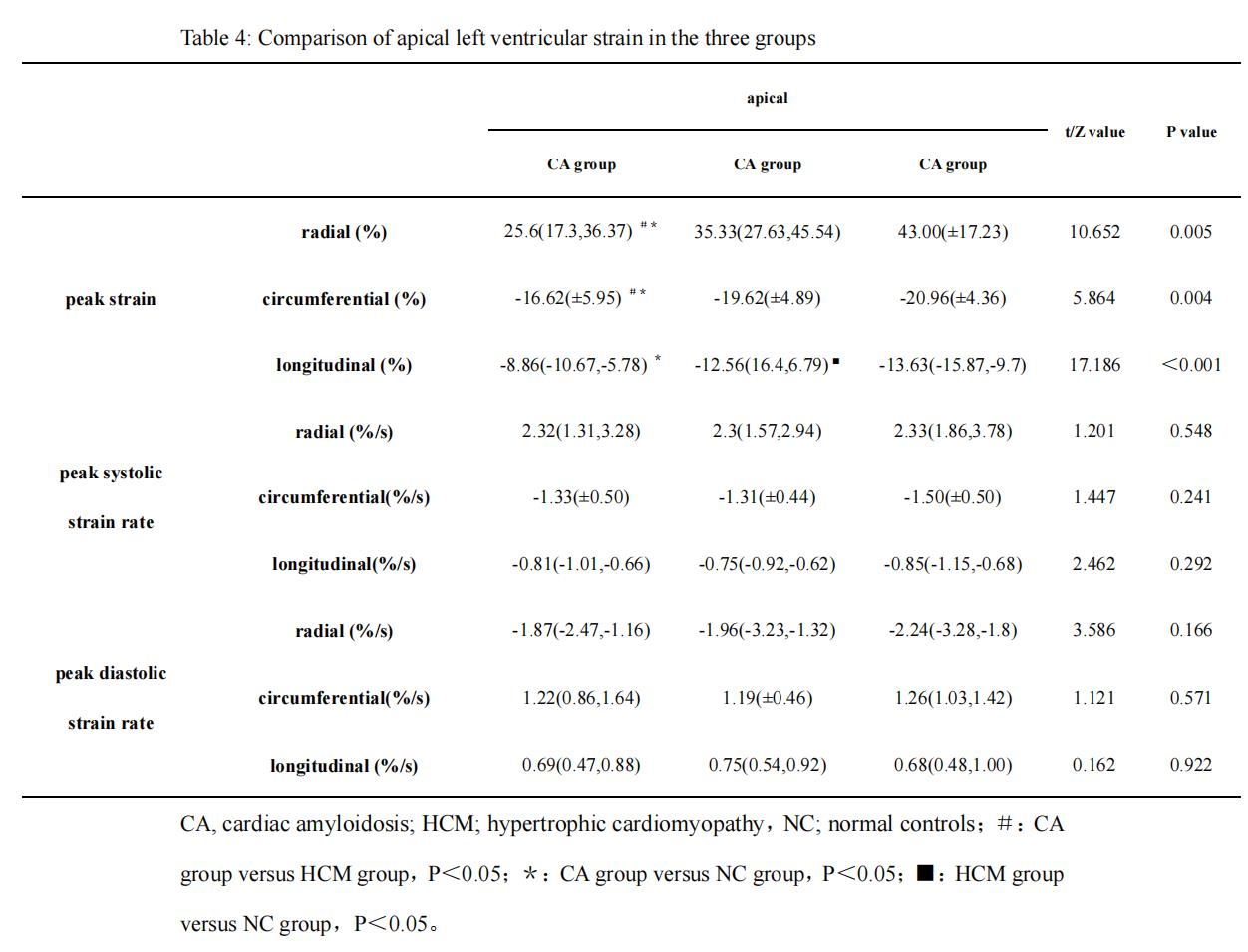
Table 4: Comparison of apical
left ventricular strain in the three groups
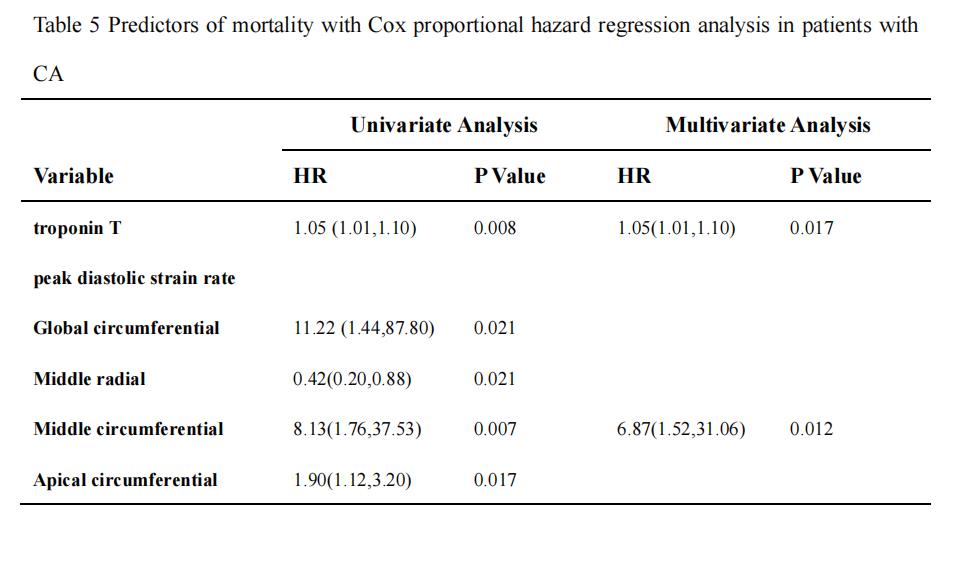
Table 5 Predictors of
mortality with Cox proportional hazard regression analysis in patients with CA
DOI: https://doi.org/10.58530/2023/4677