4675
The value of CMR feature tracking (FT) technique in quantitative assessment of left ventricular myocardial strain in cardiac amyloidosis (CA)
Jia Liu1, Jianxing Qiu1, Wei Li1, Jiangkai He1, Kai Zhao1, and Jianxiu Lian2
1Peking University First Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
1Peking University First Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular, Cardiac magnetic resonance,Feature tracking,Strain,Cardiac amyloidosis
Subjects were divided into light-chain amyloidosis (AL-CA), transthyretin-related amyloidosis (ATTR-CA) and control group. CMR-FT technique was used to measure apical, middle and basal strain of left ventricle. Results showed ICC value was higher than 0.9 in all strain parameters, and meanwhile all strain parameters in AL-CA group and ATTR-CA group were lower than those in control group except for apical RS. However, there was no statistical difference between the AL-CA group's and ATTR-CA group. Strain evaluation could evaluate patients of CA, which may provide evidence for the treatment and diagnosis of CA.Introduction
The etiology, diagnosis methods, treatment strategies and prognosis of the two types of cardiac amyloidosis (CA) are quite different in clinical practice, including light-chain amyloidosis(AL-CA) and transthyretin-related amyloidosis (ATTR-CA). Therefore, early diagnosis and classification of CA are of great significance for guiding follow-up treatment and prognosis evaluation1-3. Cardiovascular magnetic resonance (CMR) plays an important role in noninvasive diagnosis of CA, which could offer structure and function parameters. CA patients often show restrictive dysfunction with preserved ejection fraction (EF). However, traditional CMR technology is not enough to quantitative patients' myocardial diastolic function. CMR-FT technology can achieve myocardial strain measurement in recent years, which have higher accuracy than ultrasonic speckle tracking imaging technology5. It is expected to use CMR-FT for early diagnosing and evaluating CA without contrast agent4-7. The objective of this study is to explore the value of CMR-FT in quantitative assessment of left ventricular myocardial strain in patients with CA and further distinguish AL-CA and ATTR-CA.Methods
A total of 20 cardiac light-chain amyloidosis patients (AL-CA group, 15 males, mean age: 31∽75years), 20 cardiac transthyretin-related amloidosis patients (ATTR-CA group, 16 males, mean age: 31∽68 years) diagnosed by pathology in the Peking University First Hospital from April 2016 to March 2022 and 20 healthy subjects (control group). All participants underwent 3.0T CMR examination (Ingenia CX, Philips Healthcare, the Netherlands) with 32-channel abdominal coil. The sequence of steady-state free precession (SSFP) cines were performed for CMR-FT assessment. Scan parameters were as follows: TR=45.6 ms , TE=1.4 ms , field of view (FOV)=340×340 mm , slice thickness=8 mm, voxel size=1.6×1.6×8 mm3. CMR-FT technique was used to measure 3-dimensional(3D) basal, mid-cavity, apical and global myocardium longitudinal strain (LS), circumferential strain(CS)and radial strain (RS)of left ventricle with CVI 42.0(version 5.11,Circle Cardiovascular Imaging,Calgary,Canada)as shown in Figure 1 and 2. The SPSS26.0 and Medcalc 20.0 software were used to calculate statistical results. Intra-observer agreement was also assessed by intraclass correlation coefficient (ICC). ANOVA and Bonferroni post hoc comparisons were used to explore differences among different groups’s strain parameters. P<0.05 was considered as significantly different.Results
The intraclass coefficient (ICC) value was higher than 0.9 in all strain parameters as shown in Table 1, and the Bland-Altman analysis results were shown in Figure 3. As shown in Table 2, the results of CMR-FT strain analysis showed that all strain parameters in AL-CA group and ATTR-CA group were lower than those in control group (P < 0.05) except for apical RS. However, there was no statistical difference between the AL-CA group's strain parameters and the ATTR-CA group (P > 0.05).Discussion
Feature tracking technology were used for evaluating cardiac amyloidosis (CA) in this study. Results showed that the repeatability of myocardial strain parameters achieved excellent agreement. And there were significant differences between normal and CA patients, but no difference showed between AL-CA and ATTR-CA. The consistency analysis of measurement data from different observers has always been a concern of imaging, and is also the basis for the application of certain image signs or parameters. Based on the data of myocardial strain parameters measured by two observers, this study used ICC values and the Bland Altman method to evaluate the consistency between the two observers. In this study, the average difference range of CS values measured by two observers was consistent and acceptable. All of the measured myocardial strain parameters have ICC values>0.9, which can fully meet the requirements of diagnosis and differential diagnosis.The typical features of CA in echocardiography include the relative apical preservation mode of LS, which can help differentiate from other cardiac hypertrophy diseases8, and CMR can also repeat similar results9 which is similar to our resluts. In other studies, LGE was used as the gold standard and CS value was used as the diagnostic index for 61 CA patients. The results showed that the sensitivity, specificity and accuracy reached 93.8%, 69.2% and 88.5% respectively, suggesting that CS also has a high reference value for the diagnosis of CA10. Therefore, myocardial strain should be considered as an important content in the assessment of myocardial function of patients with CA (especially subclinical CA). Our study showed that all strain parameters in AL-CA group and ATTR-CA group were lower than those in control group except for apical RS. However, there was no statistical difference between the AL-CA group's strain parameters and the ATTR-CA group. Maybe we should increase our sample size to investigate the difference between two types of CA further.Conclusion
There is good intra-observer agreement of CMR-FT strain parameters, and therefore this method is feasible. CMR has certain value in quantitative assessment of left ventricular myocardial strain in CA.Acknowledgements
No acknowledgement found.References
[1] Gertz MA, Dispenzieri A. Systemic amyloidosis recognition, prognosis, and therapy: a systematic review [J]. JAMA, 2020, 324:79-89. [2] Ruberg FL, Maurer MS, Judge DP, et al. Prospective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the transthyretin amyloidosis cardiac study (TRACS) [J]. [3] Rubin J, Maurer MS. Cardiac amyloidosis: overlooked, underappreciated, and treatable [J]. Annu Rev Med, 2020, 71(1): 203-219. [4] Xia H, Yeung DF, Di Stefano C, et al. Ventricular strain analysis in patients with no structural heart disease using a vendor-independent speckle-tracking software[J]. BMC Cardiovasc Disord, 2020, 20(1): 274. [5] Pedrizzetti G, Claus P, Kilner PJ, et al. Principles of cardiovascular magnetic resonance feature tracking and echocardiographic speckle tracking for informed clinical use[J]. J Cardiovasc Magn Reson, 2016, 18(1): 51. [6] Smiseth OA, Torp H, Opdahl A, et al. Myocardial strain imaging: how useful is it in clinical decision making[J]. Eur Heart J, 2016, 37: 1196-1207. [7] Marwick TH, Shah SJ, Thomas JD. Myocardial strain in the assessment of patients with heart failure: a review [J]. JAMA Cardiol, 2019, 4:287-294. [8]Phelan D, Collier P, Thavendiranathan P, et al. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart, 2012, 98: 1442–1448. [9]Quarta CC, Solomon SD, Uraizee I et al. Left Ventricular Structure and Function in TTR-Related versus AL Cardiac Amyloidosis. Circulation, 2014, 129(18):1840-1849. [10] Oda S, Utsunomiya D, Nakaura T, et al. Identification and Assessment of Cardiac Amyloidosis by Myocardial Strain Analysis of Cardiac Magnetic Resonance Imaging[J]. Circ J, 2017, 81(7):1014-1021. [11] Wan K, Sun J, Yang D, et al. Left ventricular myocardial deformation on cine MR images: relationship to severity of disease and prognosis in light-chain amyloidosis [J]. Radiology, 2018, 288:73-80.Figures
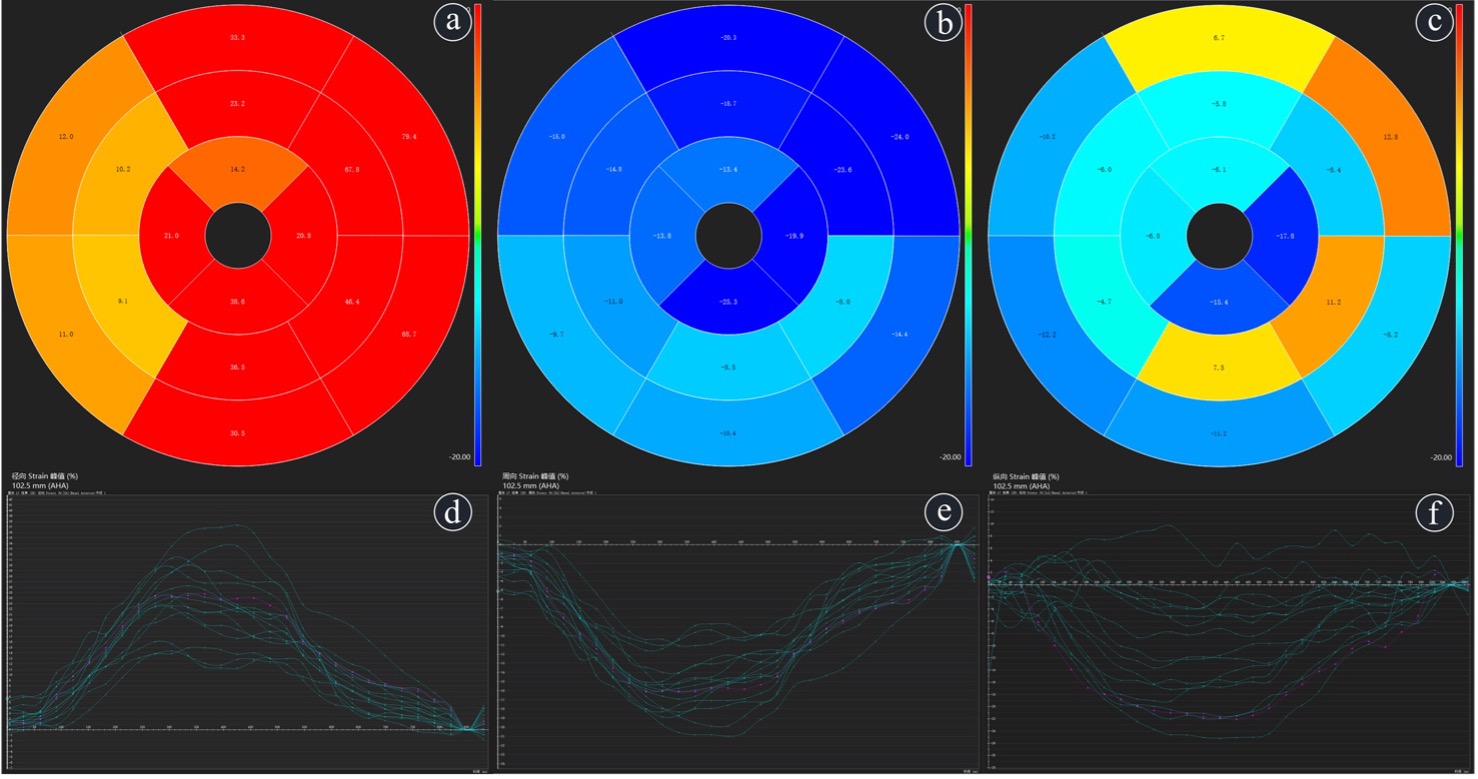
Figure 1 16 segment bull eye diagrams and myocardial strain curves of an ATTR-CA case, male, 34 years old. a~c RS、CS、LS’s 16 segment bull eye diagrams respectively;d~f correspongding RS、CS、LS’s myocardial strain curves.
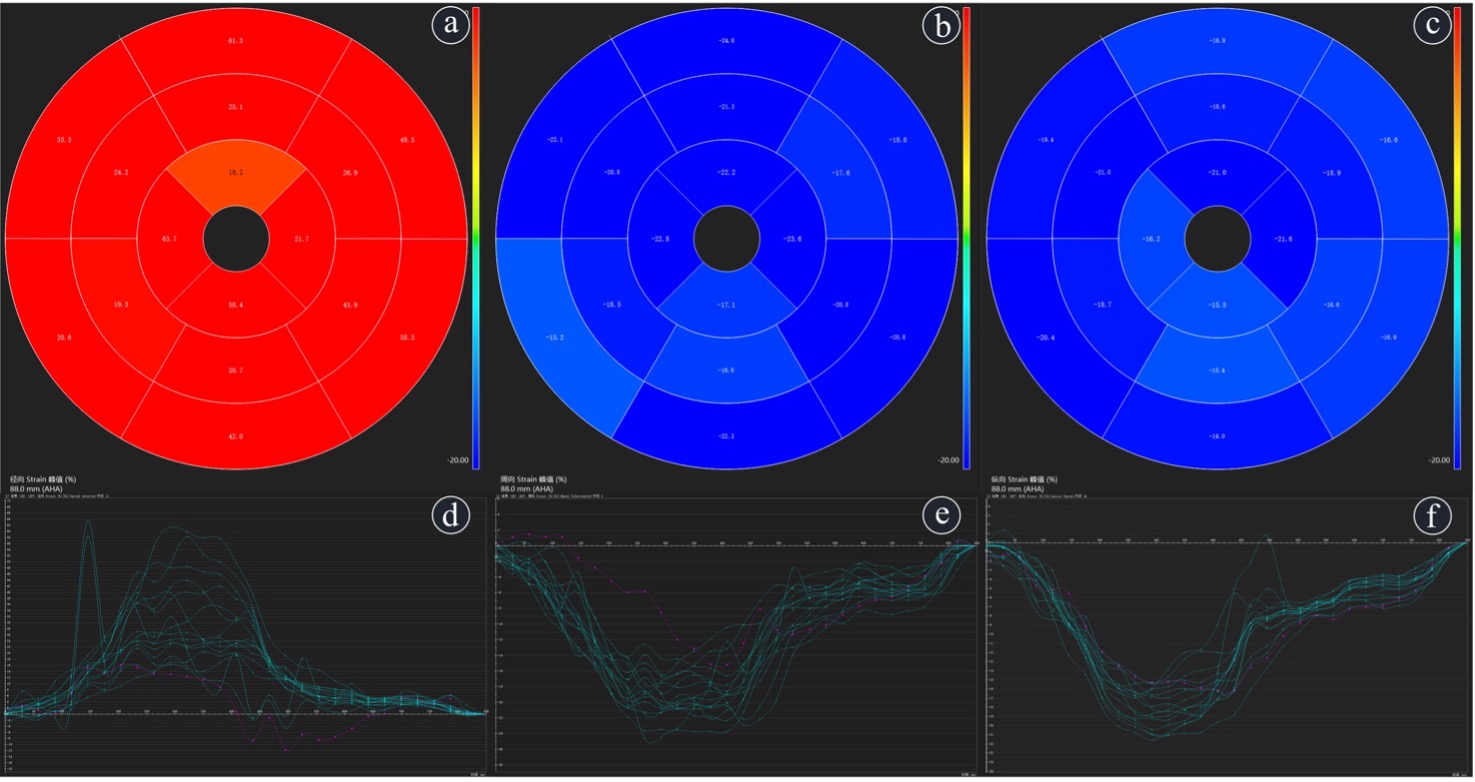
Figure 2 16 segment bull eye diagrams and myocardial strain curves of a normal control case, male, 54 years old. a~c RS、CS、LS’s 16 segment bull eye diagrams respectively;d~f corresponding RS、CS、LS’s myocardial strain curves.
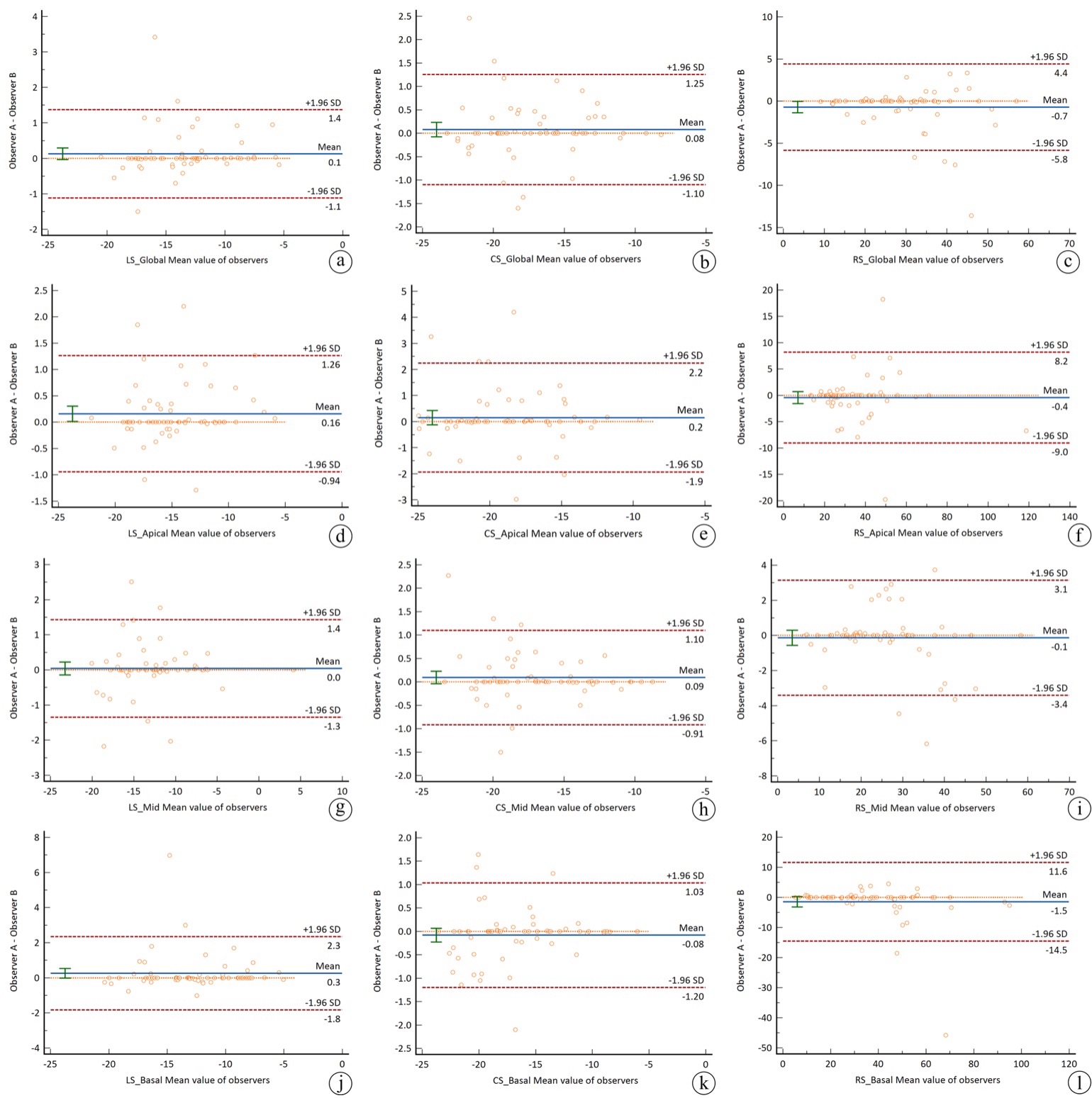
Figure 3 intra-observer agreement of all myocardial strain parameters of left ventricular a∽c. Bland-Altman of LS_Global、CS_Global、RS_Global;d∽f. Bland-Altman of LS_Apical、CS_ Apical、RS_ Apical;g∽i. Bland-Altman of LS_Mid、CS_ Mid、RS_ Mid;j∽l. Bland-Altman of LS_Basal、CS_ Basal、RS_Basal (the solid line means the average of the difference between the two observers, the dotted line means 95%CI of the difference between the two observers, the distance between the dot to the solid line means the difference between the two observers, X-axis means the average values.
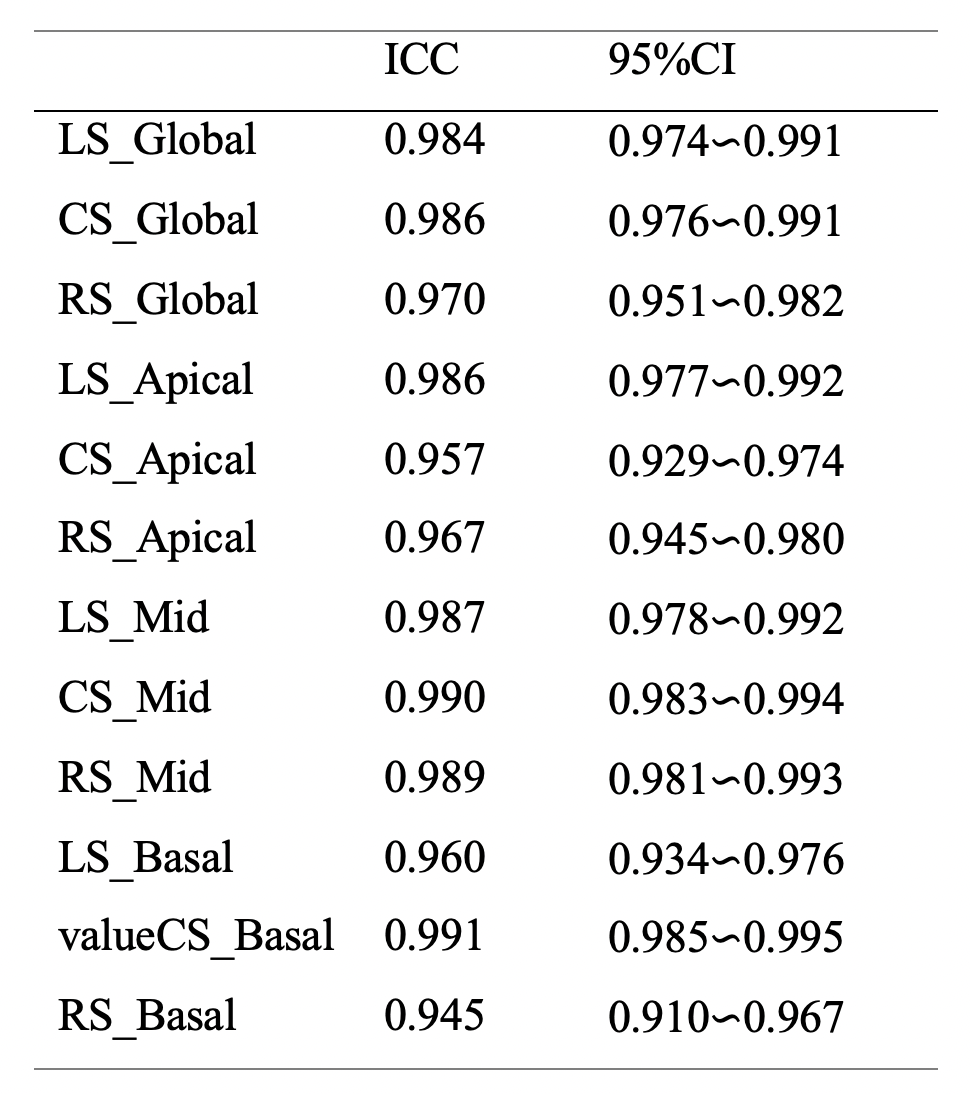
Table 1 intra-observer agreement of all myocardial strain parameters of left ventricular
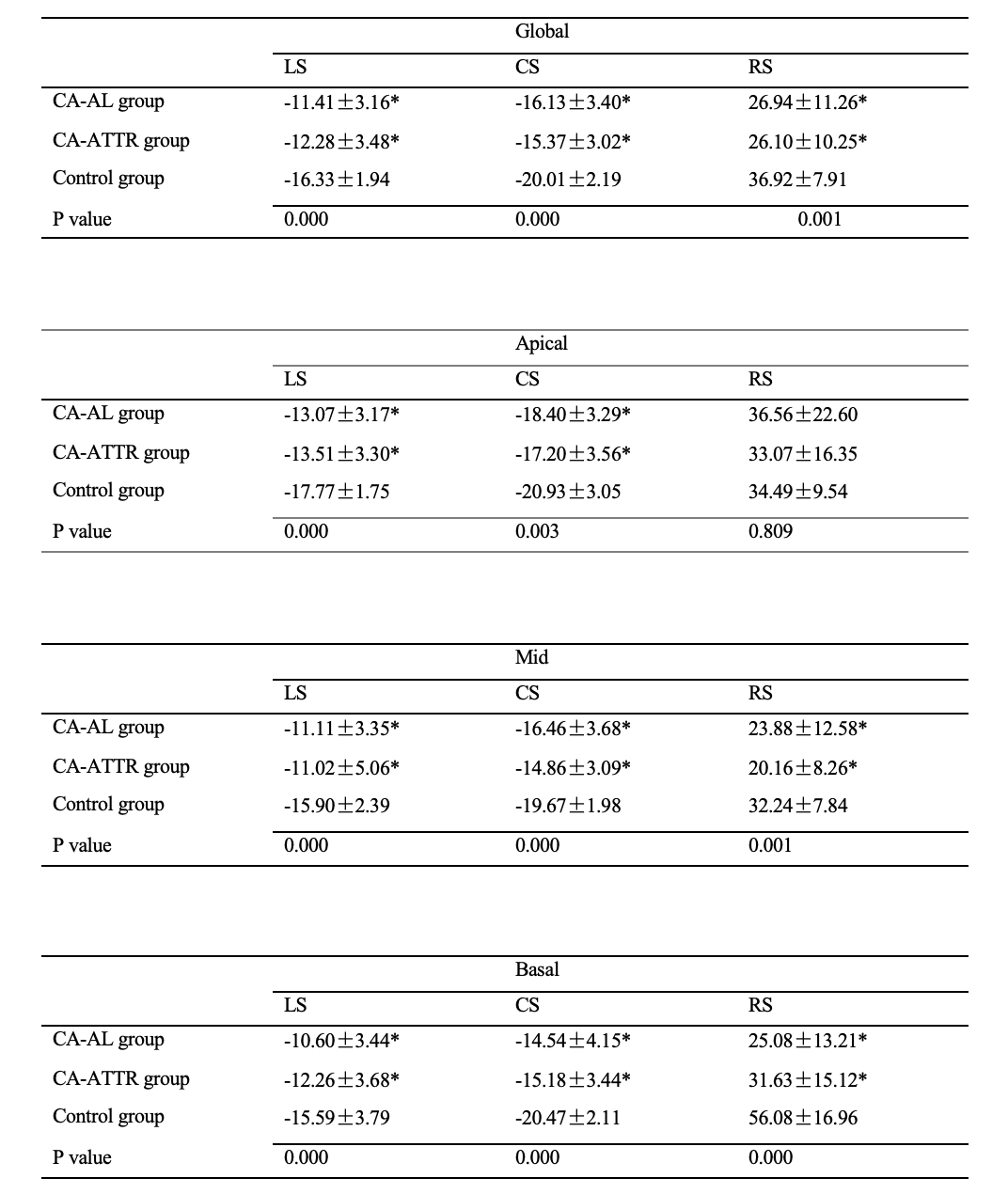
Table 2 the differences among the three groups’s strain parameters
DOI: https://doi.org/10.58530/2023/4675