4658
Motion-resolved pulmonary imaging for simultaneous fractional ventilation and T1 mapping using MR Multitasking
Chaowei Wu1,2, Hsu-Lei Lee1, Nan Wang1,3, Fei Han4, Vibhas Deshpande5, Andreas Voskrebenzev6, Jens Vogel-Claussen6, Anthony G Christodoulou1,2, Yibin Xie1, and Debiao Li1,2
1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Radiology Department, Stanford University, Stanford, CA, United States, 4Siemens Healthcare, Los Angeles, CA, United States, 5Siemens Healthcare, Austin, TX, United States, 6Institute for Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany
1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Radiology Department, Stanford University, Stanford, CA, United States, 4Siemens Healthcare, Los Angeles, CA, United States, 5Siemens Healthcare, Austin, TX, United States, 6Institute for Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany
Synopsis
Keywords: Lung, Quantitative Imaging
Pulmonary imaging has taken on greater importance during the COVID-19 pandemic. Regional fractional ventilation (FV) and T1 from MR imaging are potential biomarkers for pulmonary tissue and functional abnormality. However, FV imaging is limited to 2-D acquisition or 3-D with low spatial resolution, and T1 imaging typically requires long breath-holding that is not practical in many scenarios. Furthermore, there is no existing technique for simultaneous acquisition of both pieces of information. To address these limitations, we propose a novel motion-resolved pulmonary imaging technique for simultaneous FV and T1 mapping using MR Multitasking, and demonstrate its feasibility in 7 healthy volunteers.
Purpose
Evaluations of lung tissue and pulmonary function have taken on particular importance during the global COVID-19 pandemic. As a versatile imaging technique, MRI is especially suitable for early screening and long-term follow-up due to its non-ionizing nature. Studies have shown that fractional ventilation (FV) estimated from a series of time-resolved MR images is capable of revealing potential pulmonary disorders1,2. T1 mapping can be used in the detection of fibrosis3 and embolism4. However, pulmonary MRI faces challenges in spatial coverage, SNR, and motion artifacts. Ventilation mapping methods usually use 2D acquisition5 to avoid severe motion artifacts or 3D acquisition6 with limited in-plane resolution. Existing lung T1 mapping techniques are 2D acquisition and typically require breath-holding or respiratory avaraging, which results in compromises in coverage and image quality. Simultaneous acquisition of T1 maps and FV map is not yet available. To address those limitations, we propose a novel MR Multitasking technique7 to enable respiratory motion resolved imaging of the entire lung and investigate the feasibility of simultaneous motion-resolved T1 mapping and FV mapping using a 6-minute scan.Methods
Sequence Design: With Multitasking, two sequential 3D FLASH scans with different flip angles were used to generate T1 contrast. No preparation module was used. A stack-of-spiral sampling pattern with randomized reordering following Gaussian distribution in-plane and in partition encoding was designed for data sampling. Ultra-short TE (TE=0.17ms) was enabled to maximize signal-noise-ratio. One spiral interleave in the partition kz=0 was repeated every 8 readouts7.Imaging Model: In the reconstruction, images $$$I=(\textbf{r},t,\alpha)$$$ were represented as a 3-way tensor $$$\mathscr{A}$$$ with one way representing 3D spatial location $$$\textbf{r}=(x,y,z)$$$, the second indexing temporal dimension $$$t$$$, and the third indexing flip angle $$$\alpha$$$. The tensor can be decomposed in collapsed form as $$\textbf{A}_{(1)}=\Phi \times_1 \textbf{U},\space \tag{1}$$ Where $$$\textbf{U}$$$ contains spatial basis functions and the tensor $$$\Phi$$$ contains temporal basis functions to resolve temporal states (e.g. motion, perfusion, flip angle). $$$\Phi$$$ can be determined from the training data $$$\textbf{d}$$$. The spatial factor $$$\textbf{U}$$$ is reconstructed by: $$\widehat{ \textbf{U} }=\arg \min _{\textbf{U}}||\textbf{d}-\Omega[\Phi \times_1 \textbf{FSU}]||_2^2+\lambda R(\textbf{U}),\space \tag{2}$$ With undersampling operator $$$\Omega$$$, spatial Fourier transform operator $$$\textbf{F}$$$, coil sensitivity $$$\textbf{S}$$$, regularization function $$$R(\cdot)$$$ and regularization parameter $$$\lambda$$$.
T1 Mapping and Fractional Ventilation Analysis
T1 maps were fitted based on the Bloch equations for dual flip angle contrast8 on the end-of-expiration state.
The FV map and flow-volume (FVL) correlation map were estimated from the lower flip angle images using a third-party prototype software (MR Lung v2.1; Siemens Healthcare, Erlangen, Germany)2.
Imaging Experiments: 7 healthy volunteers were scanned on a 3T scanner (MAGNETOM Vida, Siemens Healthcare, Germany). The imaging parameters were: FOV = 500x500x240mm3 in coronal view, resolution = 1.6x1.6x10mm3, TE/TR=0.17/3ms, dual flip angle = 2°/8°. Subjects were free-breathing during the scan. Each coil image was reconstructed separately, then combined by the sum-of-squares (SOS) method9. An end-of-expiration breath-holding dual flip angle sequence with the same imaging parameters (FOV, resolution, ultra-short TE, TR, flip angle) and stack-of-spiral trajectory was used for T1 map reference. A 2-D PREFUL sequence2 was used for ventilation maps reference.
Results
Figure 1 shows the sequence diagram and k-space trajectory. Figure 2 shows representative T1 maps of the breath-holding reference sequence and the proposed method from one representative healthy subject. Figure 3 shows a representative FV map and FVL correlation map by 2-D PREFUL and Multitasking from the same subject. Multitasking demonstrated comparable image quality and value in T1 maps by visual assessment. Ventilation maps of the proposed method show comparable uniformity but blurred lung bronchi. Table 1 shows the statistics of lung parenchyma T1 and ventilation, indicating a significant difference in FV between Multitasking and reference, but no significant difference in FVL correlation and T1 measurements. In 7 healthy volunteers, end-of-expiration lung parenchyma T1 values by Multitasking are 1316.6±207.1ms, which are consistent with the literature4,10,11.Discussion and Conclusion
The preliminary study demonstrated the feasibility of simultaneous acquisition of respiratory motion resolved T1 map and fractional ventilation map using the proposed pulmonary MR Multitasking technique with a single 6-min scan. In 7 healthy volunteers, the proposed method shows comparable T1 map quality with breath-holding reference while the T1 measurements are consistent with literature reports. Further validation of fractional ventilation measurements and testing in patients with various lung disorders is required.Acknowledgements
No acknowledgement found.References
1. Nyilas S, Bauman G, Pusterla O, et al. Ventilation and perfusion assessed by functional MRI in children with CF: reproducibility in comparison to lung function. Journal of cystic fibrosis. 2019;18(4):543-550.2. Voskrebenzev A, Gutberlet M, Klimeš F, et al. Feasibility of quantitative regional ventilation and perfusion mapping with phase‐resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magnetic resonance in medicine. 2018;79(4):2306-2314.
3. Gai ND, Malayeri AA, Bluemke DA. Three‐dimensional T1 and T2* mapping of human lung parenchyma using interleaved saturation recovery with dual echo ultrashort echo time imaging (ITSR‐DUTE). Journal of Magnetic Resonance Imaging. 2017;45(4):1097-1104.
4. Mirsadraee S, Tse M, Kershaw L, et al. T1 characteristics of interstitial pulmonary fibrosis on 3T MRI—a predictor of early interstitial change? Quantitative imaging in medicine and surgery. 2016;6(1):42.
5. Bauman G, Bieri O. Matrix pencil decomposition of time‐resolved proton MRI for robust and improved assessment of pulmonary ventilation and perfusion. Magnetic resonance in medicine. 2017;77(1):336-342.
6. Klimeš F, Voskrebenzev A, Gutberlet M, et al. 3D phase‐resolved functional lung ventilation MR imaging in healthy volunteers and patients with chronic pulmonary disease. Magnetic Resonance in Medicine. 2021;85(2):912-925.
7. Christodoulou AG, Shaw JL, Nguyen C, et al. Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nature biomedical engineering. 2018;2(4):215-226.
8. Deoni SC, Rutt BK, Peters TM. Rapid combined T1 and T2 mapping using gradient recalled acquisition in the steady state. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2003;49(3):515-526.
9. Roemer PB, Edelstein WA, Hayes CE, Souza SP, Mueller OM. The NMR phased array. Magnetic resonance in medicine. 1990;16(2):192-225.
10. Saunders LC, Eaden JA, Bianchi SM, Swift AJ, Wild JM. Free breathing lung T1 mapping using image registration in patients with idiopathic pulmonary fibrosis. Magnetic Resonance in Medicine. 2020;84(6):3088-3102.
11. Stadler A, Jakob PM, Griswold M, Barth M, Bankier AA. T1 mapping of the entire lung parenchyma: influence of the respiratory phase in healthy individuals. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2005;21(6):759-764.
Figures
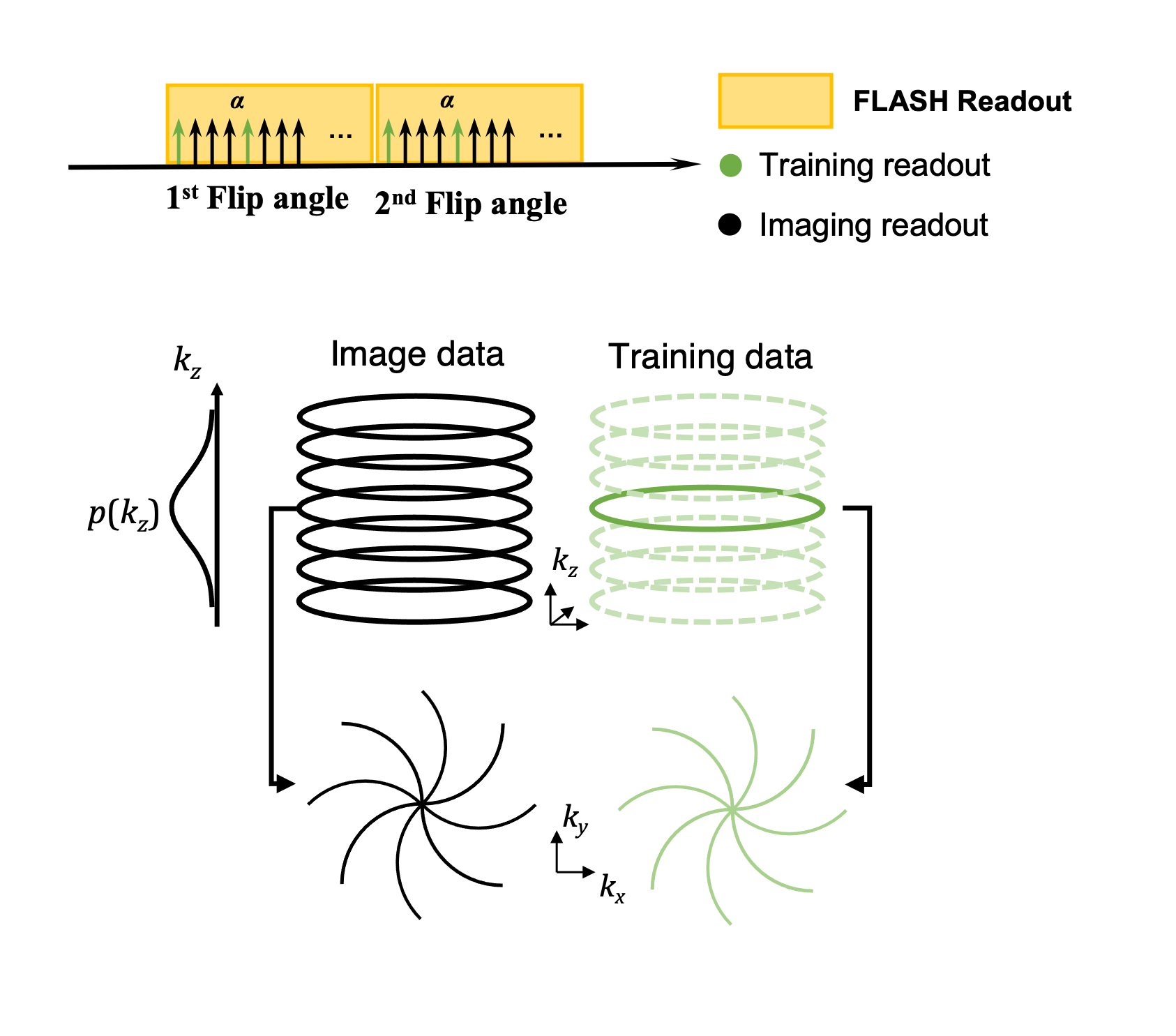
Figure 1. Sequence diagram and k-space trajectory
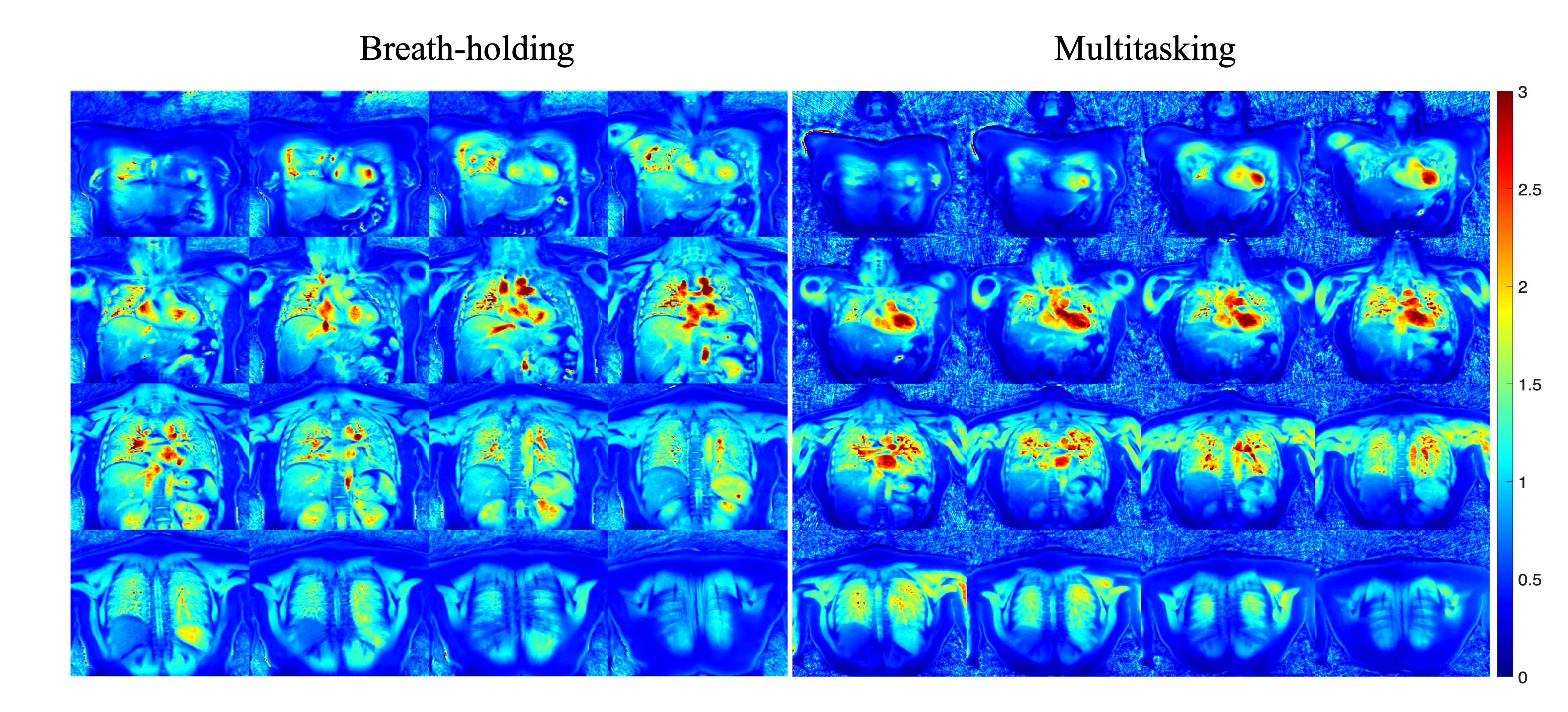
Figure 2. T1 maps of breath-holding reference and free-breathing Multitasking (proposed)
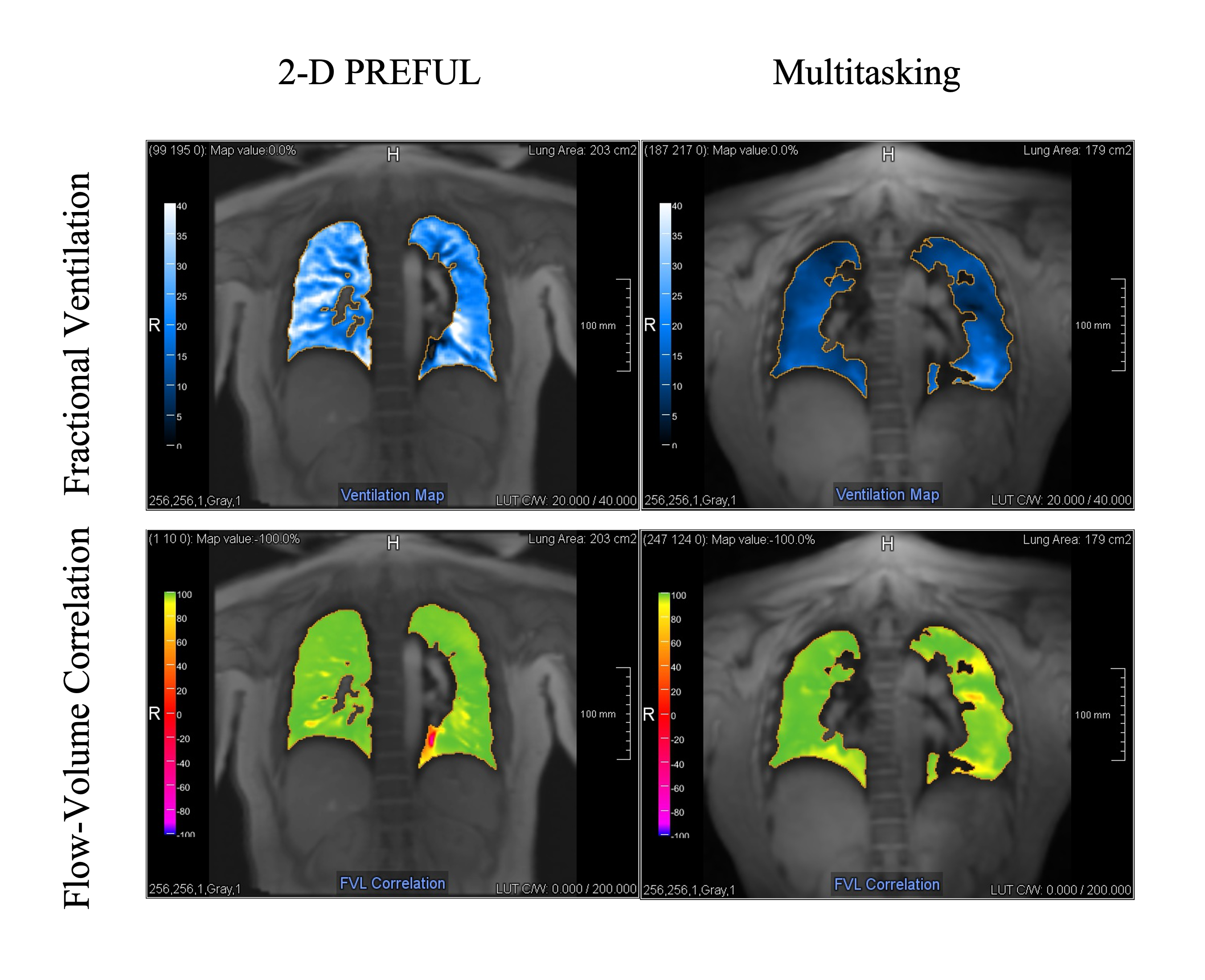
Figure 3. Ventilation maps of 2-D PREFUL reference (left) and Multitasking (right). Top row: fractional ventilation map. Bottom row: fractional ventilation loop correlation

Table 1. Statistics of FV and FVL correlation in 2-D PREFUL and Multitasking
DOI: https://doi.org/10.58530/2023/4658