4587
Improved multi-channel pTx B1+ mapping in the head and neck at 7T by combining RF shims and transmit voltages1Wellcome Centre for Integrative Neuroimaging, FMRIB, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
Synopsis
Keywords: Parallel Transmit & Multiband, High-Field MRI, B1+ mapping
Acquiring robust multi-channel B1+ maps in both the head and neck using pTx head coils at 7T can be challenging due to the combination of low RF penetration into the neck, the limited dynamic range of multi-channel B1+ mapping techniques, and B0 sensitivity. We present a pipeline for large dynamic range pTx field mapping along with a publicly available 10-subject database of head and neck field maps for a commonly used multi-channel head transmit coil. The pipeline is evaluated by comparing the predicted B1+ to the measured B1+ for random transmit shim configurations in the head and neck.Introduction
The use of parallel transmission (pTx) for ultra-high-field MRI1 provides improved control over the transmit B1 (B1+) field by controlling the amplitude and phase of the individual transmit channels. Multi-channel B1+ mapping aims to characterize the transmit fields of all pTx channels. This enables the calculation and optimization of different (including universal2) RF shims and pTx pulses.In applications such as arterial spin labeling3,4 and arterial blood suppression for vessel wall imaging5, multi-channel B1+ information may be required in the neck as well as in the head. Acquiring these data using pTx head coils can be challenging due to the combination of low RF penetration into the neck and the inherently limited dynamic range of B1+ mapping techniques. High transmit voltages can achieve B1+ coverage in the neck, but are inaccurate for high-B1+ regions. Here, an approach to simultaneously achieve accurate multi-channel B1+ measurement in the head and neck is proposed. Using this method, a 10-subject multi-channel head-and-neck B1+ database for a standard 8-channel 7T pTx head coil was acquired.
Methods
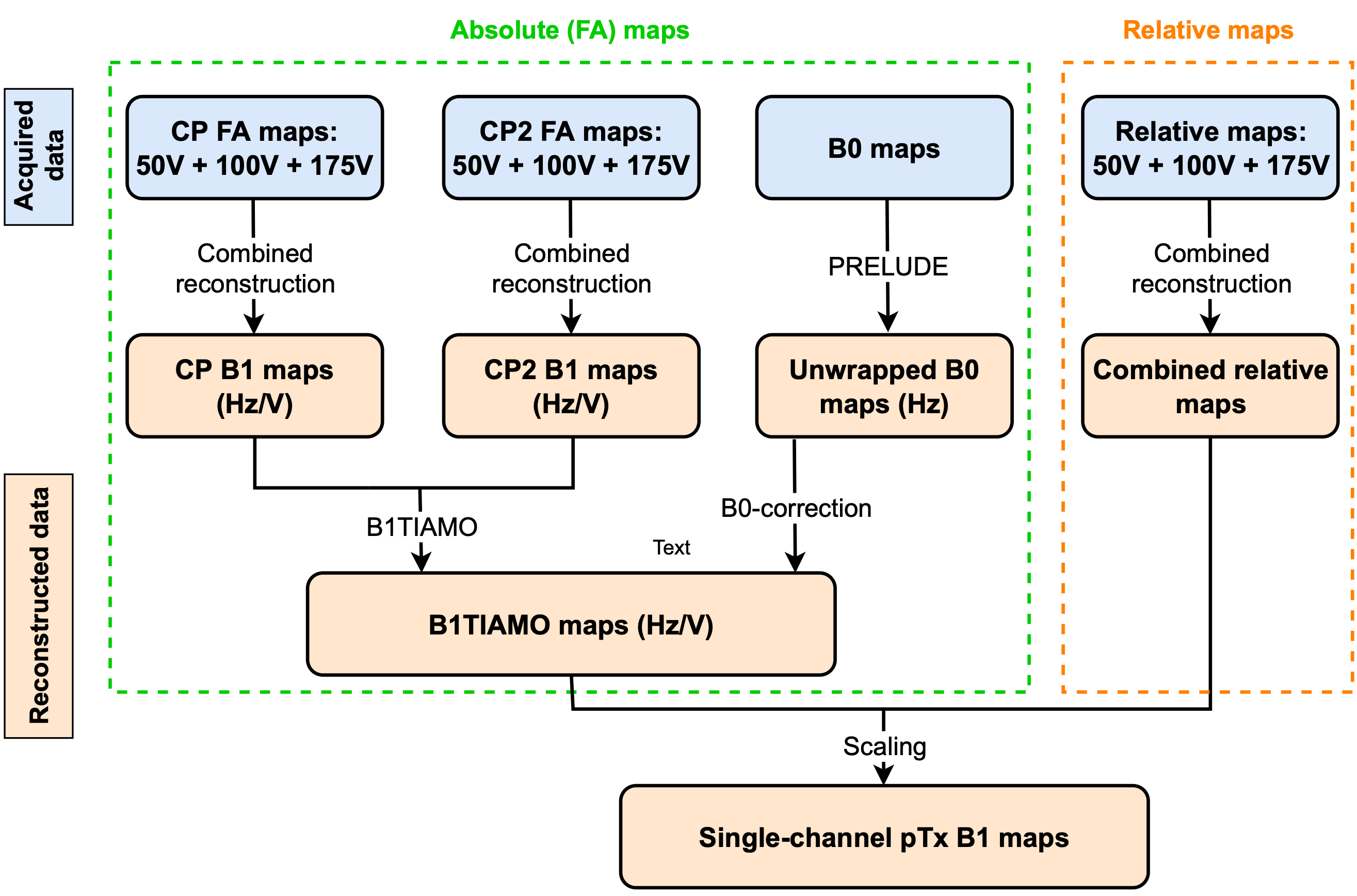
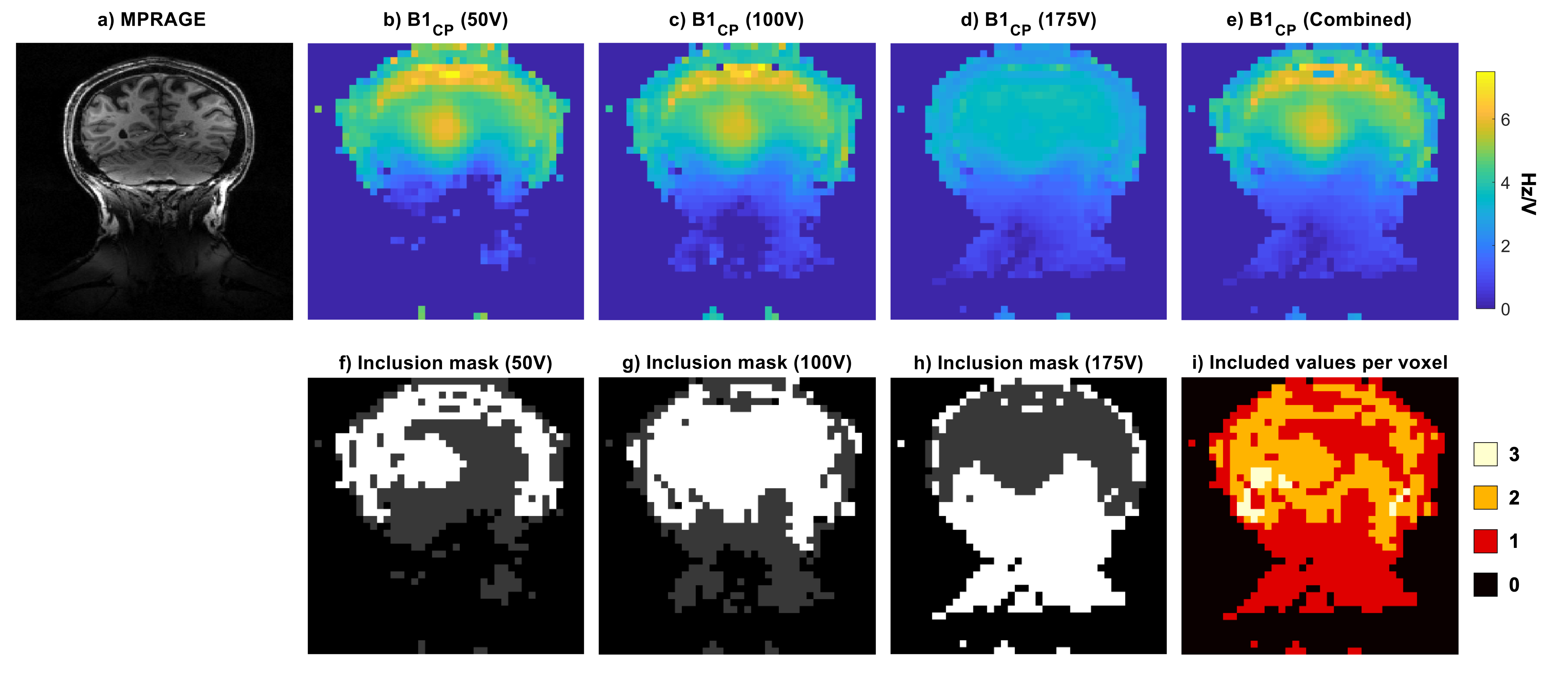
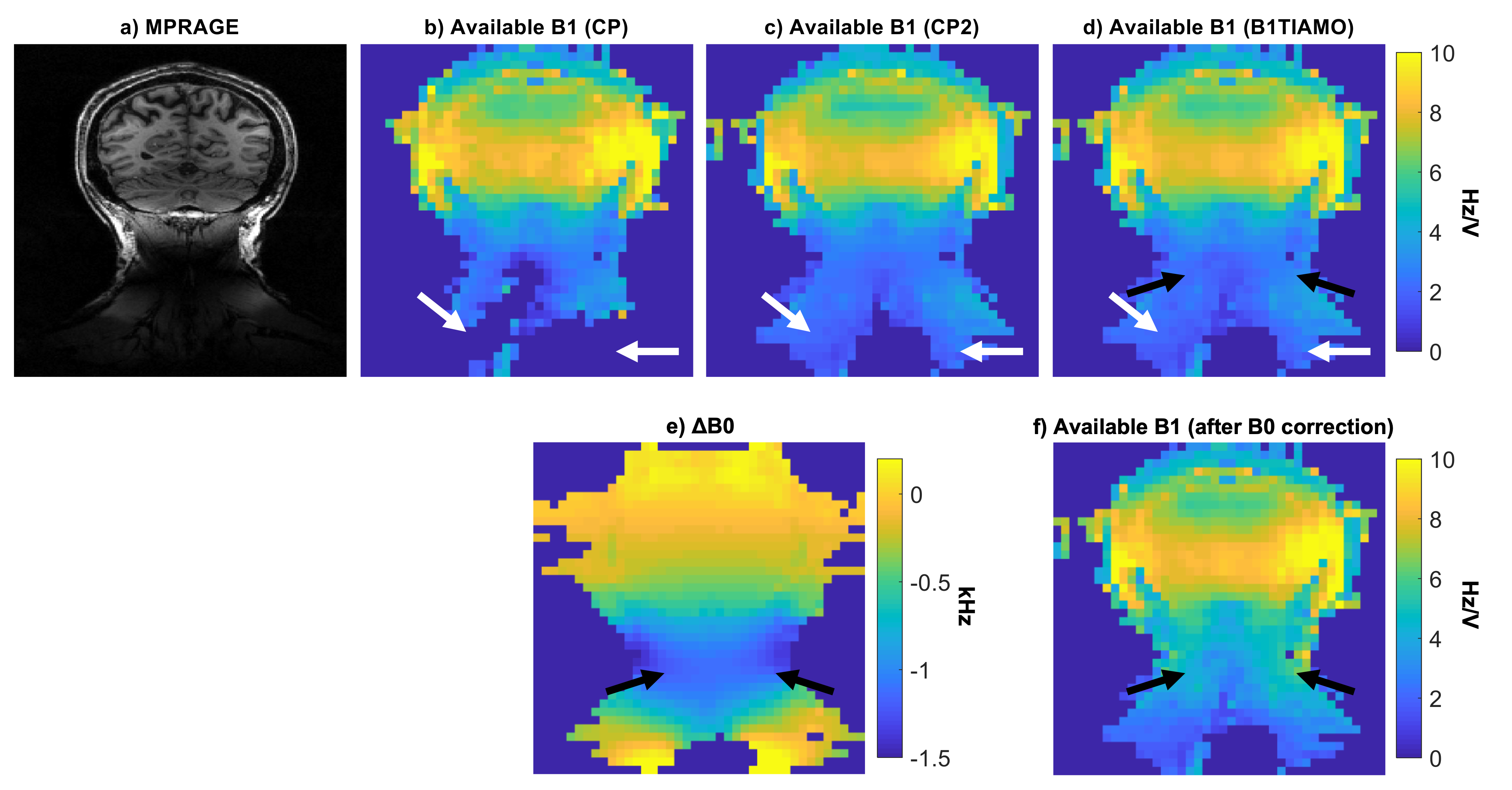
Data were acquired on a Siemens Magnetom 7T scanner using a Nova Medical 8Tx/32Rx head coil under an institutional ethical agreement. All B1+ and B0 field maps were acquired in 3D with the same FOV (225×225×300mm) and a resolution of 7.5×5.6×6.2mm. MPRAGE structural data were acquired at 1.2mm isotropic resolution for anatomical reference.The pipeline, which is shown in Figure 1, comprised of three parts: the first is absolute field mapping, the second relative field mapping, and the third combines them to generate multi-channel B1+ field maps. Six absolute maps were acquired using Sandwiched B1+ mapping6. These included three transmit reference voltages (50V, 100V and 175V), each acquired in two transmit configurations (known as B1TIAMO7): CP-mode (45° phase increments per channel) and CP2-mode (90° phase increments per channel). These six absolute B1+ maps were combined by imposing consistency criteria in the B1+ data expressed in voltage-independent Hz/V units: see Figure 2. Finally, B0 maps were measured and used to correct for off-resonance B1+ underestimation arising from the rectangular RF pulse used for B1+ mapping: see Figures 3e-f. PRELUDE8 was used to unwrap the phase maps used for B0 measurement.
The second step measured relative transmit maps at three reference voltages (50V, 100V, and 175V) using low flip angle gradient echo with a nominal flip angle of 4°. These were measured by transmitting on one channel at a time in an interleaved fashion to minimise magnetisation history effects. The three relative transmit maps were combined using a previously described large dynamic range method9.
The final step combined the absolute maps with the relative maps to form complex multi-channel B1+ field maps (Figure 1).
Using this approach, large dynamic range B1+ field maps were measured in 10 healthy volunteers (23-56 years old; 8M/2F). For four subjects, additional absolute B1+ maps were measured for validation purposes using two arbitrary RF shims (again at reference voltages of 50V, 100V and 175V).
Results
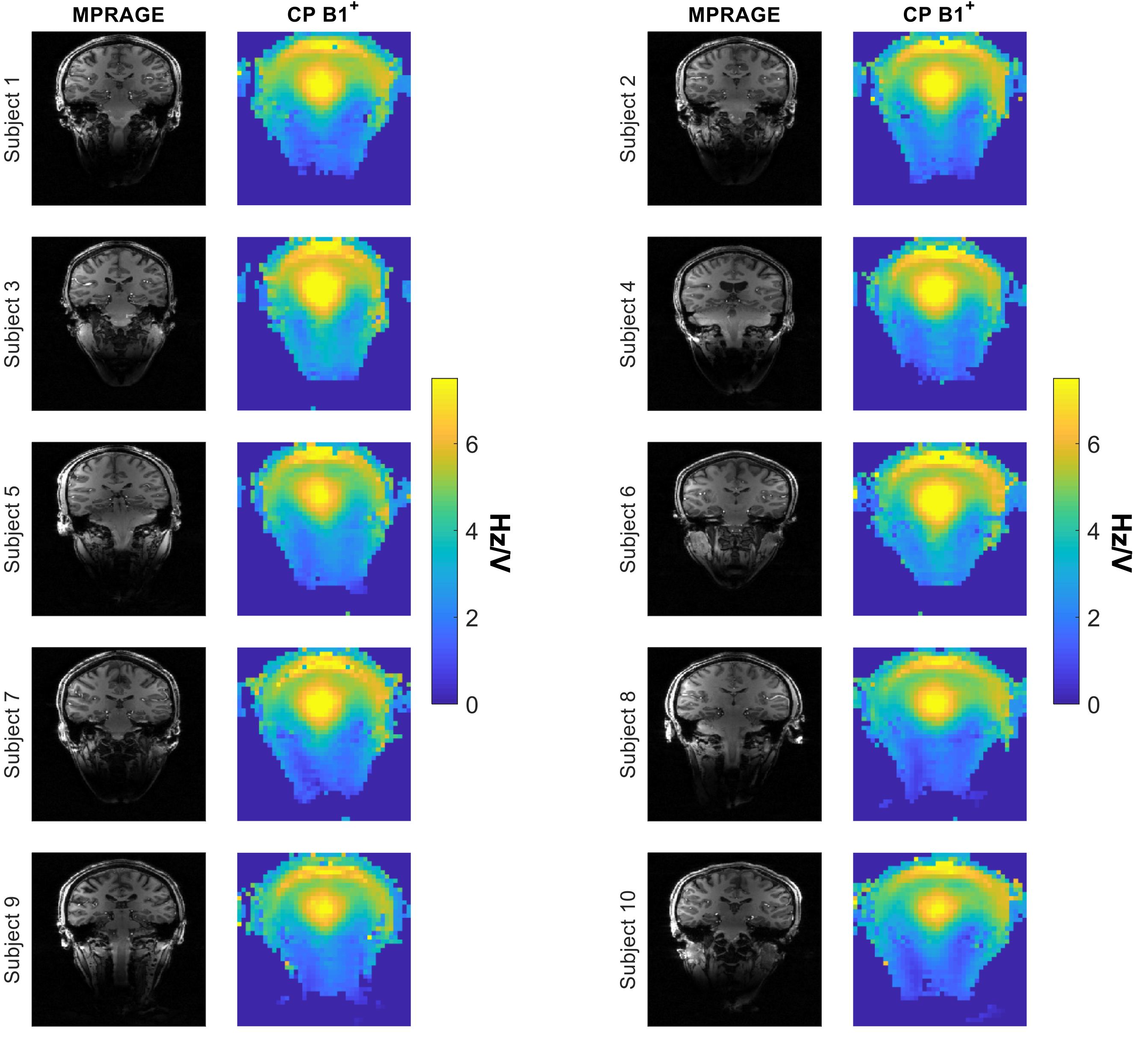
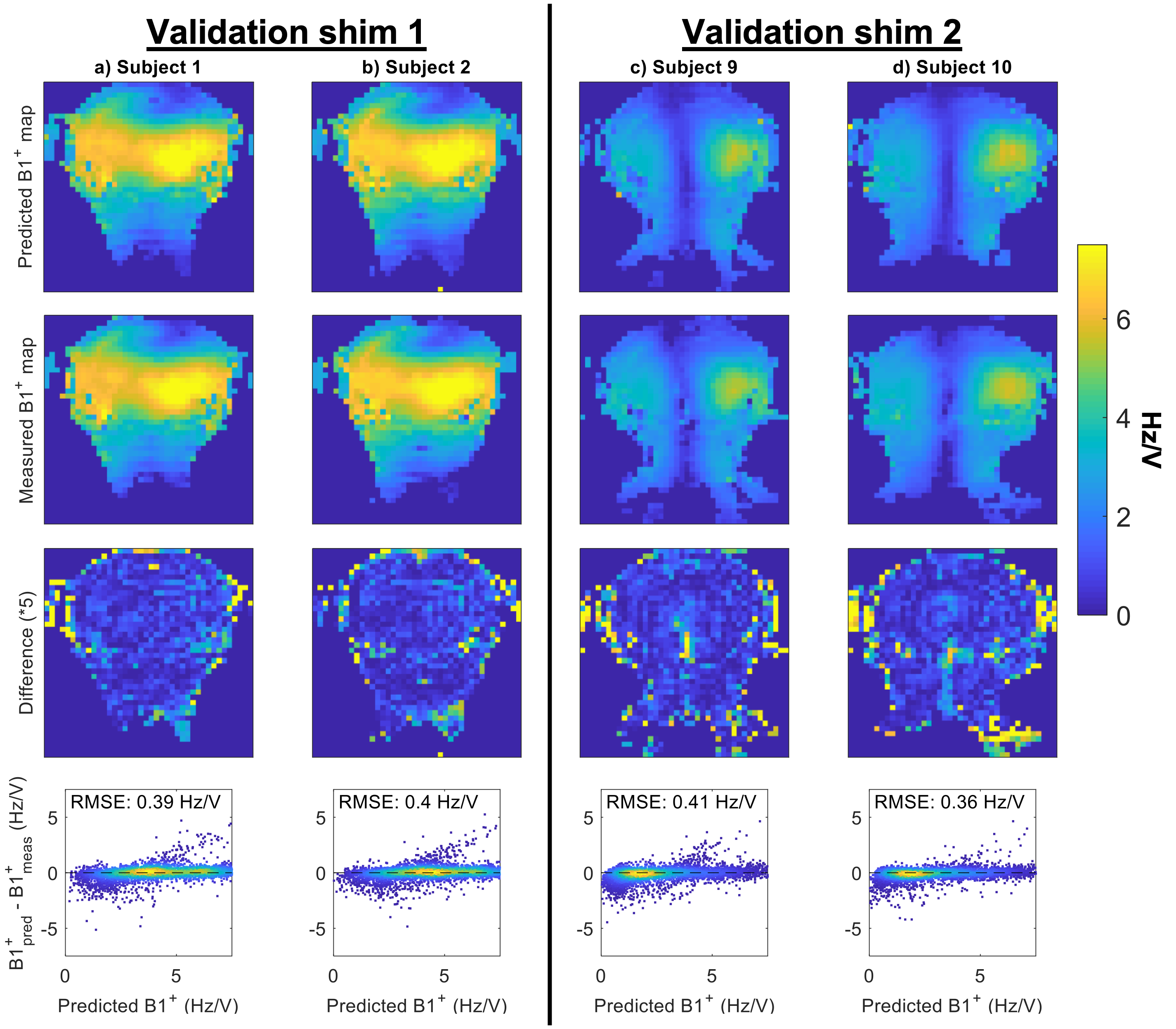
Figure 2 demonstrates how all three voltages are required to cover the full dynamic range of B1+ without departing the linear response of the measurement method, enabling full head-and-neck coverage. Figure 3 demonstrates the utility of B1TIAMO and B0 field correction to increase the spatial coverage. Figure 3e shows up to -1000 Hz off-resonance, requiring B1+ correction by up to a factor of 2.Figure 4 shows the CP-mode B1+ maps for the 10 healthy volunteers. Figure 5 compares the predicted B1+ to the measured B1+ in two random transmit shim configurations. A root-mean-square error (shown in the bottom row) of 0.4 Hz/V was observed for all four subjects.
Discussion
When combining B1+ maps acquired using different RF shims and transmit voltages using the proposed pipeline, a robust B1+ measurement can be obtained in the neck without compromising the B1+ accuracy in the head. Figure 4 shows that this increased coverage is consistently achieved, independent of subject size and position within the coil. The data were acquired using a commonly used pTx coil, so should be useful for other research centres for the calculation of universal pTx shims and pulses or for simulation purposes. Therefore, our data are made openly available online (DOI:10.5287/bodleian:ZB6Gk8QzN).When comparing predicted and acquired B1+ maps for arbitrary RF shims (Figure 5), excellent agreement can be observed throughout the imaging volume. The root-mean-square error values of around 0.4 Hz/V indicate that some differences remain between the predicted and acquired maps. However, some of this remaining disagreement may be caused by inaccuracies in the measured B1+ maps rather than the predicted B1+ maps. For example, in the low-B1+ regions in the middle of the head for Validation Shim 2, discontinuities which do not typically appear in B1+ maps are visible in the measured B1+ maps, while the predicted B1+ maps remain spatially smooth. This is also visible in the scatter plots in Figure 5, where higher measured values are observed for voxels with low predicted B1+ values.
Conclusion
Combining B1+ data from different voltages and RF shims allows the reconstruction of accurate multi-channel head-and-neck B1+ maps for pTx head coils at 7T.Acknowledgements
MdB receives financial support from Siemens Healthineers and the Dunhill Medical Trust. PJ receives support from the Dunhill Medical Trust and the NIHR Oxford Biomedical Research Centre. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).References
1. Padormo F, Beqiri A, Hajnal J v., Malik SJ. Parallel transmission for ultrahigh-field imaging. NMR Biomed. 2016;29(9):1145-1161. doi:10.1002/nbm.3313
2. Gras V, Vignaud A, Amadon A, le Bihan D, Boulant N. Universal pulses: A new concept for calibration-free parallel transmission. Magn Reson Med. 2017;77(2):635-643. doi:10.1002/mrm.26148
3. Tong Y, Jezzard P, Okell TW, Clarke WT. Improving PCASL at ultra-high field using a VERSE-guided parallel transmission strategy. Magn Reson Med. 2020;84(2):777-786. doi:10.1002/mrm.28173
4. Wang K, Ma SJ, Shao X, et al. Optimization of pseudo-continuous arterial spin labeling at 7T with parallel transmission B1 shimming. Magn Reson Med. 2022;87(1):249-262. doi:10.1002/MRM.28988
5. de Buck MHS, Kent JL, Hess AT, Jezzard P. Parallel Transmit DANTE-SPACE for improved black-blood signal suppression at 7 Tesla. In: Proceedings of the 31th Annual Meeting of ISMRM; 2022:2092.
6. Kent JL, Dragonu I, Valkovic L, Hess AT. Rapid 3D Absolute B1+ Mapping using a Sandwiched Train Pre-Saturated TurboFLASH Sequence at 7T for the Brain and Heart. Magn Reson Med. 2022;1-13. doi:10.1002/mrm.29497
7. Brunheim S, Gratz M, Johst S, et al. Fast and accurate multi-channel B1+ mapping based on the TIAMO technique for 7T UHF body MRI. Magn Reson Med. 2018;79(5):2652-2664. doi:10.1002/mrm.26925
8. Jenkinson M. Fast, automated, N-dimensional phase-unwrapping algorithm. Magn Reson Med. 2003;49(1):193-197. doi:10.1002/mrm.10354
9. Padormo F, Hess AT, Aljabar P, et al. Large dynamic range relative B1+ mapping. Magn Reson Med. 2016;76(2):490-499. doi:10.1002/mrm.25884
Figures