4548
Postmortem Imaging with Reusable 3D Printed Ex Vivo Brain Enclosures/Cutting Guide for MRI Registration with Gross Anatomy Photographs at 7T1Bioengineering, University of Pittsburgh, Pittsburgh, PA, United States, 2UPMC, Pittsburgh, PA, United States, 3University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Keywords: New Devices, Ex-Vivo Applications
The ability to continuously prototype and 3D print new containers as well as using an improved transmit coil has led to major improvements in ex-vivo image quality. This has also allowed for a more automated registration process of the MR images to the gross anatomy
Introduction
Since the creation of the 3D printed ex vivo brain enclosure and cutting guide more than 40 brains have been scanned at 7T and registered to the pathology as well as in vivo scans when available. This novel approach to scanning, cutting and registering MRI images to the gross anatomy has proven to be robust and reusable.Previously this study utilized the 16-channel Tic-Tac-Toe (TTT) Coil [1,2] and since has moved to the newly designed 60-channel single-transmit/32 channel receive TTT Coil [3]. There have also been updates to the container to increase the usable volume inside the container while decreasing the volume it takes up inside the rigid receive coil.
Methods
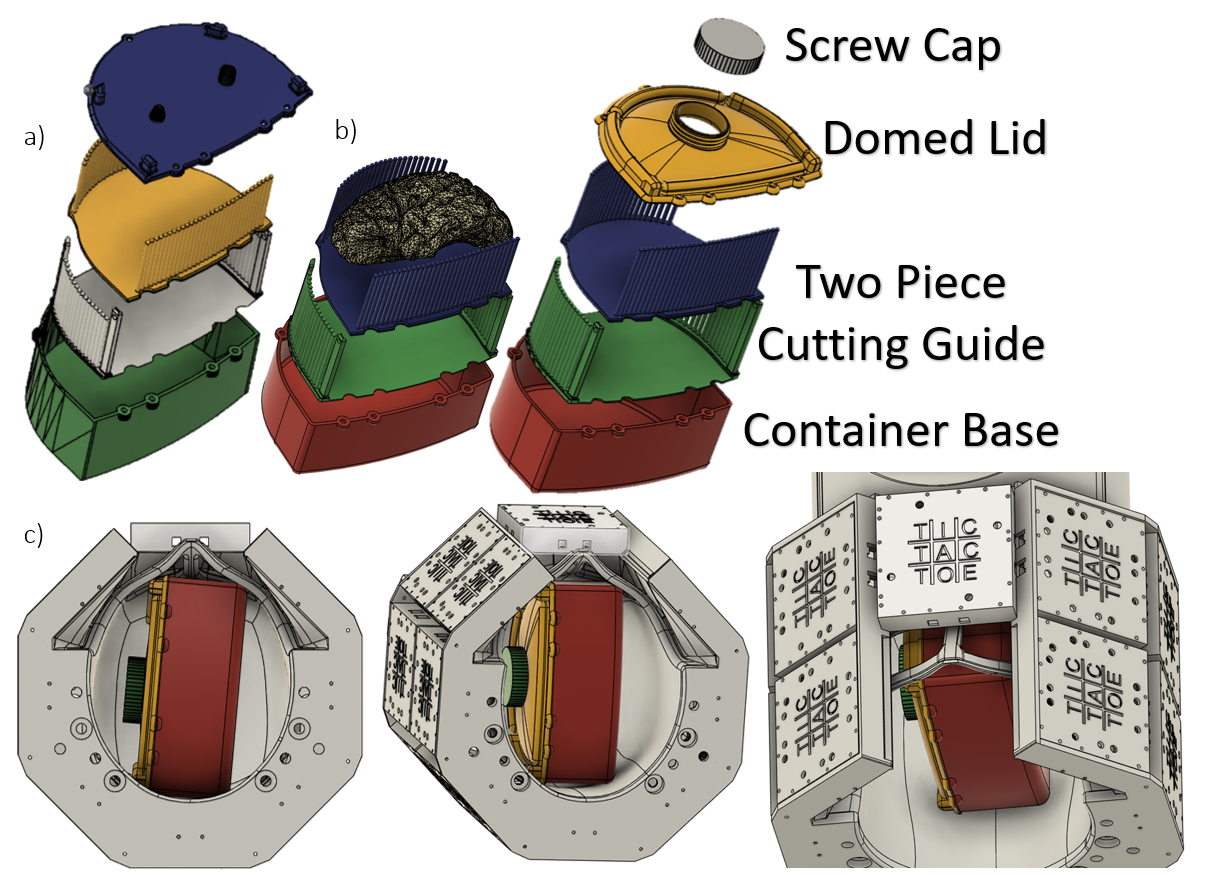
The updated container, visible in Figure 1.b, makes use of a domed lid design which allows for an overall smaller container base while increasing the usable volume the brain occupies in the container. The container has also been rounded to eliminate all sharp corners and fit easier in the oblong head shaped receive coil. The previous fill port and nozzle connector have been replaced with a watertight screw cap. The larger hole allows for hemisphere volume between the top of the container base and the peak of the domed lid to be filled entirely eliminating the possibility for there to be a layer of air between the lid and agar.The left hemisphere of the brain is separated from the right and cerebellum and embalmed in 4% PFA until the day of scanning. An agarose mixture of water, 1.5% agarose and 30% sugar by weight is created and heated to a liquid. The brain is placed in the cutting guide and the cutting guide is placed into the base of the container. Agarose is poured into the container and around the brain carefully ensuring minimal air bubbles are left in the sulci of the brain and ventricles. The lid is then attached, more agarose is added until the container is filled, and the screw cap is secured. The container is wrapped in a plastic bag prior to scanning as an added security measure protecting the coil from the possibility of liquids damaging the coil and providing a barrier between the human tissue/PFA and coil.
The container is then placed into the coil as shown in Figure 1.c, note that it is rotated slightly for improved B1+. The first MR images acquired is a B1+ map using a Turbo-FLASH sequence with TR/TE = 2000/1.16ms; TA = 12min; flip angle from 0° to 90° in 18° increments; and 3.2mm isotropic resolution. Next is an Mp2rage with TA = 32min; TR/TE = 6000/4.1ms; Flip Angle = 6 and 7 degrees; TI1 = 514; TI2 = 2020ms; and 0.4mm isotropic resolution. A GRE is then acquired with TA = 59min TR = 40ms; TE1 = 8ms; TE2 = 15ms; TE3 = 21ms; and .37mm isotropic resolution. A T2-SPACE is acquired with TA = 1hr 38min TR/TE = 3400/363ms; and .36mm isotropic resolution. When transitioning to the 60-channel coil the voltage for the T2-SPACE voltage was scaled proportionally for the higher B1+ field intensity, the new coil provides
Results
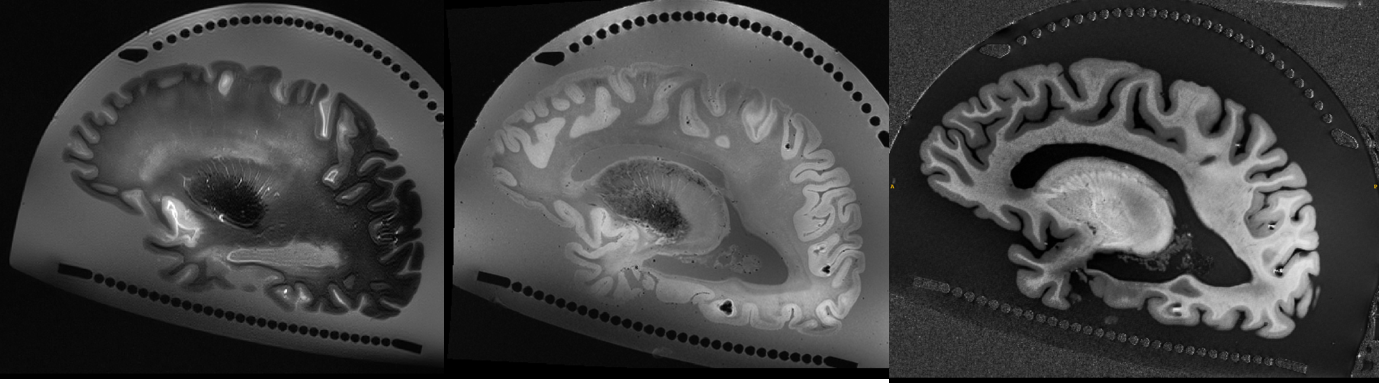
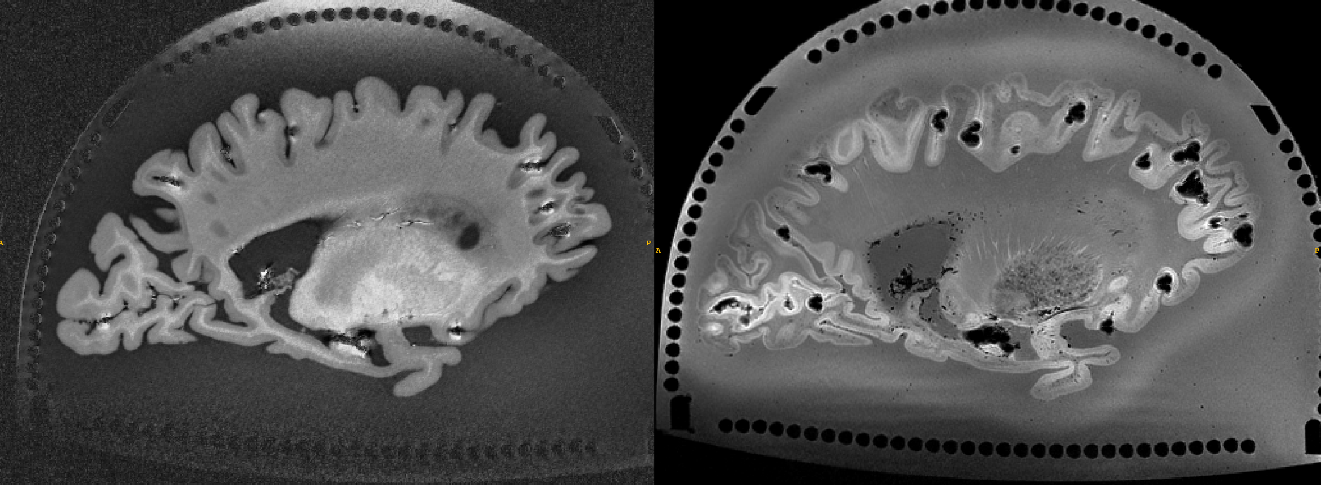
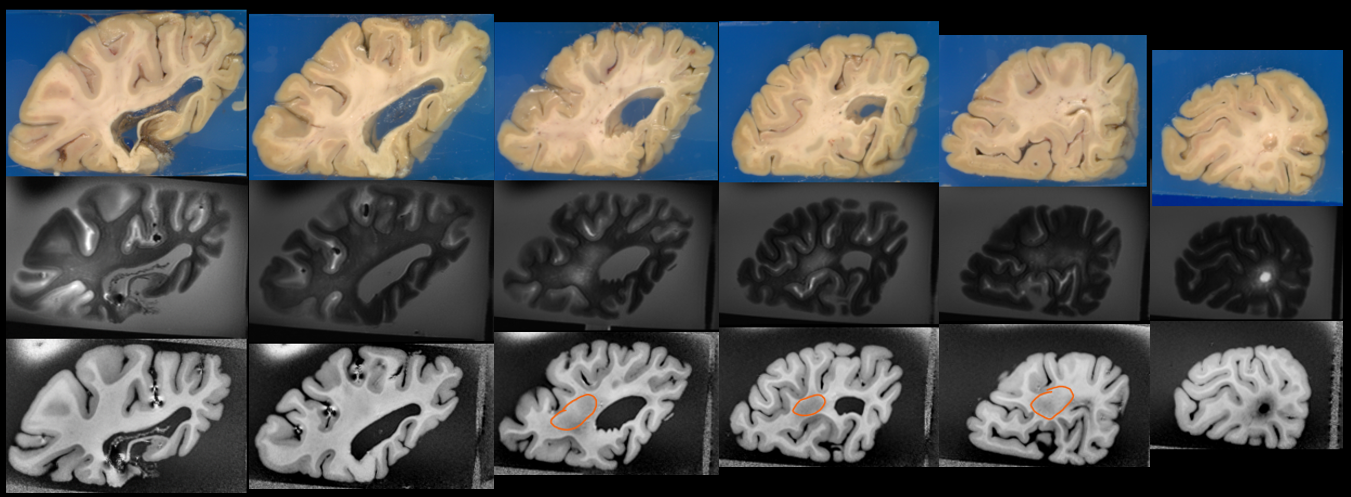
In Figure 2.a b and c are the 60-Channel T2-SPACE, GRE, and MP2RAGE respectfully. The quality of these images can be compared to those in Figure 3.a b and c from the 16-channel coil MP2RAGE and GRE respectively.The image registration process has been automated making use of a photograph provided from the pathologist of cutting locations in order to compute structural similarity index and applying a position gate to guarantee alignment of edge cases. The registered MR images to gross anatomy are visible in Figure 3 and are a near perfect match at all locations. The image quality from the 16-channel to 60-channel TTT coil can be seen in Figure 4. Masks of two separate brains were created and used to analyze the B1+ only where the brain occupies space within the container and are visible in Figure 4.
Discussion
A major benefit our method provides is that the brain is scanned intact with minimal deformations using agarose as a medium to suspend the tissues [4]. This replicated in vivo condition also allows the pathologist to review the images prior to cutting. After deciding where to cut, the design of the cutting guide also provides the pathologist with the freedom to cut at any location with a variety of angles through any singular location.The slightly smaller container size allows for more flexibility when positioning the container in the rigid receive coil. This is important because the 60-channel TTT coil is tuned for a human head.
Conclusion
The improved container shape and lid has resulted in significant improvements, specifically minimizing the manual labor by the pathologist as well as image quality improvement by reducing air bubbles during embedding. The use of the 60-channel single-transmit TTT Coil has also improved the image quality.Future work may include slightly altering the container shape further to make it smaller still and refining the agarose doping concentrations to mimic the dielectric properties of the human head to achieve better homogeneity as seen in vivo [3].
Acknowledgements
This work was supported by the National Institutes of Health under award numbers R01MH111265, R01AG063525, T32MH119168, and U19AG068054.References
References
1. Santini, T., et al. (2020). “Improved 7 Tesla Transmit Field Homogeneity with Reduced Electromagnetic Power Deposition Using Coupled Tic Tac Toe Antennas.” Sci Rep 11: 3370
2. Berardinelli, J., et al. (2022). “Reusable 3D Printed Ex-vivo Brain Enclosure and Two-Piece Cutting Guide for Axial and Coronal MRI Registration with Gross Anatomy Photographs” In Proc. of the 31st International Society of Magnetic Resonance in Medicine Annual Meeting, London, England, United Kingdom
3. Santini, T., et al. (2019). “Homogeneous 64-channel RF transmit array for brain imaging at 7T, 9.4T, and 10.5T.” In Proc. of the 27th International Society of Magnetic Resonance in Medicine Annual Meeting, Montreal, Quebec, Canada.
4. David Lahna, BA, Natalie Roese, MPH, Randy Woltjer, MD, PhD, Erin L Boespflug, PhD, Daniel Schwartz, BA, John Grinstead, PhD, Hiroko H Dodge, PhD, Rachel Wall, MS, Jeffrey A Kaye, MD, William D Rooney, PhD, Lisa C Silbert, MD, Postmortem 7T MRI for guided histopathology and evaluation of cerebrovascular disease, Journal of Neuropathology & Experimental Neurology, 2022;, nlac103,
Figures