4538
Evaluation of Potential Benefits of 7T for Knee Epiphyseal Bone Marrow ASL Imaging
Xiufeng Li1, Jutta Ellermann1, and Gregory J. Metzger1
1University of Minnesota, Minneapolis, MN, United States
1University of Minnesota, Minneapolis, MN, United States
Synopsis
Keywords: Bone, Perfusion, ASL, Knee, 7T, Ultrhigh Field
Knee epiphyseal bone marrow ASL imaging (called knee ASL imaging in the following) is challenging due to very low perfusion in epiphyseal yellow bone marrow mainly consisting of fat cells with a sparse network of capillaries. In general, it is known that higher magnetic fields (i.e. ≥7T) can specifically benefit ASL imaging. However, the specific potential benefits in the knee have not been systematically evaluated to date. We have performed theoretical simulations to explore the potential gain for knee ASL imaging at 7T compared to 3T and present our preliminary experimental results comparing both field strengths.Purpose
Bone marrow perfusion can provide essential knowledge about bone physiology and to improve our understanding of disease etiology and pathophysiology, assist the differentiation between normal and abnormal bone marrow, and assess the response to prescribed therapies. Arterial spin labeling (ASL) magnetic resonance imaging (MRI) (1), as a noninvasive and non-contrast-enhanced approach, is well suited for longitudinal monitoring of disease progression and routine evaluation of therapy response. Recent studies have showed that ASL imaging can measure knee epiphyseal bone marrow blood flow (BMBF) and reflect disease-related changes in juvenile osteochondritis dissecans patients (2-4). These studies also revealed existing challenges including an intrinsically low signal-to-noise ratio (SNR) due to low perfusion and methodological limitations such as single slice coverage and long acquisition times, hampering routine knee ASL applications.Ultrahigh (≥7T) magnetic field (UHF) can specifically benefit ASL imaging and overcome these challenges by increasing SNR, prolonging blood and tissue T1, and improving parallel imaging performance. Today, 7T MRI scanners are becoming more widely available following the FDA’s approval for clinical in the brain and knee. Knee epiphyseal bone marrow ASL imaging (called knee ASL imaging in the following) has been recently performed at 7T with encouraging results (5). However, the specific benefits of 7T for knee ASL imaging have not been systematically evaluated to date. We will report our theoretical simulations to explore the potential gains of 7T compared to 3T for knee ASL imaging and present preliminary experimental results comparing both field strengths.
Methods
Compared to other ASL methods, the flow-sensitive alternating inversion recovery (FAIR) approach does not require the labeling plane or slab perpendicular to feeding arteries, making it robust and suitable for imaging organs or body regions with complicated arterial vascular architectures. The FAIR technique has been applied for knee ASL studies to measure bone marrow blood flow (BMBF) using the single-subtraction/single-delay approach with a sequence-defined temporal bolus width (2-5). In addition, to overcome or minimize the adverse effects of B0 off-resonance and the susceptibility in the knee, spin-echo imaging methods have been used, such as the single-shot fast-spin-echo (ss-FSE) image readout (2-5). The sequence and parameters of these previously presented FAIR ss-FSE imaging methods are also used in the comparison presented here and are illustrated in Figure 1.Our theoretical simulations of the knee ASL imaging at 3T and 7T utilized the same approach as before (6). All the simulations and the analyses of knee ASL imaging data acquired from 3T and 7T (please refer to the previous reports (3,5) for study details) were primarily performed using MATLAB scripts. The blood flow quantification model, formula for perfusion SNR efficiency, and parameters for theoretical simulations are presented in Tables 1 and 2, respectively. With an assumed constant coil g factor across field strengths, image SNR under parallel imaging conditions were normalized to that without parallel imaging. The theoretical potential gains of 7T compared to 3T have been evaluated for different situations where the TRs of 7T were different times of that at 3T.
Results and Discussions
Our simulation results (Figure 2A) suggest that, to achieve optimal ASL SNR efficiency and take advantage of the prolonged blood T1 and higher SNR at 7T, a longer temporal bolus (TI1) should be used by producing a larger effective labeling slab (blue slab in Figure 1) with a larger labeling inversion slab (red slab in Figure 1). For example, when a 1.5 s TI1 is used for 7T imaging, ~2.2 and ~1.7 times higher perfusion SNR efficiencies can be achieved with 0.6 s and 1.2 s PBDs, respectively, even with a TR doubled compared to 3T (Figures 2B and 2C). Of course, a larger labeling slab requires a larger B1+ coverage for the knee coil, and unfortunately, only typical ASL parameters for 3T (e.g., TI/TI1 = 1.2/0.6 s and effective labeling slab size = 60 mm) were used in the previous 7T study (5) to accommodate a short temporal bolus due to limited achievable effective labeling slab size. In addition, as observed in the previous 7T study, B1+ inhomogeneity can further result in lower SNR and SNR efficiency, which is consistent to our preliminary results from the comparison of knee ASL imaging between 3T and 7T (Figure 3). Furthermore, the dramatically increased SNR efficiency at 7T (Figures 2B and 2C) makes it feasible to apply a longer PBD to minimize the adverse intravascular artifacts for reduced bias and accurate flow quantification, which is impossible at 3T due to the intrinsically lower perfusion SNR (2).As is well-known, parallel imaging will have better performance with g factors smaller at 7T for a similar RF coil configuration, which means that the real SNR gain at 7T with parallel imaging most likely would be higher than those used for the presented simulations.
Conclusions
Our study results suggest that to fully take advantage of the benefits of 7T on knee ASL imaging, in addition to overcoming the existing technical changelings due to B1+ and B0 inhomogeneity, a large B1+ coverage is critically important to produce a sufficiently long temporal bolus width to achieved 1.7 to 2.2 times higher SNR efficiency compared to 3T.Acknowledgements
This study was supported by National Institute of Health R56EB033365 and P41 EB027061.References
- Detre JA, Leigh JS, Williams DS, Koretsky AP (1992) Perfusion imaging. Magn Reson Med 23:37-45.
- Li X, Johnson CP, Ellermann J. Measuring Knee Bone Marrow Perfusion Using Arterial Spin Labeling at 3 T. Sci Rep. Mar 24, 2020; 10(1):5260. doi:10.1038/s41598-020-62110-y.
- Li X, Johnson CP, and Ellermann J. Epiphyseal Bone Marrow Perfusion Imaging in the Distal Femur Using Arterial Spin Labeling: Feasibility and Challenges. In: Proceedings of the 25th Annual Meeting of ISMRM, ISMRM 2017: Abstract 0852.
- Li X, Johnson CP, and Ellermann J. Knee Epiphyseal Bone Marrow Perfusion Imaging Using FAIR RESOLVE. In: Proceedings of the 28th Annual Meeting of ISMRM, ISMRM 2020: Abstract 1142.
- Li X, Johnson CP, Ellermann J. 7T bone perfusion imaging of the knee using arterial spin labeling MRI. Magnetic resonance in medicine: official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine. May 2020;83(5):1577-1586. doi:10.1002/mrm.28142.
- Li X, Ugurbil K, and Metzger GJ. Theoretical Evalaution of Ultrahigh Field Benefits to Non-Contrast Enhanced Renal Perfusion Imaging Using FAIR-EPI. In: Proceedings of the 20th Annual Meeting of ISMRM, ISMRM 2013: Abstract 1540.
- Hales PW, Kirkham FJ, Clark CA. A general model to calculate the spin-lattice (T1) relaxation time of blood, accounting for haematocrit, oxygen saturation and magnetic field strength. Journal of cerebral blood flow and metabolism: official journal of the International Society of Cerebral Blood Flow and Metabolism. Feb 2016;36(2):370-4. doi:10.1177/0271678X15605856.
- Krishnamurthy LC, Liu P, Xu F, Uh J, Dimitrov I, Lu H. Dependence of blood T (2) on oxygenation at 7 T: in vitro calibration and in vivo application. Magnetic resonance in medicine: official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine. Jun 2014;71(6):2035-42. doi:10.1002/mrm.24868.
- Zhao JM, Clingman CS, Narvainen MJ, Kauppinen RA, van Zijl PC. Oxygenation and hematocrit dependence of transverse relaxation rates of blood at 3T. Magnetic resonance in medicine: official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine. Sep 2007;58(3):592-7. doi:10.1002/mrm.21342.
Figures
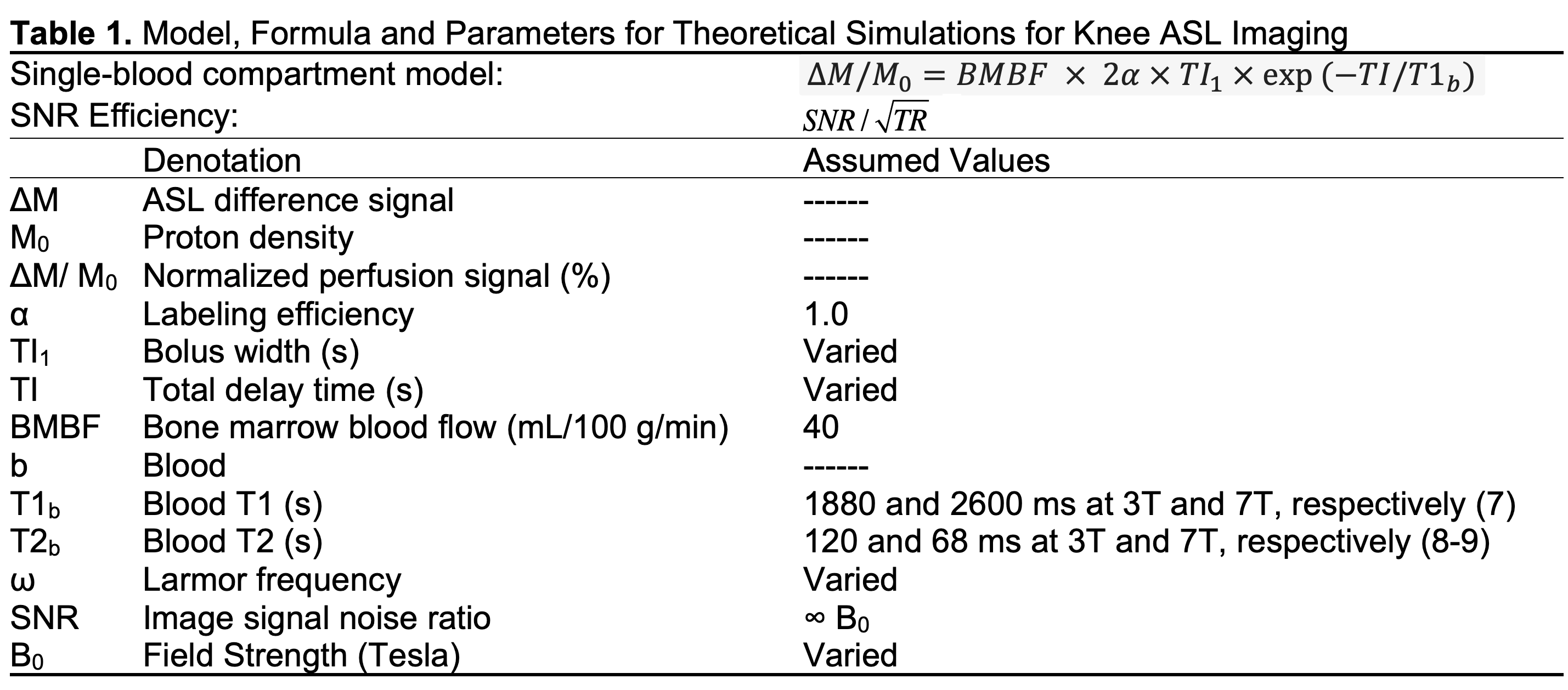
Table 1.
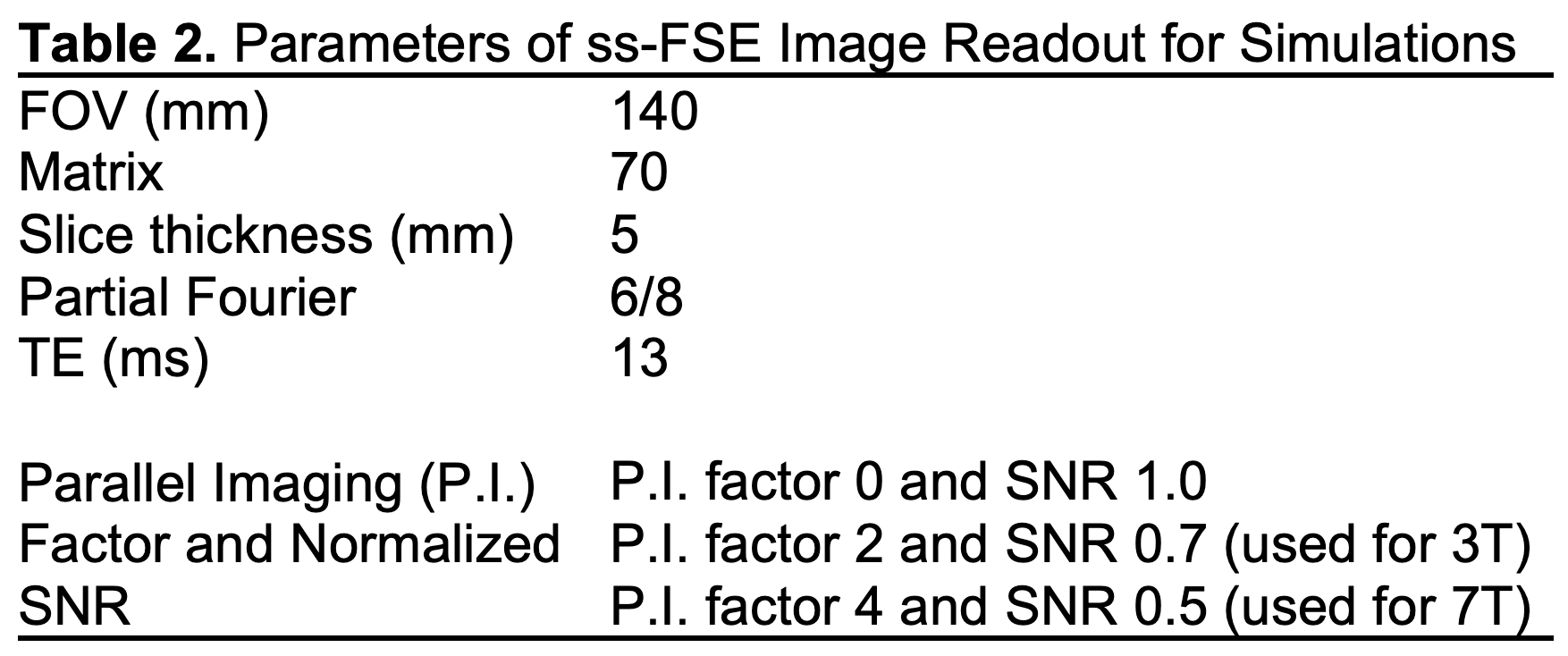
Table 2.
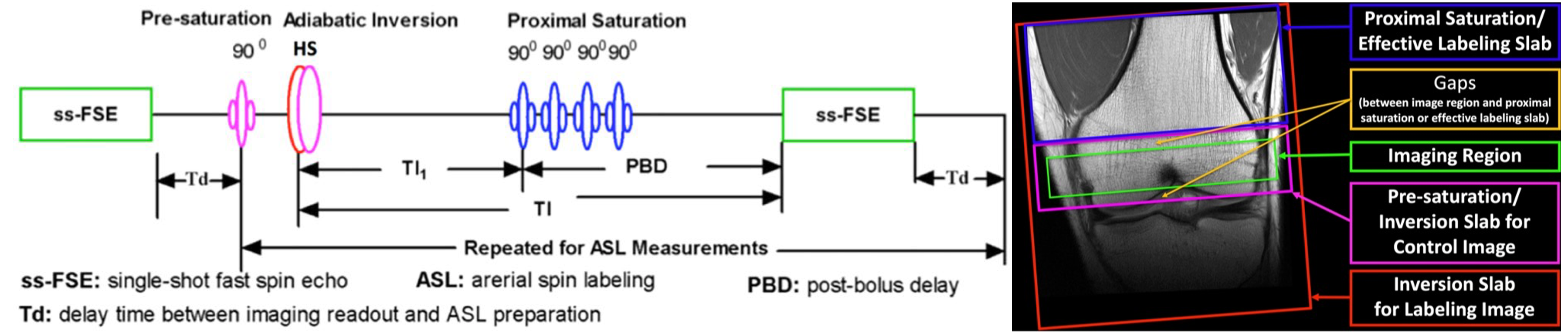
Figure 1. Sequence diagram (left) and RF pulse spatial positions (right)
of FAIR ss-FSE. A single ss-FSE image is first acquired to measure fully
relaxed bone marrow magnetization (called M0 image) before repeated
labeling or control image acquisitions with a defined temporal bolus width
(TI1) followed by a post-bolus delay (PBD=TI-TI1).
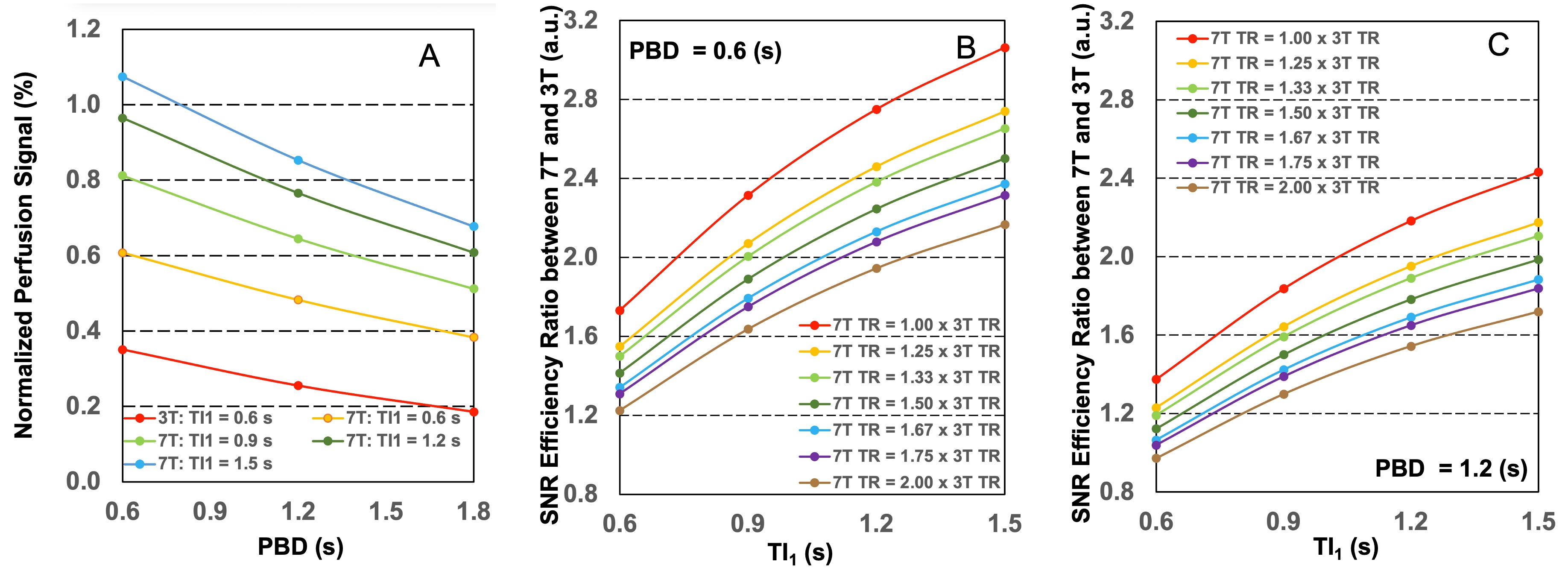
Figure 2. Simulation results
of knee FAIR ss-FSE imaging with a single-blood compartment model for BMBF
quantification using assumed 40 mL/100 g/min perfusion: normalized perfusion
signal (left), SNR efficiency ratios between 7T and 3T (middle and right) from
imaging using different TI1s and PBDs. With a typical 3 s TR at 3T,
the 1.33 and 1.67 times of 3T TR correspond to 4 s and 5 s TR for 7T,
respectively.
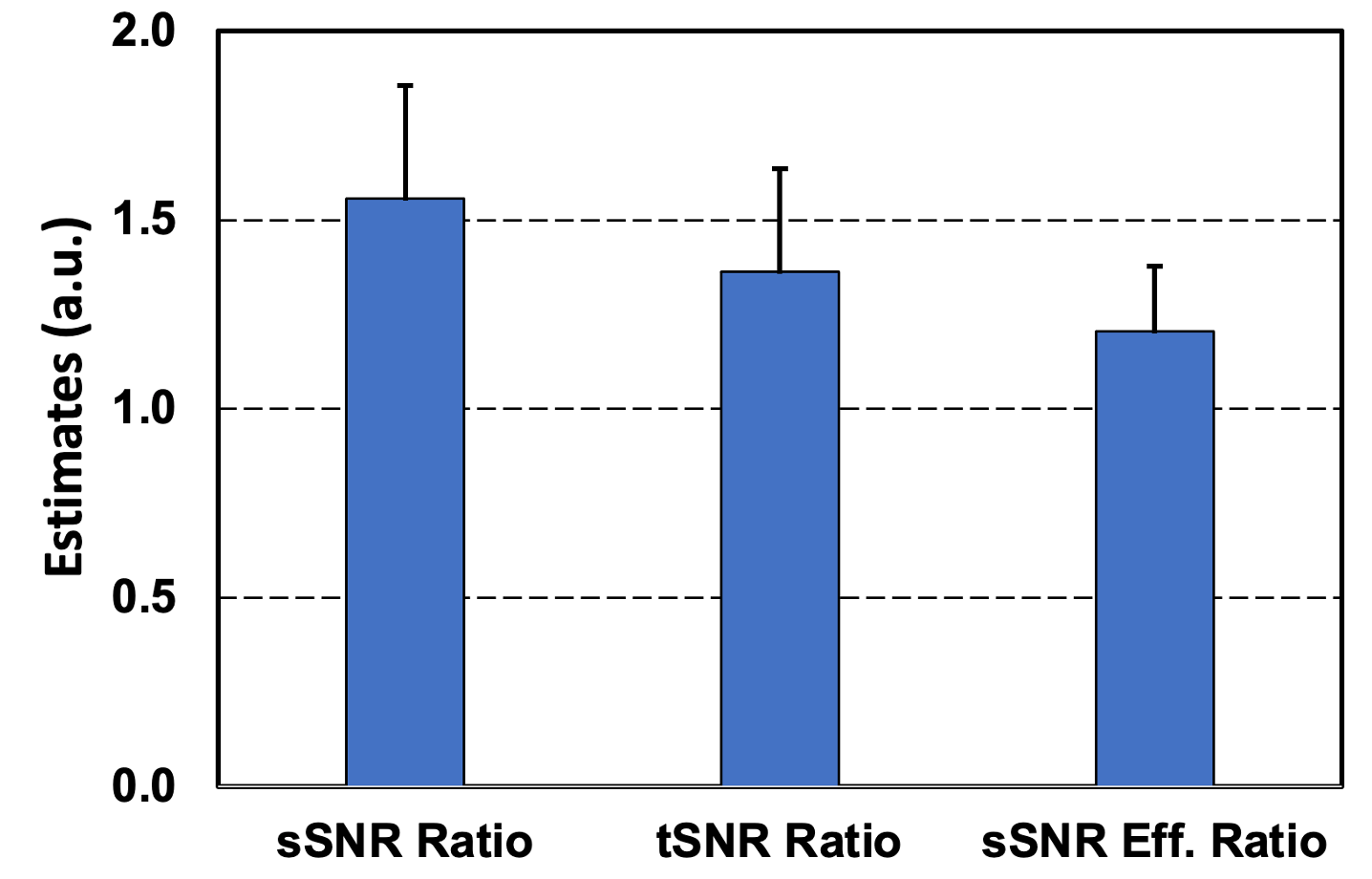
Figure 3. Spatial and temporal SNR (sSNR and tSNR)
ratios and sSNR efficiency ratio between 3T and 7T. Error bars represent
standard deviations.
DOI: https://doi.org/10.58530/2023/4538