4497
The effect of variable compressed sense (CS) undersampling patterns in hyperpolarized Xenon (129Xe) diffusion-weighted MRI1Electrical and Computer Engineering, McMaster University, Hamilton, ON, Canada, 2Imaging Research Centre, St. Joseph's Healthcare, Hamilton, ON, Canada, 3Department of Medicine, McMaster University, Hamilton, ON, Canada, 4Firestone Institute for Respiratory Health, St Joseph’s Healthcare Hamilton, Hamilton, ON, Canada, 5Imaging Research Centre, St. Joseph’s Healthcare Hamilton, Hamilton, ON, Canada, 6Biomedical Engineering, McMaster University, Hamilton, ON, Canada, 7Department of Radiology, McMaster University, Hamilton, ON, Canada
Synopsis
Keywords: Image Reconstruction, Sparse & Low-Rank Models, Compressed Sensing, Lung, 129Xenon
Compressed sensing is a fast-imaging technique capable of making high quality images with undersampled data. However, its application in hyperpolarized 129Xe diffusion-weighted MRI needs to be optimized. In this study, diffusion weighted images undersampled identically and differently, were compared with SNR, SSIM, mean ADC using repeated measures ANOVA. The application of different undersampling patterns for both diffusion-weighted and baseline images can result in ADC maps with higher quality, as compared to fully sampled equivalent parametric images. Thus, the baseline and diffusion-weighted images do not necessarily have the same optimum undersampling pattern, and optimization of each needs investigation separately.
Introduction
The size of lung airspaces can be indirectly probed by measuring the MRI apparent diffusion coefficient (ADC) of inhaled hyperpolarized 129Xe gas. ADC maps are calculated from one baseline image without diffusion weighting (i.e., b=0 cm2/s) and at least one other with diffusion weighting (i.e., b>0 cm2/s). This is used to measure airspace enlargement in lung diseases such as chronic obstructive pulmonary disorder (COPD)1. However, one challenge is the long scan time and associated breath hold, which can be problematic for patients with lung disease. Fast imaging, employing techniques such as Compressed Sensing (CS), permits faster data acquisition without sacrificing spatial resolution2 and has recently been deployed for diffusion-weighted 129Xe MRI3. Previous studies on 129Xe ventilation imaging showed substantial SNR and spatial frequency variation among CS reconstructed MR images4. In this study, we explored the effect of sampling patterns on resultant ADC maps and the effect of using identical or non-identical sampling patterns for the baseline and diffusion-weighted images.Methods
Four subjects (2 healthy never-smokers, 2 COPD) were scanned using a GE MR750 3T MRI, acquiring fully sampled 3D multi-slice HP 129Xe diffusion-weighted MR images (128x80x8, one b=0 cm2/s, one b=20 cm2/s, polarization 9-11%, age range: 25-68)5. 200 variable-density Cartesian random undersampling masks were generated each at 7 different sampling rates, (15% to 75%, step length = 10%), where undersampling was performed only in the phase encoding direction leaving central parts of k-space fully sampled6. Two different groups of ADC maps were derived: one where each pair of b-value images was undersampled identically, and a second where different undersampling masks were applied to each pair of b-value images. The Parallel Imaging Compressed Sensing (PICS) command from the Berkeley Advanced Reconstruction Toolbox (BART)7 with l1 wavelet optimization and 100 iterations, was used to reconstruct undersampled data. The results (2x7x200=2800 ADC maps per subject) were evaluated using Signal to Noise Ratio (SNR), Structural Similarity (SSIM) and mean parenchymal ADC. Statistical analysis was done using repeated measures Analysis of Variance (rmANOVA) using Matlab 2022a (The Mathworks, Natick MA). The study was approved by our local research ethics board.Results
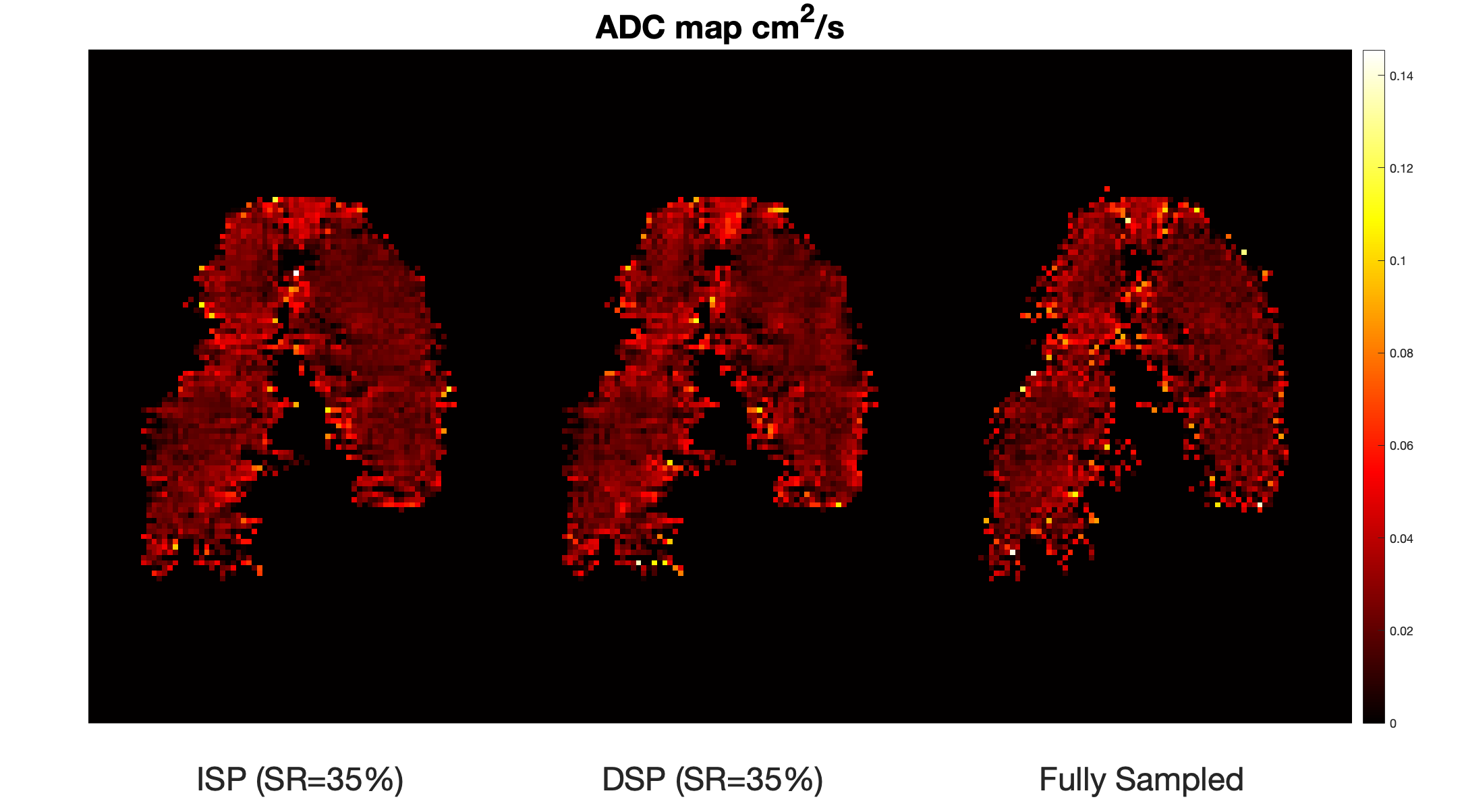
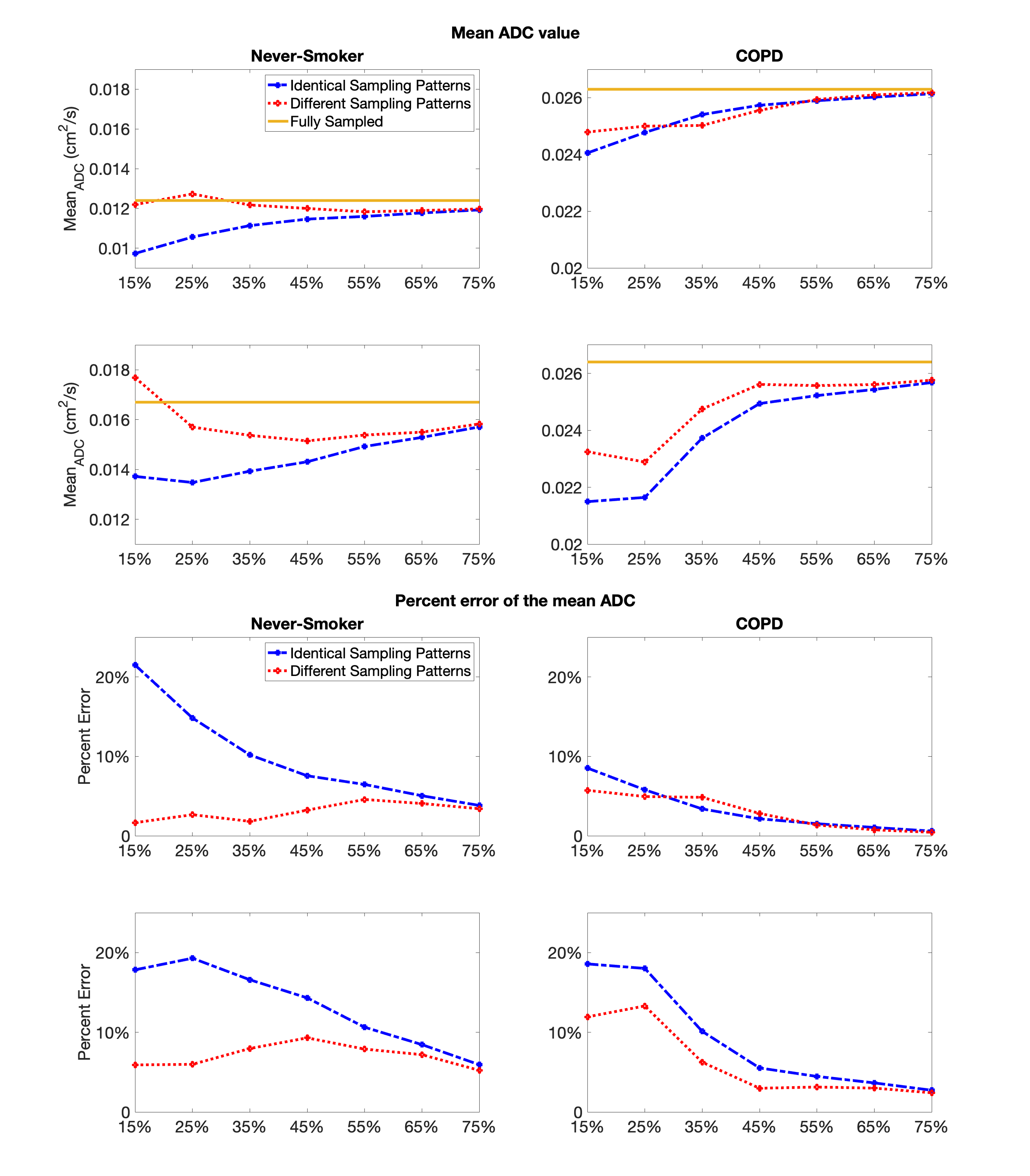
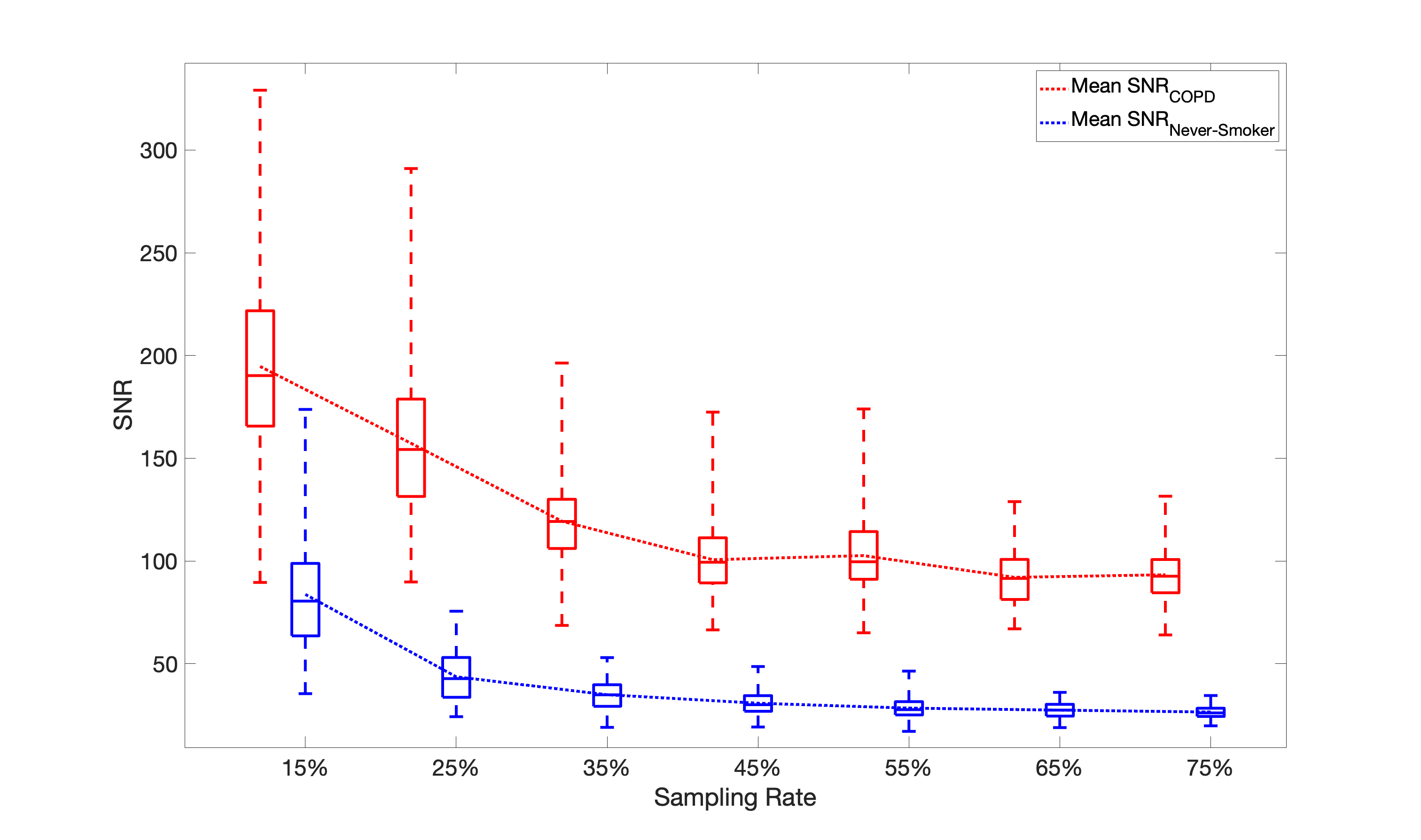
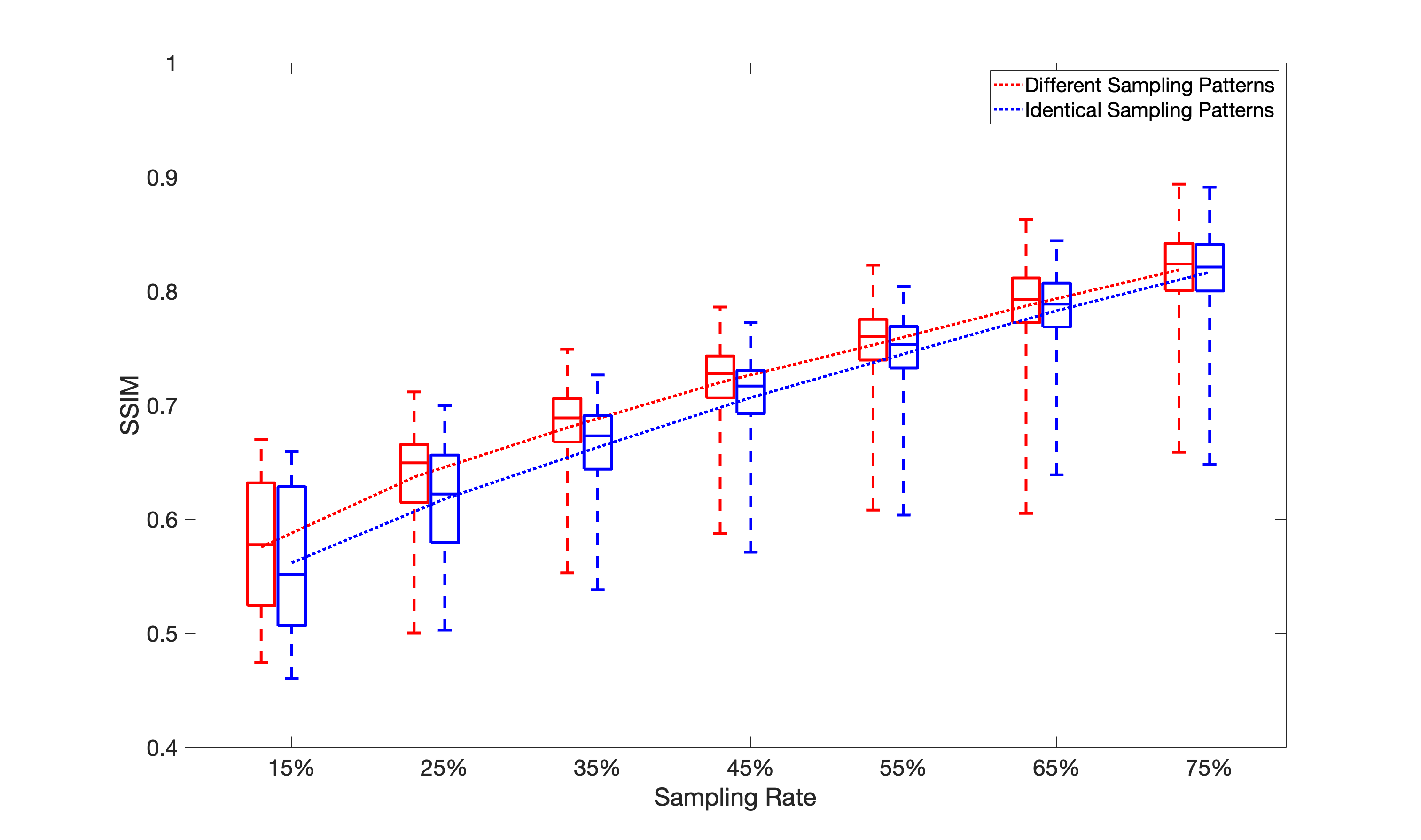
Figure 1 shows two undersampled ADC maps of a representative COPD subject (sampling rate= 35%) along with the fully sampled map (i.e., ground truth). Based on the mean ADC reported in Figure 1, by undersampling the b-values differently, the mean ADC (0.0259± 0.000252 cm2/s) is closer to the reference (0.0263± 0.000201 cm2/s) than it would be by undersampling them identically (0.0257± 0.000317 cm2/s). Figure 2 depicts the average of 200 mean ADC at 7 sampling rates for all subjects (2 COPD, 2 healthy) along with their percent error (=relative error x100). By using the same undersampling patterns (shown as the blue dash-dotted line in Figure 2) for b=0 and b=20 cm2/s, the mean ADC error was underestimated when compared to fully sampled acquisitions. However, using different undersampling patterns slightly reduced this effect (shown as the red dotted line in Figure 2). This improvement is more apparent when sampling rates were under 45% than when sampling rates are above 45%.Diffusion-weighted images, CS reconstructed over the range of sampling rates, showed wide variation in SNR (Figure 3) and SSIM (Figure 4), as previously observed by others for 129Xe ventilation MRI3. It is notable that, no matter the sampling rate, the SNR was always higher in COPD patients, compared to non-smokers (Figure 3), presumably because the lung is less ventilated, concentrating the 129Xe into a smaller volume. In addition, Figure 3 clearly shows that SNR increases as the sampling rate decreases, as expected by the noise-reduction benefits of CS2. More importantly, Figure 4 demonstrates improved SSIM performance in ADC maps derived from differently undersampled b-values when compared to those generated by identically undersampled b-value images.
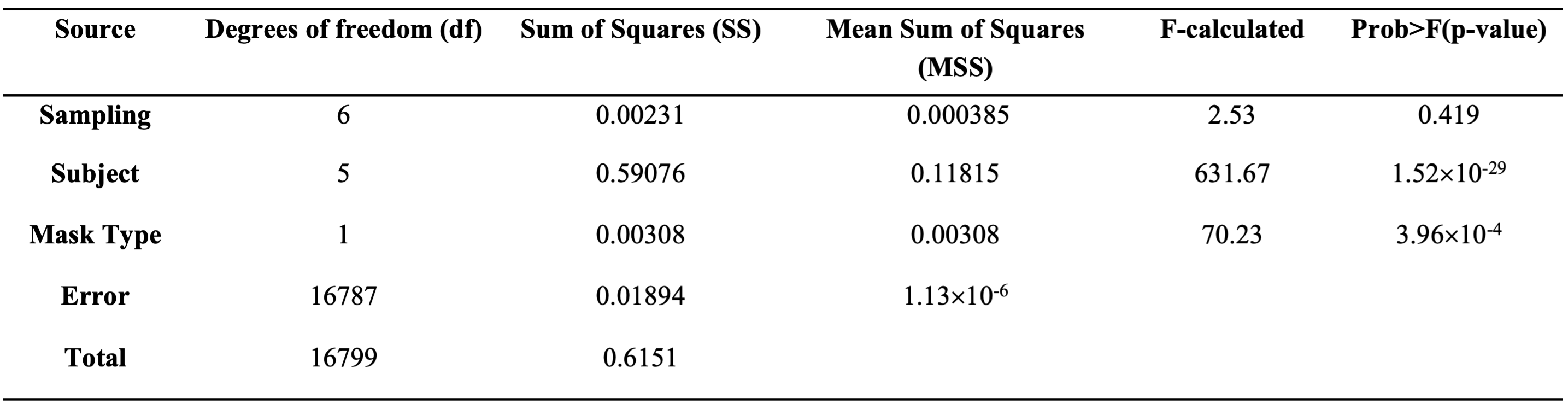
To investigate source(s) of variance, a repeated measures ANOVA (i.e., rmANOVA) was performed to determine whether the patient, sampling pattern, and/or mask type (i.e., same and differing sampling for b=0 and 20 cm2/s) had a significant impact on mean ADC values. As expected, ADC showed a highly significant difference between healthy and COPD patients (p<1.52x10-29) (Table 1). More importantly, with respect to this work, both sampling pattern (p<0.0004) and mask type (i.e., same or different between b-values) (p<0.004) played significant roles in ADC variability (Table 1).
Discussion
More accurate image reconstruction was observed in Figure 2 and Figure 4 by using different undersampling patterns for baseline (i.e., b=0 cm2/s) and diffusion-weighted hyperpolarized 129Xe lung images. The accuracy was improved by having lower mean ADC error and higher SSIM in Figure 2 and Figure 4, respectively. Of importance was the finding that ADC maps generated from b=0 and b=20 cm2/s images undersampled identically show reduced quality, as judged by mean ADC and SSIM, than those derived by differently undersampled b-values. Thus, the optimal undersampling pattern and image reconstruction likely differs between images with different diffusion weightings.Conclusion
Undersampling b-values differently increases the accuracy of the ADC maps compared to identical undersampling since the optimal undersampling pattern varies between diffusion and non-diffusion-weighted images. Moreover, since ADC results are strongly influenced by sampling patterns, optimizing hyperpolarized 129Xe diffusion-weighted MRI using CS requires careful analysis of this factor.Acknowledgements
No acknowledgement found.References
1. Kirby M, et al. (2012) Radiology 265(2):600-610. 2. Lustig M, et al. (2008) IEEE signal processing magazine 25(2):72-82. 3. Chan H-F, et al. (2017) Magn. Reson. Med. 77(5): 1916-1925. 4. Tavakkoli M, et al. (2021) ESMRMB 34:S3.07. 5. Svenningsen S, et al. (2021) Acad. Radiol. 28(6):817-826. 6. Kojima S, et al. (2018) Radiol. Phys. Tech. 11(3):303-319. 7. https://mrirecon.github.io/bart/
Figures