4468
Myocardial changes evaluation based on CMR imaging in patients with obstructive hypertrophic cardiomyopathy after Liwen procedure
Minwen Zheng1 and shuangxin li2
1Department of Radiology, Xijing Hospital, Fourth Military Medical University, Xian, China, 2Department of Radiology, Xijing Hospital, Fourth Military Medical University, xinan, China
1Department of Radiology, Xijing Hospital, Fourth Military Medical University, Xian, China, 2Department of Radiology, Xijing Hospital, Fourth Military Medical University, xinan, China
Synopsis
Keywords: Heart, Cardiovascular
This study evaluated the structural, functional and tissue characteristic changes of myocardium in patients with hypertrophic obstructive cardiomyopathy after treated with the Liwen procedure using cardiac magnetic resonance (CMR) techniques. Compared with pre-operation, one year after treated with Liwen procedure (a new effective procedure), patients’ septal and left ventricular free wall thickness and left ventricular mass (LVM) were significantly reduced. There was no significant change in left ventricular ejection fraction (LVEF) (P>0.05).Introduction:
Hypertrophic obstructive cardiomyopathy (HOCM) is a genetic cardiomyopathy characterized by asymmetric hypertrophy of the ventricular septum with left ventricular outflow tract obstruction. Left ventricular outflow tract obstruction is often associated with mitral regurgitation, which is the pathophysiological basis for symptoms such as exertional dyspnea, angina pectoris, and syncope. The Liwen procedure has been shown to be a safe and effective minimally innovative procedure for relieving left ventricular outflow tract obstruction (1). Cardiac magnetic resonance (CMR) is the gold standard in the evaluation of cardiac function (2), providing a one-stop, noninvasive assessment of the structural, functional, and histological features of the heart. CMR has been used to evaluate postoperative changes in patients with HOCM treated with alcohol septal ablation and surgical myectomy. However, there are almost no studies of the Liwen procedure. Therefore, in this study, we evaluated the structural and functional changes of the myocardium in HOCM patients treated with the Liwen procedure based on CMR imaging.Method:
Patients/Volunteers: Retrospective collected 36 HOCM patients treated with Liwen procedure intervention between September 2016 and June 2022. Scanner and coil: A German Siemens 1.5TArea magnetic resonance imaging system, combined with cardiac gating and an 8-channel abdominal phased-array coil were used to localize and scan the conventional heart. Then standard two-chamber, three-chamber, and four-chamber heart and cine sequences containing short-axis positions of the right and left ventricles were scanned. Data processing: All CMR raw images were sent to the CVI 42 (version 5.13.1, Circle Cardiovascular Imaging, Calgary, Alberta, Canada) software for analysis. End-diastolic and end-systolic were defined on LV short-axis cine images. Endocardium and epicardium were manually depicted (papillary muscles and tendons are part of the ventricular cavity and are not included in the myocardial calculations). Myocardial thickness was measured at the level of the LV papillary muscles in the interventricular septum, anterior wall, lateral wall, and inferior wall. The software automatically calculated LVEF and LVM. The short-axis LGE images were imported into the software tissue characterization module, and the left ventricular inner and outer membrane contours and marked septal onset points were manually outlined on each layer. The region of interest was outlined within the distal normal myocardium, with signal intensity within it as a reference. The software automatically identified the myocardial fibrosis region as the 5 times standard deviation (5SD) higher than the mean signal intensity across reference region. The overall left ventricular myocardium region was divided into two parts, septal and non-septal. The septal myocardial region was defined manually at each layer of the short axis images, resulting in the percentage of non-septal fibrotic myocardium to the overall LV myocardial mass, i.e., non-septal myocardial LGE%. Statistics analysis: For preoperative and postoperative comparisons, paired t-test was used. In all analyses, P<0.05 was considered as statistically significant. All statistical analyses were performed using SPSS version 22.0.0 (IBM Corporation, Armonk, NY, USA).Results:
Compared with the pre-operation, the mean left ventricular outflow tract gradient (LVOTG) difference significantly decreased from 76.36±42.2mmHg to 22±5.22 mmHg one year after surgery (p<0.001) (Figure 1). The thickness of left ventricular free wall and septum were significantly reduced to varying degrees (all p<0.05) (Figure 2). The LVEF did not change significantly (p=0.063). The LVM was significantly reduced (p<0.001) (Figure 3).Discussion:
Previous studies have demonstrated that myocardial hypertrophy in patients with HOCM, which is partly due to the afterload increasing and somewhat reversible, is not entirely genetically determined (3). In contrast with alcohol septal ablation, by the thermal ablation of hypertrophic septum with ultrasound-guided radiofrequency needle puncture directly through the apex of the heart, Liwen procedure cause the coagulative necrosis of hypertrophic myocardial cells, which can lead to a thinning of the septum, release the outflow tract obstruction and improve the previously compensated hypertrophy to some extent (4). The patient's LVM was significantly reduced one year after operation further proved the treatment effect of Liwen procedure.Conclusion:
Liwen procedure can significantly relieve left ventricular outflow tract obstruction and reduce left ventricular myocardial hypertrophy. However, Liwen procedure still cannot reverse the process of my ocardial fibrosis.Summary of main findings:
CMR provides a one-stop assessment of myocardial structural, functional, and histological changes in patients after Liwen procedure treatment.Acknowledgements
No acknowledgement found.References
Liu L, et al. Percutaneous Intramyocardial Septal Radiofrequency Ablation for Hypertrophic Obstructive Cardiomyopathy. J Am Coll Cardiol 2018;72(16):1898-1909. Plana JC, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2014;27(9):911-939. van Dockum WG, et al. Early onset and progression of left ventricular remodeling after alcohol septal ablation in hypertrophic obstructive cardiomyopathy. Circulation 2005;111(19):2503-2508. Zhou M, et al. Percutaneous Intramyocardial Septal Radiofrequency Ablation in Patients With Drug-Refractory Hypertrophic Obstructive Cardiomyopathy. JAMA Cardiol 2022;7(5):529-538.Figures
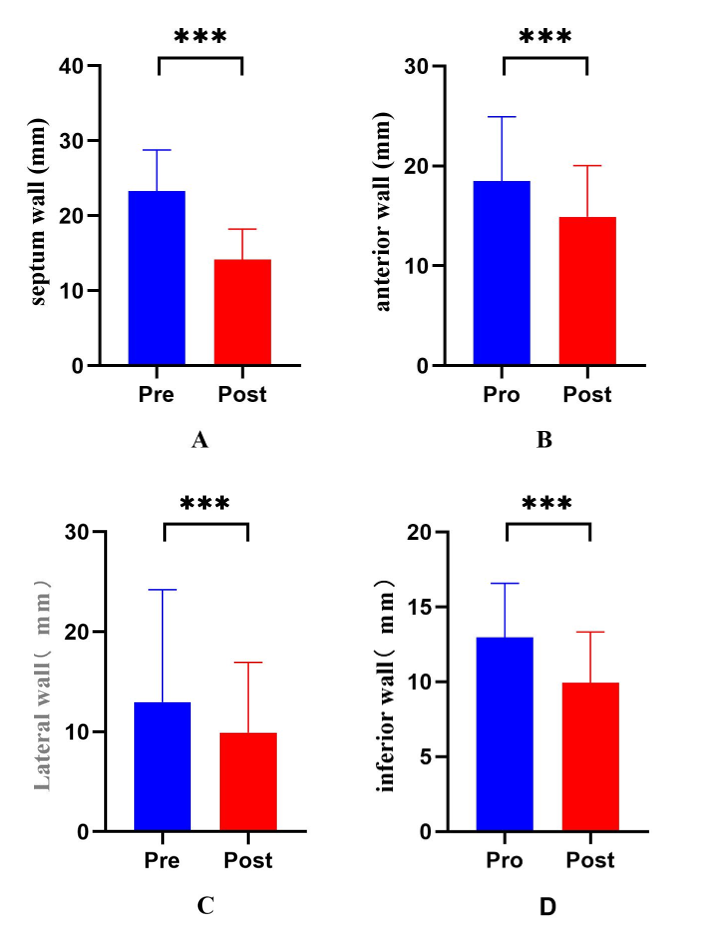
Figure 2 The thickness of the septum(A),
anterior(B), lateral(C) and inferior
(D)walls at the level of the papillary muscle were significantly reduced at
the end of LV diastole (all p<0.05) one year after
operation.
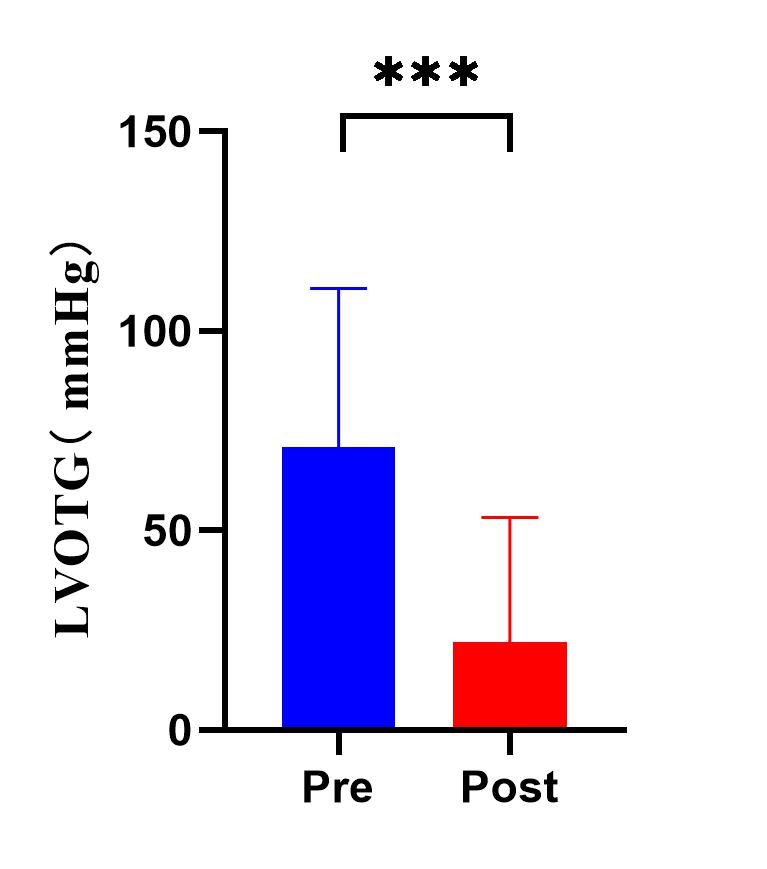
Figure 1The mean LVOTG difference
significantly decreased from 76.36±42.2mmHg to 22±5.22 mmHg one year after surgery (p<0.001).
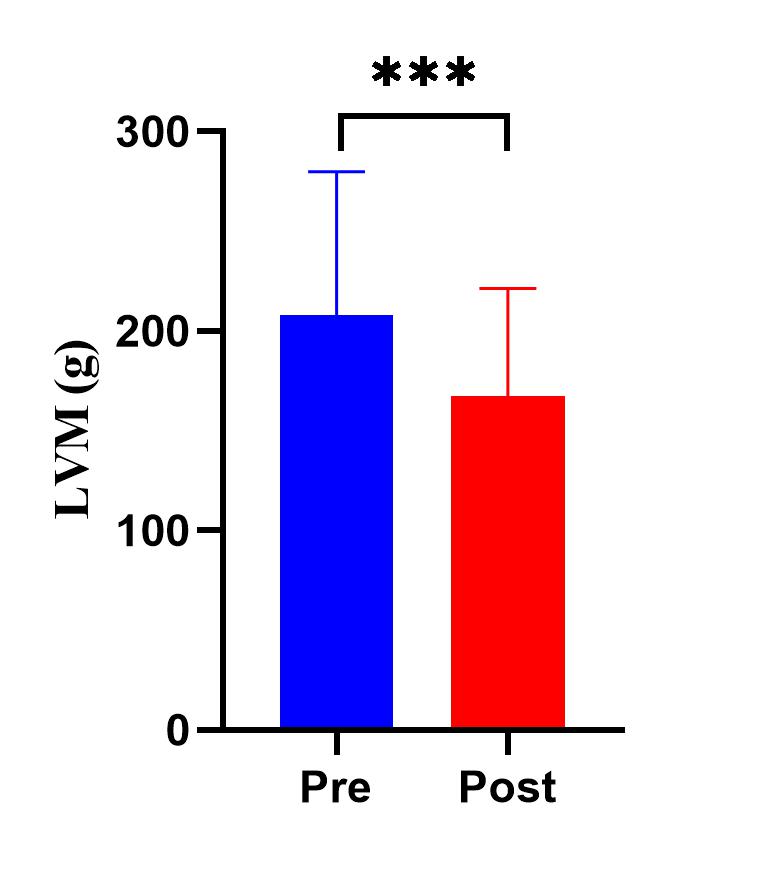
Figure
3 The
mean LVM decreased from (207.78±71.96) g to (167.37±54.1) g (p<0.001) one
year after operation.
DOI: https://doi.org/10.58530/2023/4468