4461
Intravoxel Incoherent Motion Diffusion Weighted MR Imaging to Evaluate Myocardial Microvascular Dysfunction of Exertional Heat Illness12. Department of Radiology, Jinling Hospital, Medical School of Nanjing University, Nanjing, China, 24. MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: Heart, Myocardium
Purpose: To investigate the feasibility of assessing myocardial microvascular perfusion of patients with exertional heat illness (EHI) by intravoxel incoherent motion imaging.
Methods: CMR-IVIM image quality was evaluated with a 3-point scale. CMR-IVIM derived parameters were analyzed and compared between EHI and HC. Receiver operating characteristic curve was used.
Results: CMR-IVIM image quality were significantly improved. EHI patients showed decreased D*, decreased f values and higher D values compared to HC. f showed the most robust efficacy for detecting EHI related myocardial injury with the highest area under the curve.
Conclusion: CMR-IVIM can evaluate myocardial injury of EHI patients.
abstract
Purpose: To investigate the feasibility of myocardial strain curve derived trigger delay (TD) method in cardiac magnetic resonance intravoxel incoherent motion imaging (CMR-IVIM) and in assessing myocardial diffusion and microvascular perfusion of patients with exertional heat illness (EHI).
Material and Methods: 42 male EHI patients with high level outdoor training and 22 male healthy controls (HC) undergoing 3.0-T CMR were prospectively recruited. CMR-IVIM was randomly acquired by conventional TD method (Group A) or myocardial strain curve based TD method (Group B). TD time and the difference were compared in two groups. CMR-IVIM image quality was evaluated with a 3-point scale. CMR-IVIM derived parameters (pseudo diffusion in the capillaries [D*], perfusion fraction [f] and slow apparent diffusion coefficient [D]) were analyzed and compared between EHI and HC. Receiver operating characteristic curve was used. The correlation between IVIM parameters and myocardial biomarkers was investigated.
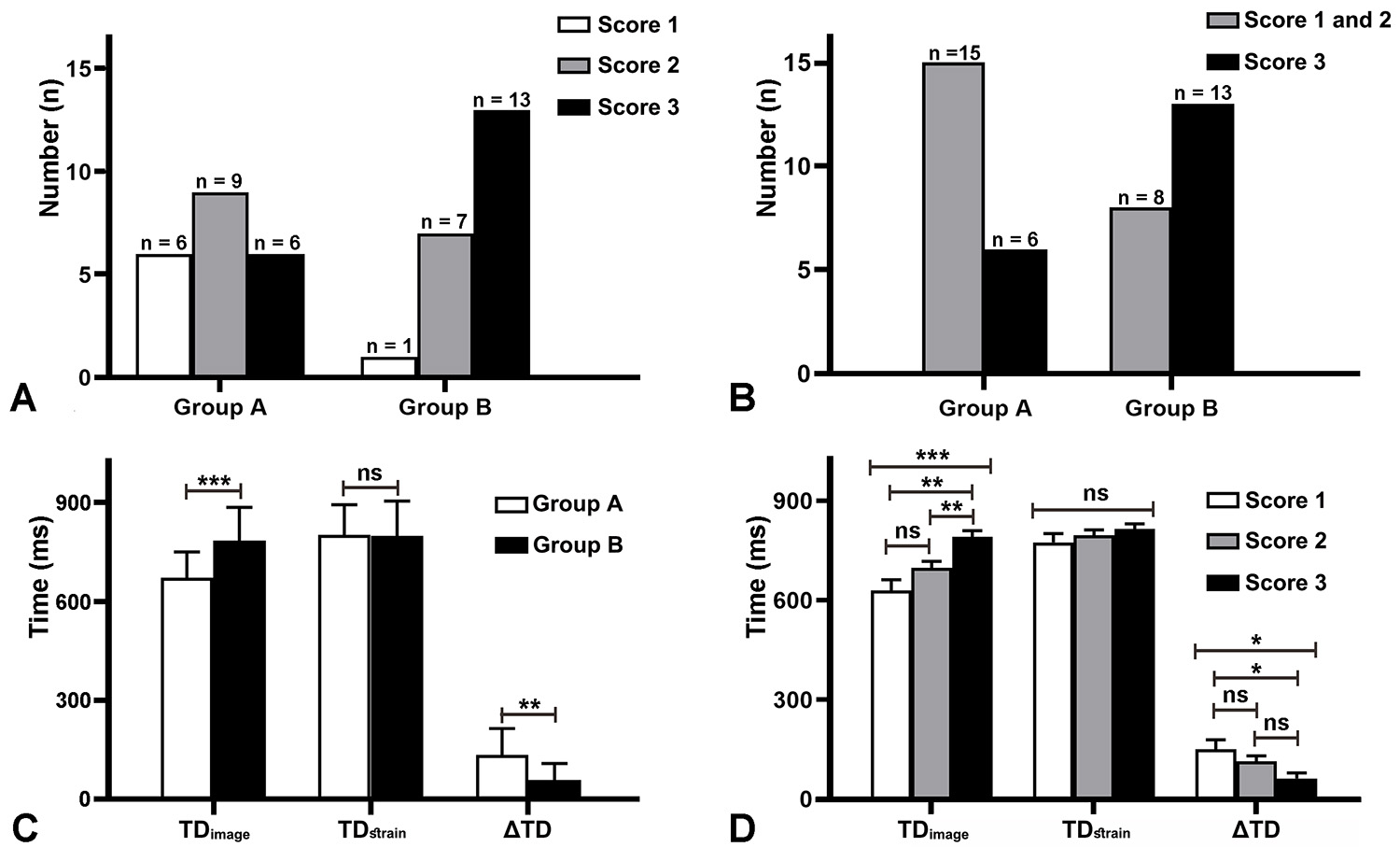
Results: CMR-IVIM image quality (3 [2-3] vs 2 [1-3], P=.014) and technical success rate (score 3) (61.9% [13/21] vs 28.6% [6/21], P = .030) were significantly improved in Group B due to shorter TD difference (133.95 ± 80.11 ms vs 58.38 ± 49.36 ms; P = .001) compared to Group A. EHI patients showed decreased D* (118.13 ± 23.34 x 10-3 mm2/s vs 142.74 ± 42.56 x 10-3 mm2/s, P = .023), decreased f values (0.42 ± 0.12 vs 0.51 ± 0.11; P = .021) and higher D values (2.98 ± 0.87 x 10-3 mm2/s vs 2.54 ± 0.63 x 10-3 mm2/s, P = .009) compared to HC. Relative to D and D*, f showed the most robust efficacy for detecting EHI related myocardial injury with the highest area under the curve (95% confident interval, 0.906: 0.799, 0.967, P<.001) and sensitivity of 88.5% and specificity of 85.6%. f value negatively correlated with creatine kinase-MB isoenzymes (r = -0.532, P = .001) and cardiac troponin I (r = -0.604, P<.001).
Conclusion: Myocardial strain curve based TD method substantially improved image quality and technical success rate of CMR-IVIM, which can evaluate myocardial injury and f value can be an effective biomarker to assess myocardial microcirculation abnormalities of EHI patients.
Acknowledgements
No acknowledgement found.References
1. Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic resonance in myocarditis: A JACC white paper. J Am Coll Cardiol 2009; 53(17): 1475-87.
2. Delattre BM, Viallon M, Wei H, et al. In vivo cardiac diffusion-weighted magnetic resonance imaging: Quantification of normal perfusion and diffusion coefficients with intravoxel incoherent motion imaging. Invest Radiol 2012; 47(11): 662-70.
3. Mou A, Zhang C, Li M, et al. Evaluation of myocardial microcirculation using intravoxel incoherent motion imaging. J Magn Reson Imaging 2017; 46(6): 1818-28.
4. An DA, Chen BH, Rui W, et al. Diagnostic performance of intravoxel incoherent motion diffusion-weighted imaging in the assessment of the dynamic status of myocardial perfusion. J Magn Reson Imaging 2018; 48(6): 1602-9.
5. Terrier B, Dechartres A, Gouya H, et al. Cardiac intravoxel incoherent motion diffusion-weighted magnetic resonance imaging with T1 mapping to assess myocardial perfusion and fibrosis in systemic sclerosis: Association with cardiac events from a prospective cohort study. Arthritis Rheumatol 2020; 72(9): 1571-80.
6. Rapacchi S, Wen H, Viallon M, et al. Low b-value diffusion-weighted cardiac magnetic resonance imaging: Initial results in humans using an optimal time-window imaging approach. Invest Radiol 2011; 46(12): 751-8.
7. Amzulescu MS, De Craene M, Langet H, et al. Myocardial strain imaging: Review of general principles, validation, and sources of discrepancies. Eur Heart J Cardiovasc Imaging 2019; 20(6): 605-19.
8. Claus P, Omar AMS, Pedrizzetti G, et al. Tissue tracking technology for assessing cardiac mechanics: Principles, normal values, and clinical applications. JACC Cardiovasc Imaging 2015; 8(12): 1444-60.
9. Bouchama A, Knochel JP. Heat stroke. N Engl J Med 2002; 346(25): 1978-88.
10. Dronca M, Pasca SP, Nemes B, et al. Cardiac markers (bnp, nt-pro-bnp, troponin i, troponin t, in female amateur runners before and up until three days after a marathon. Clin Chem Lab Med 2008; 46(6): 880-1.
11. Rajiah PS, Kalisz K, Broncano J, et al. Myocardial strain evaluation with cardiovascular mri: Physics, principles, and clinical applications. Radiographics 2022; 42(4): 968-90.
Figures
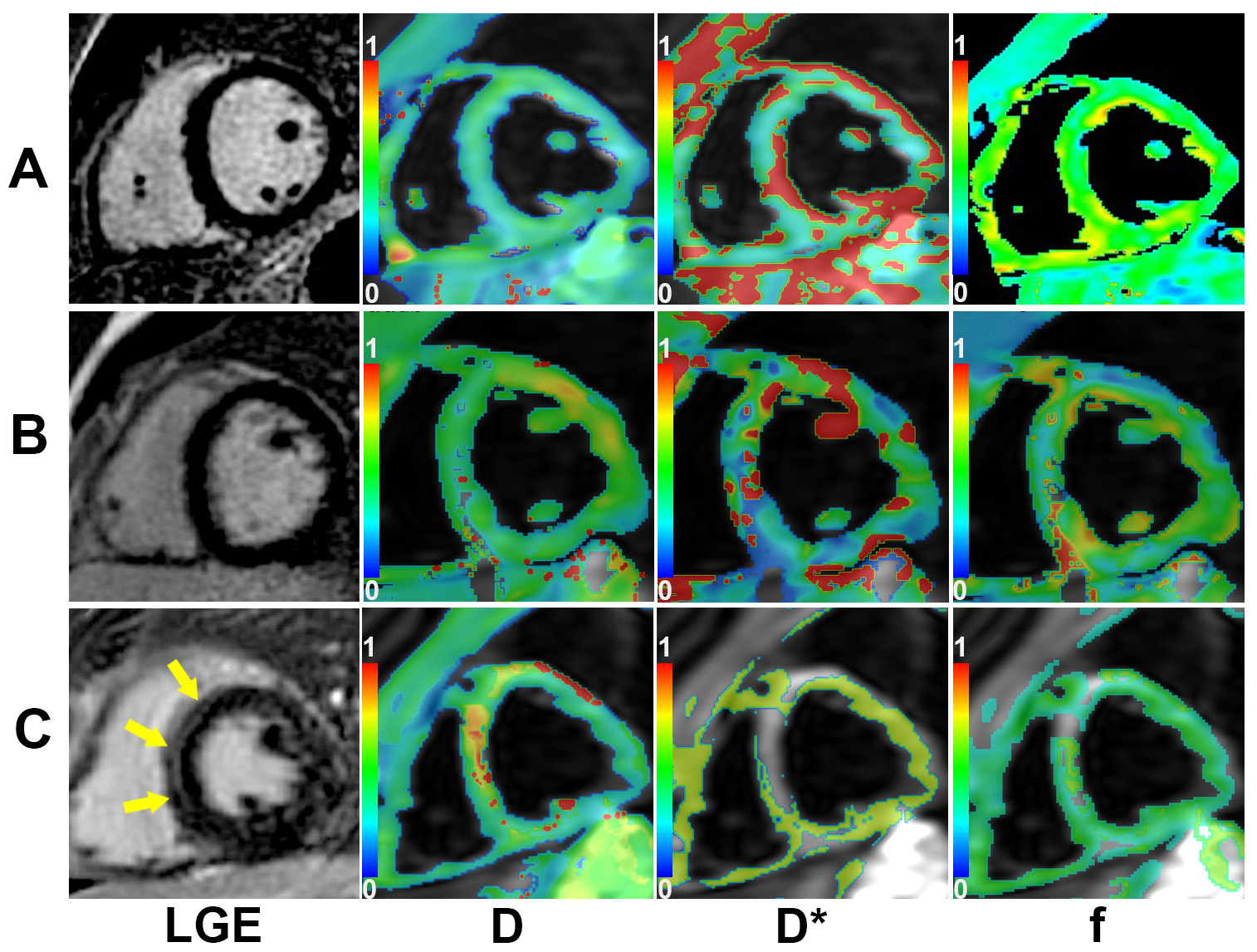
Panel A. A 23-year-old (first row) healthy male had normal LGE image, D value (2.13 x 10-3mm2/s), D* value (152.74 x 10–3 mm2/s) and f value (0.582). Panel B. A 23-year-old male (middle row) with EHI shows negative LGE, but the D value is increased (3.01 x 10-3 mm2/s), while D* value (102.74 x 10–3 mm2/s) and f (0.318) value are reduced. Panel C. A 21-year-old (bottom row) with EHI and positive LGE in the LV septal segment (arrow) had higher D value (3.72 x 10-3 mm2/s), reduced D* value (98.21 x 10–3 mm2/s) and f value (0.286).
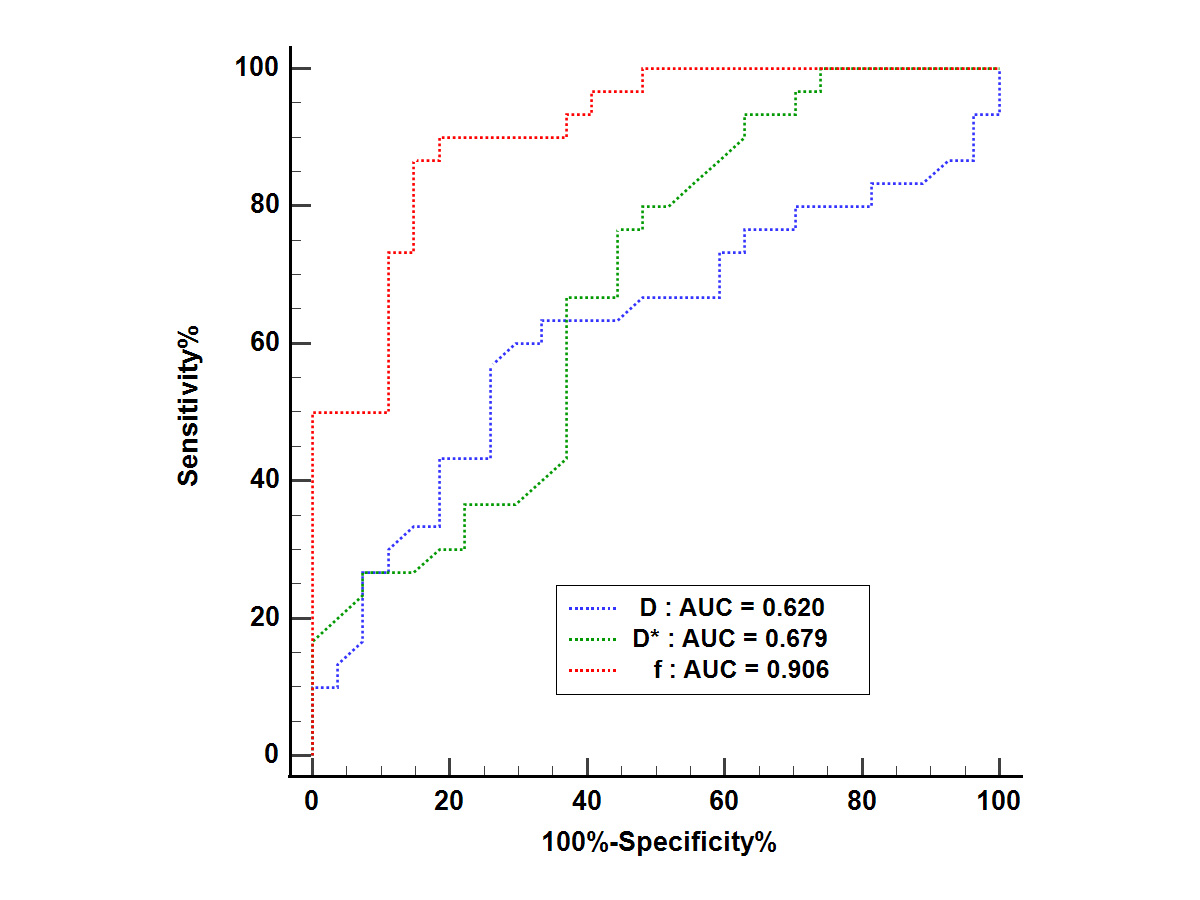
Receiver-operator characteristics curve (ROC) analyses to assess diagnostic performance of CMR-IVIM parameters in the myocardial injury of EHI. AUC = area under the ROC curve.