4354
Accelerated cardiac cine imaging using deep learning: impact on left ventricular function and AI segmentation model1Radiology, The First Hospital of Jilin University, Changchun, China, 2Nuclear Medicine, The First Hospital of Jilin University, Changchun, China, 3Cardiovascular Center, The First Hospital of Jilin University, Changchun, China, 4Philips Healthcare, Beijing, China
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Myocardium, Cardiomyopathy,Data Analysis
Cardiac MRI is considered reference standard for the noninvasive assessment of ventricular volumes and function. However, long multibreath-hold acquisition time can prove difficult in patients and lead to poor image quality. In this study, we investigated the use of a deep learning-based reconstruction algorithm, named Compressed SENSE Artificial Intelligence(CS-AI), to accelerate two-dimensional cine bSSFP for cardiac MRI. The purpose of this study was to compare the image quality and performance of a CS-AI-based cine sequence between reference and accelerated methods: SENSE, Compressed-SENSE, and CS-AI, and then to investigate the impact of images reconstructed by deep learning on AI segmentation model.Introduction
Cardiac magnetic resonance imaging (CMR) is considered a reference standard for the noninvasive assessment of ventricular volumes and function. A multisection two-dimensional cine balanced steady-state free precession(bSSFP) short-axis imaging through the ventricles is obtained over multiple breath holds to mitigate respiratory motion. However, long multi-breath-hold acquisition time can prove difficult in patients, especially those who are unable to comply with breath-holding instructions and lead to poor image quality1. Sensitivity encoding (SENSE) and Compressed-SENSE (CS) can shorten the acquisition time while maintaining the image quality2,3. Moreover, some artificial intelligence approaches have also been shown to accelerate the scan further1. However, some deep neural networks have been recently found vulnerable to the designed input samples which a slightly modified, such as adversarial examples. Thus, the reliable assessment of cardiac volumetric and functional parameters using images reconstructed by deep learning and its impact on other deep learning-based segmentation models are still not very clear. In this study, Compressed SENSE Artificial Intelligence(CS-AI) reconstruction4,5 was used to reduce the noise and optimize the image quality of cine bSSFP. It is hypothesized that cardiac cine imaging with CS-AI reconstruction can reduce scan time while maintaining an accurate assessment of ventricular volumetry, meanwhile having a similar performance on the AI segmentation model compared with images using CS reconstruction. The purpose of this study is to compare the image quality, volumetric and functional parameters of a CS-AI-based cine sequence between SENSE and Compressed-SENSE, and to investigate the impact of images reconstructed by deep learning on other deep learning-based segmentation models.Methods
This prospective study was approved by the local institutional Ethics Committee and written informed consent was obtained from all subjects. 30 adults undergoing cardiac MRI from December 2021 to October 2022 in the local hospital using a 3.0T system (Ingenia Elition, Philips Healthcare).Both conventional and accelerated short-axis bSSFP cine were acquired with the following parameters: FOV = 350×350×92 mm, slice thickness(mm)= 8 mm; matrix size= 196×196; TR/TE(ms)= 2.8/1.40; flip angle(deg) = 45; cardiac phases=25; Breath-holds=4, SENCE/CS acceleration factor =1.8(standard)/4,scan time=10-11(SENCE1.8)/7-9(CS4)sec: depends on the heartbeat. The short-axis cine images were analyzed from images reconstructed by SENSE,CS and CS-AI(denoising level=strong).In the CS-AI reconstruction, the CS reconstruction chain was replaced by a lot of convolution neural network (CNN) reconstruction. Two radiologists scored overall image quality of all short-axis stacks on a five-point Likert scale, of which 5 score represented excellent image quality, while 1 score represented poor. All CMR parameters of left ventricular(LV) volume and function were measured using dedicated software (Cvi42 , Circle Cardiovascular Imaging, Calgary, Canada), which was completed by experienced operators without knowledge of the clinical data and scanning parameters. The segmentation of endocardial and epicardial contours of the left or right ventricle were completed automatically using a deep learning-based segmentation model. The Dice index was used to measure the accuracy of the segmentation output (LV endocardium and epicardium, RV endocardium) . The Friedman test, and one-way ANOVA were performed to test the CMR data derived from different sequences. The difference in image quality scores were compared with the Wilcoxon rank-sum test.Results and Discussions
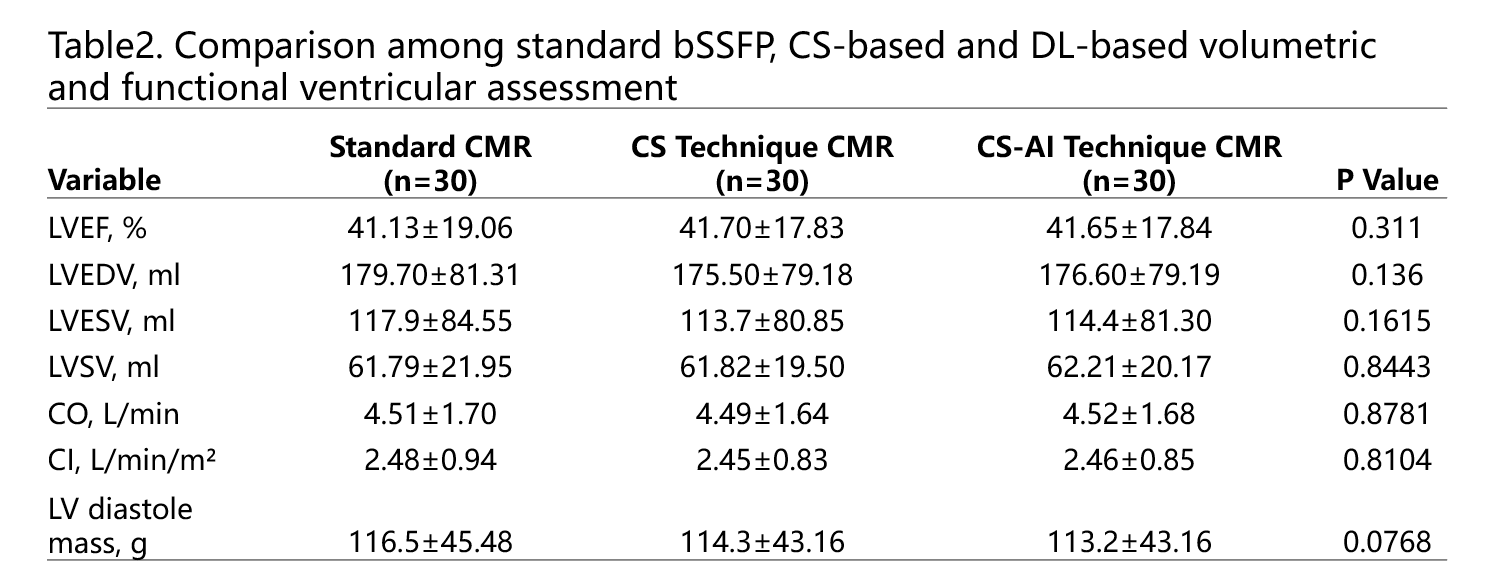
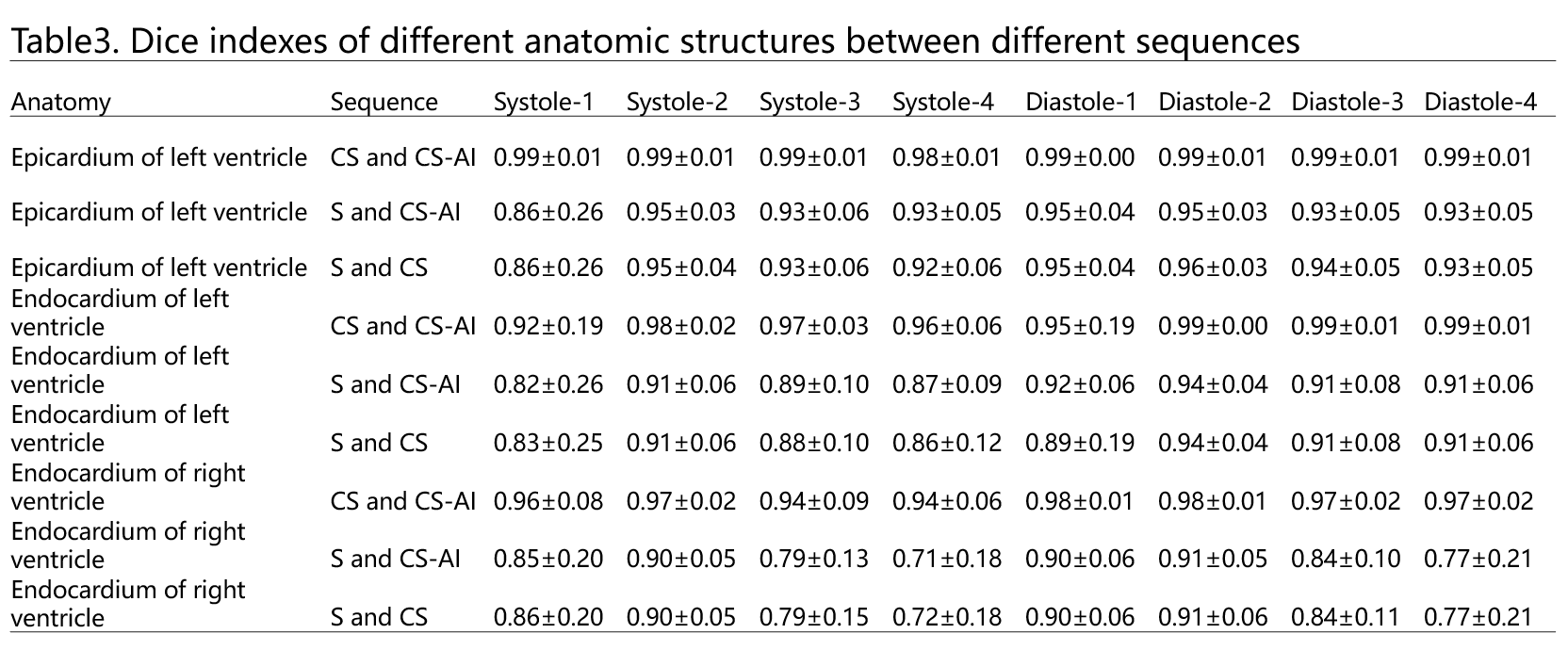
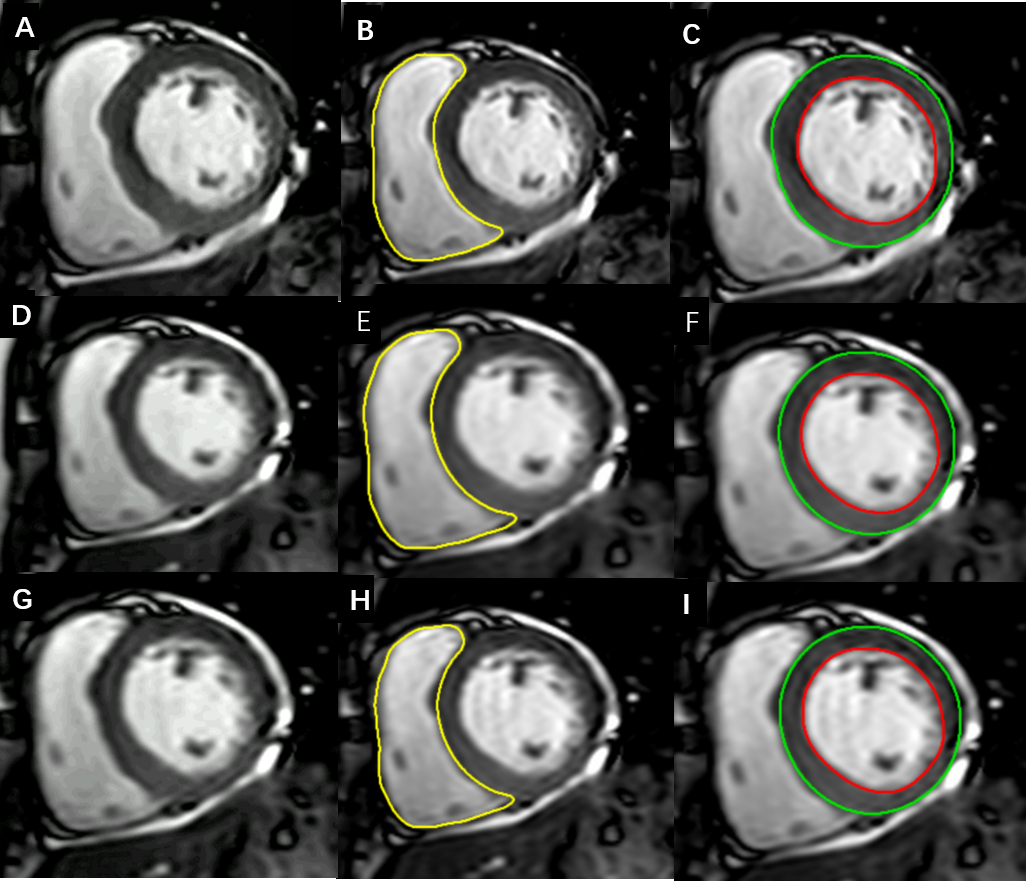
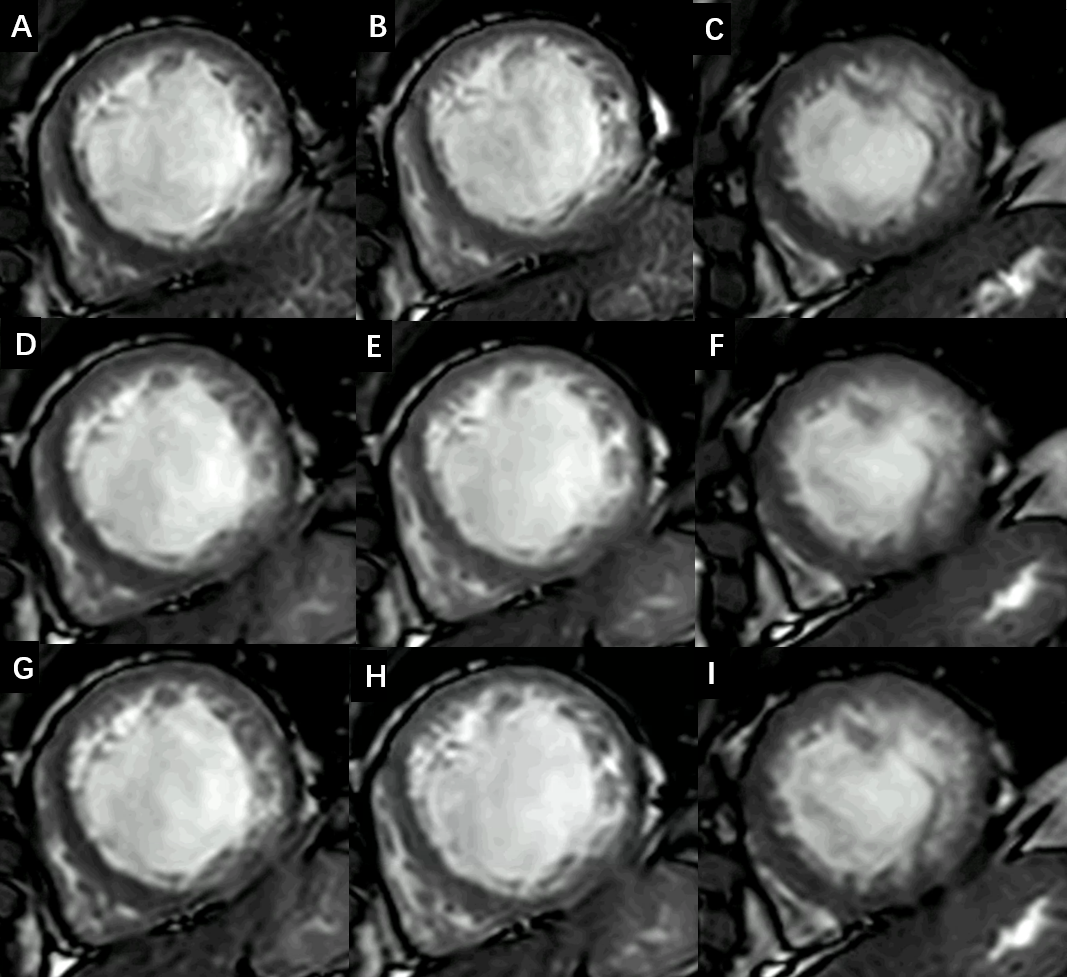
30 participants (mean age 50.13 years, range 23–76 years; 18 men) were evaluated, Table1. shows the patient’s demographics and baseline characteristics. Overall image quality scores were 4.39 ± 0.64(CS-AI 4),4.15 ± 0.67(CS4)versus 4.62 ± 0.50(SENCE 1.8)(all P< 0 .05). All CMR parameters of LV volume and function acquired from sequences reconstructed by CS 4 and CS-AI4 had no statistical difference with standard bSSFP(Table2). Table 3. Shows the Dice indexes of different anatomic structures between different sequences. For the endocardial and epicardial contours of left ventricle, all of the Dice indexes were very high between CS and CS-AI(>0.90),and also high between SENCE and CS,SENCE and CS-AI(>0.80); But for the endocardial contours of right ventricle, the Dice indexes were very high only between CS and CS-AI(>0.90), while between SENCE and CS,SENCE and CS-AI, some Dice indexes were lower than 0.80. These results may reflect the morphologic changes of right ventricle and its thin wall could affect the performance of AI segmentation model. Figure1 and 2 show cardiac cine bSSFP short-axis imaging reconstructed with SENCE, CS and CS-AI, the images reconstructed with CS-AI show better image quality than CS.Conclusion
The results demonstrated the feasibility of applying the CS-AI reconstruction to evaluate cardiac function with high accuracy in patients. The images reconstructed by CS-AI has little impact on the performance of AI segmentation model.Acknowledgements
No acknowledgement found.References
1. Zucker Evan J, Sandino Christopher M, Kino Aya et al. Free-breathing Accelerated Cardiac MRI Using Deep Learning: Validation in Children and Young Adults.[J] .Radiology, 2021, 300: 539-548.
2. Vincenti Gabriella,Monney Pierre,Chaptinel Jérôme et al. Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass.[J] .JACC Cardiovasc Imaging, 2014, 7: 882-92.
3. Chen Xiao,Yang Yang,Cai Xiaoying et al. Accelerated two-dimensional cine DENSE cardiovascular magnetic resonance using compressed sensing and parallel imaging.[J] .J Cardiovasc Magn Reson, 2016, 18: 38.
4. Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access. 2020;8:204825-204838.
5. Pezzotti N, de Weerdt E, Yousefi S, et al. Adaptive-CS-Net: FastMRI with Adaptive Intelligence. arxiv. 2019;(NeurIPS).
Figures
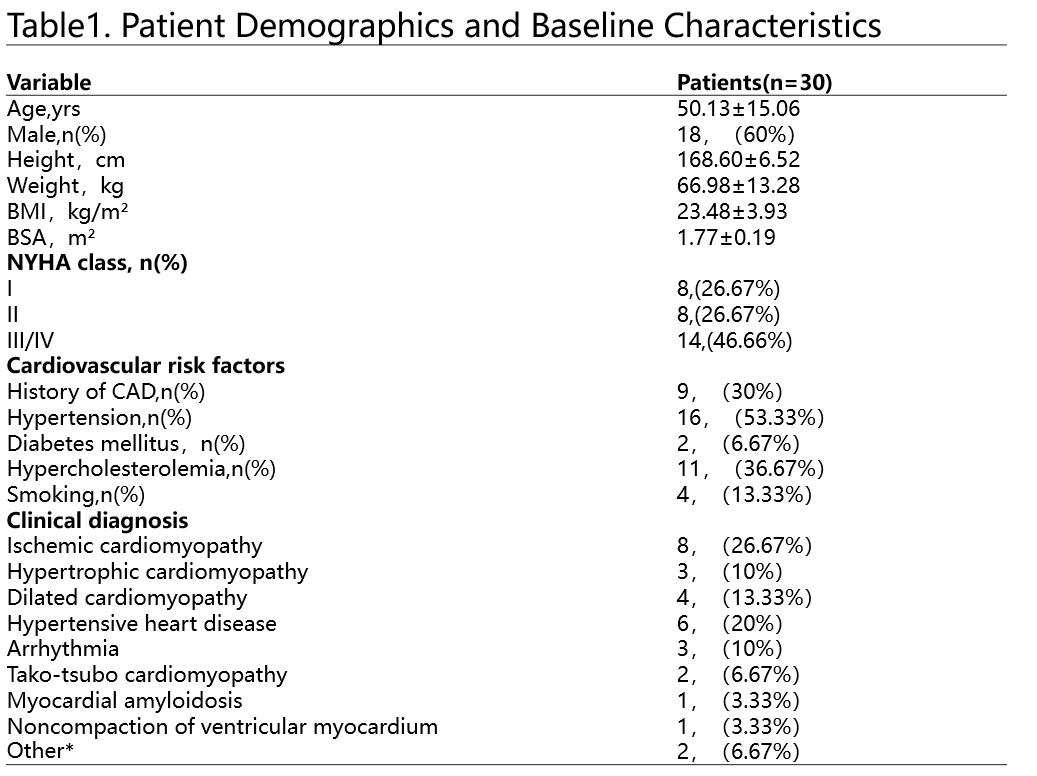
Values are expressed as either mean± SD or number(percentage).*patients with other diseases,such as hematological disease, or symptom of dyspnea,palpitation,pectoralgia.BMI =body mass index; BSA =body surface area; CAD = coronary artery disease.