4305
Free-water DTI and cognitive performance in patients with intracranial vascular occlusion disease and transient ischemic attack1Shanghai Key Laboratory of Magnetic Resonance, School of Physics and Electronic Science, East China Normal University, Shanghai, China, 2Department of Neurosurgery, Tong Ji Hospital, School of Medicine, Tong Ji University,, Shanghai, China
Synopsis
Keywords: Data Analysis, Diffusion Tensor Imaging, free-water elimination DTI
The objective of this study was to explore the relationship between cognitive impairment and free-water elimination DTI (FWE-DTI) metrics in patients with intracranial vascular occlusion disease (IVOD) and transient ischemic attack (TIA). 22 IVOD with TIA patients were tested with cognitive scales and scanned using a 3T echo-planar imaging sequence. The results show global FWE-DTI metrics were associated with patients' cognitive performance in some domains, which indicated the potential of FWE-DTI as new indices for assessing global brain changes in this disease.Introduction
Patients with intracranial vascular occlusion disease (IVOD) and transient ischemic attack (TIA) showed evidence of cognitive impairment,which has been demonstrated associating with microstructural changes in white matter (WM) using diffusion tensor imaging (DTI) 1-3. However, these conventional DTI metrics can be further refined by isolating the effects of extracellular free water (FW) by a the free-water elimination DTI (FWE-DTI) model4. The aim of this study was to explore the relationship of FWE-DTI measurements with cognitive functions.Materials and Methods
Being excluded from other cerebrovascular diseases, a total of 22 IVOD and TIA patients with a mean age of 54.00±11.12 years old have been enrolled in this study.The cognitive tests focused on the domains including memory, language capability, and executive function. Montreal Cognitive Assessment-Basic (MoCA-B) and Mini-Mental State Examination (MMSE) were employed for cognition functions. Ability of daily living was assessed by the Instrumental Activities of Daily Living scale (IADL-14). In addition, mental health scales were comprised of the Hamilton Depression Rating Scale (HAMD-7), Hamilton Anxiety Scale (HAMA), and Neuropsychiatric Inventory (NPI).
All the patients were scanned on a 3T MRI system (Prisma Fit, Siemens Healthcare, Erlangen, Germany) with a 64-channel head coil. The DTI data were acquired using an echo-planar imaging sequence with 64 non-collinear directions at b=1000 s/mm2 and one unweighted image at b= 0 s/mm2. Scanning parameters were as follows: repetition time (TR) = 8500 ms, echo time (TE) = 63 ms, field of view (FOV) = 224× 224 mm2, matrix size =112 × 112, flip angle = 90°, Number of slices = 75, and slice thickness = 2 mm.
DTI data were preprocessed using FMRIB’s Software Library (FSL) (www.jiscmail.ac.uk/lists/fsl.html) 5. Eddy and head motion were corrected using the FSL function with the reference volume set as the default 0. An open-source library diffusion in python (DIPY) were used for DTI image reconstruction. The conventional FA and MD maps were calculated from the data using weighted linear least-squares fitting model. Free-water maps were fitted by a two-compartmental model using the regularized gradient descent algorithm 6. Meanwhile, the FWE-DTI model was applied to generate FW-corrected fractional anisotropy (FAt) and mean diffusivity (MDt) maps4. Tract-based spatial statistics (TBSS) in the FSL6 was applied to analyze standard DTI and FWE-DTI imaging indices for WM. Mean global DTI metrics were calculated within the skeleton for each subject.
The relationship between DTI metrics and cognitive performance was calculated by Pearson correlation coefficient. All results were considered statistically significant with a two-tailed p-value of less than 0.05. Statistical analysis was performed using IBM SPSS statistics 22.
Results
Table 1 shows the median and interquartile range (IQR) of cognitive measurements. According to the standards of grading provided in each test manual, patients with MoCA-B median score of 14 and MMSE median score of 25 could be considered as cognitive impairment. IADL-14 median score is 16, which indicated decreased daily life skills. For memory, both delay recall median scores (5 mins delay recall socre = 3, 5 mins delay recall score = 4) lower than instance recall(16.5). For language, both scales median score reflects lower capabilities than normal. Trail Making Test (TMT) are negatively scored where higher scores denote poor performance. According to the median scores of HAMD, HAMA, and NPI, there is a tendency to be anxious but no depression so far.Table 2 summarizes the relationships between neuropsychological test scores and global DTI metrics. Higher global FW is associated with worse MoCA-B (r=-0.474, p=0.026), MMSE (r=-0.591, p=0.005), HVLT-R1 (r=-0.642, p=0.002), LMA (r=-0.663, p=0.001), and VFT (r=-0.602, p=0.005) scores. Similar results are totally found for MD and MDt. The opposite results are present in FA and FAt. In the contrast, FW is proportionate to IADL-14 (r=0.508, p=0.019), TMT-A (r=0.616, p=0.008), and TMA-B (r=0.633, p=0.006), as well as MD, while FA and FAt are in direct contradiction to it. Further analysis shows that the association is stronger(higher r values) for FAt with MoCA-B, IADL-14, TMT-A, and HAMA than FA with them.
Discussion and Conclusion
FW is a sensitive marker of subtle neuroinflammation, but here we identify a relationship between global FW and cognitive performance in the IVOD with TIA. Both FW and FAt of the diffusion signal were associated with patients' cognitive impairment, which reinforces the potential of FWE-DTI as a useful imaging contrast.FA more likely reflects disruptions to white matter microstructure, and is more affected by TIA demonstrated by prior studies.1,7 As a result, global FA and FAt measures were more associated with cognitive performance than FW or MD.
However, we haven’t found enough evidence that FWE-DTI was more sensitive to predict TIA cognitive performance, probably because we used global mean values to describe the changes of the whole brain, which could not precisely detect the change of the local lesion. Since patients have different infarcted areas, region of interest analysis for the local focus area of each patient will be expected to be applied in the future.
In a conclusion,our present results declared that DTI with FW correction is related to IVOD with TIA patients' cognitive performance,and it provides a new metric for assessing global brain changes in the disease.
Acknowledgements
References
1. Kern KC, Wright CB, Leigh R. Global changes in diffusion tensor imaging during acute ischemic stroke and post-stroke cognitive performance. J Cereb Blood Flow Metab. 2022;42(10):1854-66.2. Tariq S, Tsang A, Wang M, Reaume N, Carlson H, Sajobi TT, et al. White matter tract microstructure and cognitive performance after transient ischemic attack. PLoS One. 2020;15(10):e0239116.
3. Guo J, Wang S, Li R, Chen N, Zhou M, Chen H, et al. Cognitive impairment and whole brain diffusion in patients with carotid artery disease and ipsilateral transient ischemic attack. Neurol Res. 2014;36(1):41-6.
4. Pasternak, O.; Sochen, N.; Gur, Y.; Intrator, N.; Assaf, Y. Free water elimination and mapping from diffusion MRI. Magn. Reson. Med. 2009, 62, 717–730
5. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. FSL. Neuroimage 2012;62(2):782-790
6. Golub M, Neto Henriques R, Gouveia Nunes R. Free-water DTI estimates from single b-value data might seem plausible but must be interpreted with care. Magn Reson Med. 2021;85(5):2537-51.
7. Ferris JK, Edwards JD, Ma JA, Boyd LA. Changes to white matter microstructure in transient ischemic attack: A longitudinal diffusion tensor imaging study. Hum Brain Mapp. 2017;38(11):5795-803.
Figures
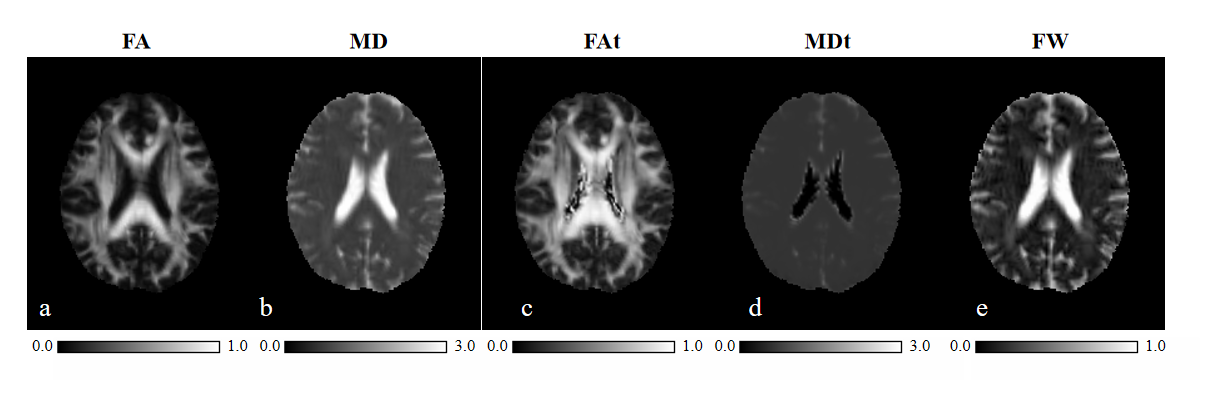
Figure 1. Scalar maps estimated from DTI data acquired from one of the petients in the study.fractional anisotropy (FA) and mean diffusivity (MD) , using standard DTI (first and second column); FW-corrected fractional anisotropy (FAt) and mean diffusivity (MDt) , free water fraction (FW) , using free-water elimination DTI ( third to fifth columns)
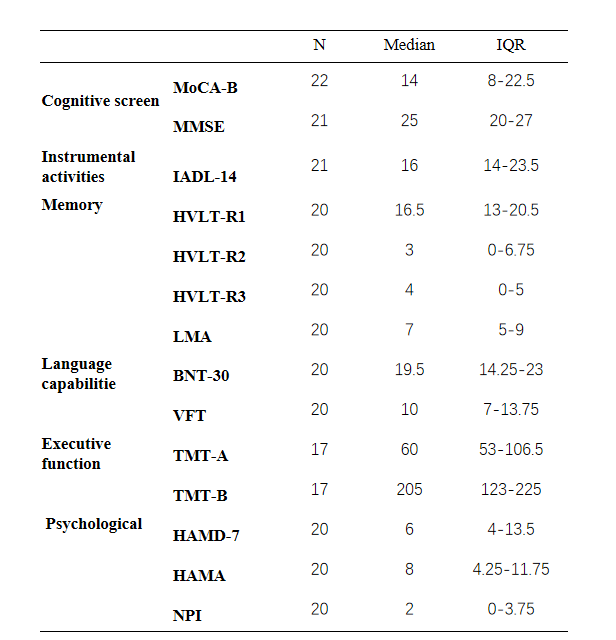
Table 1. Cognitive measures on IVOD patients with TIA. IQR: interquartile range; MoCA-B: Montreal Cognitive Assessment Basic; MMSE: Mini-Mental State Examination; IADL-14: Instrumental Activities of Daily Living scale; HVLT-R: Hopkins Verbal Learning Test(1=instant recall; 2=5 mins delay recall; 3=20 mins delay recall); LMA: Wechsler Memory Scale-Revised Logical Memory Story; BNT-30: Boston Naming Test (30 items); VFT: Vegetable Fluency Test; TMT:Trail Making Tests; HAMD: Hamilton Depression Rating Scale; HAMA: Hamilton Anxiety Scale; NPI: Neuropsychiatric Inventory.
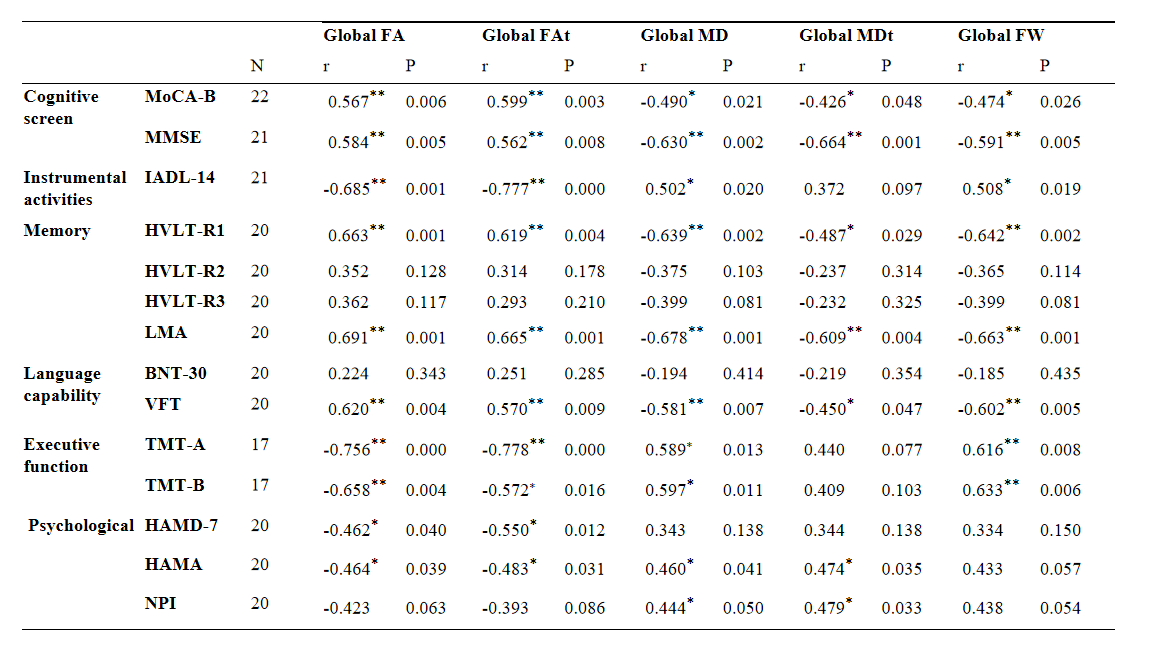
Table 2. Bivariate correlation analysis between global DTI metrics and cognitive performance. r: Pearson correlation coefficient; **. P< 0.01(two-tailed test) *. P<0.05(two-tailed test)