4293
Wideband bright- and black-blood late gadolinium enhancement imaging for patients with cardiac implantable electronic device1IHU LIRYC, Electrophysiology and Heart Modeling Institute, Université de Bordeaux – INSERM U1045, Pessac, France, 2Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 3Department of Cardiovascular Imaging, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Pessac, France, 4Department of Cardiac Pacing and Electrophysiology, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Pessac, France, 5CIBM Center for Biomedical Imaging, Lausanne, Switzerland
Synopsis
Keywords: Myocardium, Tissue Characterization, Metallic device
Conventional LGE PSIR provides very good contrast between healthy and scar tissue, but scar patterns may be confused with blood signal. Joint LGE bright- and black-blood imaging allows for improved scar contrast and detailed cardiac anatomy. However, many patients with cardiac implantable electronic device (CIED) do not undergo cardiac imaging due to severe hyperintensity artefacts. Here we propose a technology to image myocardial scars with unprecedent scar contrast in patients with CIED by combining bright- and black-blood SPOT imaging with wideband MRI. We showed that wideband SPOT can suppress CIED-related hyperintensity artefacts, while maintaining improved scar contrast and localization.
Introduction
Late gadolinium enhancement (LGE) is the current gold standard imaging technique for the assessment of myocardial scars1. Although it provides very good contrast between healthy and scar tissue, scar patterns may be confused with blood signal, resulting in ambiguities in scar detection. A novel imaging technique, termed SPOT2, combines bright- (BR) and black- (BL) blood imaging in a single sequence to obtain images that removes this ambiguity and with improved myocardial contrast and scar localization. However, many patients with cardiac implantable electronic device (CIED) do not undergo cardiac LGE imaging due to severe regional hyperintensity artefacts3 induced by the devices. Here we propose a technology to enable imaging of myocardial scars with unprecedent scar contrast in patients with CIED by combining joint bright- and black-blood SPOT imaging with wideband MRI3.Methods
Acquisition: SPOT2 is a single-shot ECG-triggered sequence that collects BR and BL images in an interleaved fashion (Fig.1A). In odd heartbeats, BL images (providing better scar detection) are generated by a non-selective adiabatic hyperbolic secant (HS) 180° inversion recovery (IR) pulse followed by a T2 preparation module (T2p). In even heartbeats, BR images (providing better scar localization) are collected by only playing out a T2p. The T2p (duration=26.6ms) consists of a 90° tip-down pulse, of two adiabatic HS refocusing pulses, and of a 90° tip-up5. A crusher gradient removes all residual transverse magnetization.To eliminate the hyperintensity artefacts from the non-properly inverted myocardium signal in the presence of CIED, the IR bandwidth was increased from 0.8 to 9.2kHz (Fig.1BC) with a peak B1 amplitude of 30μT. The IR duration was set to 10.24ms. This wideband IR was implemented in the existing reference 2D phase-sensitive inversion recovery (PSIR)1 and in 2D SPOT,2 referred to as wideband IR SPOT. To further reduce CIED-related artefacts, the bandwidth of the two T2p refocusing pulses were also increased from 1.6 to 5kHz (Fig.1BD) with a peak B1 amplitude of 30μT. This method is referred to as wideband IR+T2 SPOT hereafter. To eliminate bSSFP-associated banding artefacts in the presence of CIED, a gradient echo readout was used for both PSIR and SPOT4.
Experiments and analysis: The proposed sequence was tested in the ISMRM-NIST phantom (QualibreMD) and in one patient implanted with a CIED. The following parameters were used for all sequences: FOV=300mm2, resolution=1.4x1.4mm2, slice thickness=8mm, TE/TR=2.7/4.8ms, flip angle=15°, readout bandwidth=751Hz/pixel, 5 signal averages. All experiments were performed on a 1.5T system (MAGNETOM Aera, Siemens). The phantom study was conducted to test the effect of wideband IR SPOT and wideband IR+T2 SPOT, with an inversion time TI=200ms. Wideband SPOT was then compared to wideband PSIR, with TI=450ms for PSIR. A CIED was taped on the side of the phantom (Fig.2A). The extent of the artefact was measured on coronal images. Percentage artefact reduction was evaluated as the percentage reduction in banding and hyperintensity artefacts of each wideband sequence compared to the sequence without wideband. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated. CNR was calculated in two phantom vials with T1/T2 values characteristic of human myocardium (green tube in Fig.3A) and scar (pink tube in Fig.3A). Finally, reference PSIR and wideband IR+T2 SPOT were tested in a cardiac patient implanted with a pacemaker, 15min after injection of 0.2 mmol/kg gadolinium-contrast based agent.
Results
In the presence of CIED, SPOT and reference PSIR provide phantom images with banding, hyperintensity artefacts and signal voids (Fig.2AB). The extent of the signal void for all sequences corresponded to 7.8cm compared to ICD-free imaging without artifacts. The artefact extent with wideband PSIR decreased from 14.5 to 7.8cm (white arrows, Fig.2A), with hyperintensity artefacts entirely suppressed but remaining signal void (7.8 cm extent) (Fig.2A). CNR slightly improved with wideband PSIR whereas SNR slightly decreased (Fig.3A). The artefact extent in conventional SPOT BL and BR was of 14.5cm and 12cm, respectively. Wideband IR SPOT reduced the artefact extent to 11.7cm on BL images but with remaining hyperintensity artefacts (91% reduction). As expected, wideband IR had no effect on BR images. However, wideband IR+T2 SPOT reduced the artefact extent on both BL and BR images to 7.8cm, with suppressed hyperintensity and banding artefacts. CNR slightly decreased for wideband IR SPOT and wideband IR+T2 SPOT on both BL and BR images. SNR was similar for conventional, wideband IR and wideband IR+T2 on BL and BR images. Overall, wideband IR+T2 SPOT performed as good as wideband PSIR for the reduction of hyperintensity artefacts, but with a much higher CNR on BR and BL images and higher SNR on BR images.In the patient, banding and hyperintensity artefacts are present when using conventional PSIR but were successfully suppressed with wideband IR+T2 SPOT (Fig.4).
Conclusion
Wideband IR+T2 SPOT can suppress hyperintensity and banding artefacts on both black- and bright-blood images compared with conventional PSIR and wideband IR SPOT, making it a promising technique for scar assessment in patients with CIED. In vivo clinical testing is now warranted.Acknowledgements
This research was supported by funding from the French National Research Agency under grant agreements Equipex MUSIC ANR-11-EQPX-0030, ANR-21-CE17-0034-01, Programme d’Investissements d’Avenir ANR-10-IAHU04-LIRYC, and ANR Chaire Professeur Junior and from the European Council under grant agreement ERC n715093. A.B. acknowledges a Lefoulon-Delalande Foundation fellowship administered by the Institute of France.References
1. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002 Feb; 47(2):372-83. doi: 10.1002/mrm.10051. PMID: 11810682; PMCID: PMC2041905.
2. Bustin A, Sridi S, Maillot A, et al. Improved myocardial scar visualization with two-minute free-breathing joint bright- and black-blood lategadolinium enhancement imaging. In: Proceedings from the Joint Annual Meeting ISMRM-ESMRMB. ; 2022:0271.
3. Rashid S, Rapacchi S, Vaseghi M, Tung R, Shivkumar K, Finn JP, Hu P. Improved Late Gadolinium Enhancement MR Imaging for Patients with Implanted Cardiac Devices. Radiological Society of North America. 2014 Jan;270(1):269-74. doi: 10.1148/radiol.13130942. Epub 2013 Oct 28. PMID: 24086074; PMCID: PMC4228714.
4. Rashid S, Rapacchi S, Shivkumar K, Plotnik A, Finn JP, Hu P. Modified wideband three-dimensional late gadolinium enhancement MRI for patients with implantable cardiac devices. Magn Reson Med. 2016 Feb;75(2):572-84. doi: 10.1002/mrm.25601. Epub 2015 Mar 13. PMID: 25772155; PMCID: PMC4661130.
5. Nezafat R, Stuber M, Ouwerkerk R, Gharib AM, Desai MY, Pettigrew RI. B1-insensitive T2 preparation for improved coronary magnetic resonance angiography at 3 T. Magn Reson Med. 2006 Apr;55(4):858-64. doi: 10.1002/mrm.20835. PMID: 16538606.
Figures
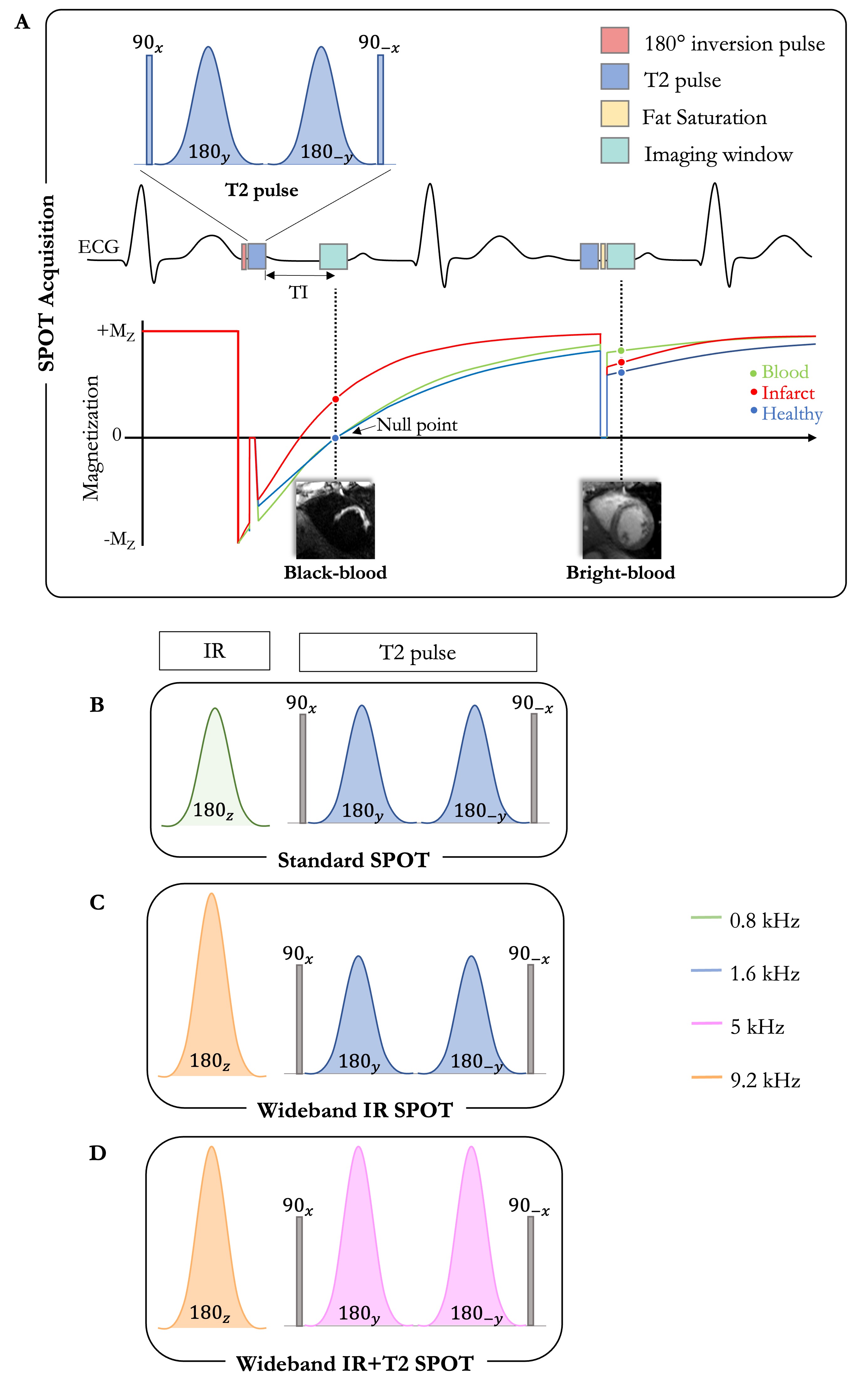
Fig.1. Framework A. SPOT: In odd heartbeats, a black-blood image is obtained by a 180° IR followed by an adiabatic T2p. In even heartbeats, only a T2p is applied to get a bright-blood image. B. Standard SPOT applies IR and T2p refocusing pulses with standard BW of 0.8 and 1.6kHz, respectively. C. Wideband IR SPOT applies IR with BW=9.2kHz and amplitude of 30μT. D. Wideband IR+T2 SPOT applies IR and T2p refocusing pulses with BW= 9.2 and 5kHz, respectively, and amplitude of 30μT. Abbreviations: IR, inversion recovery; Mz, longitudinal magnetization; TI, inversion time; BW, bandwidth.
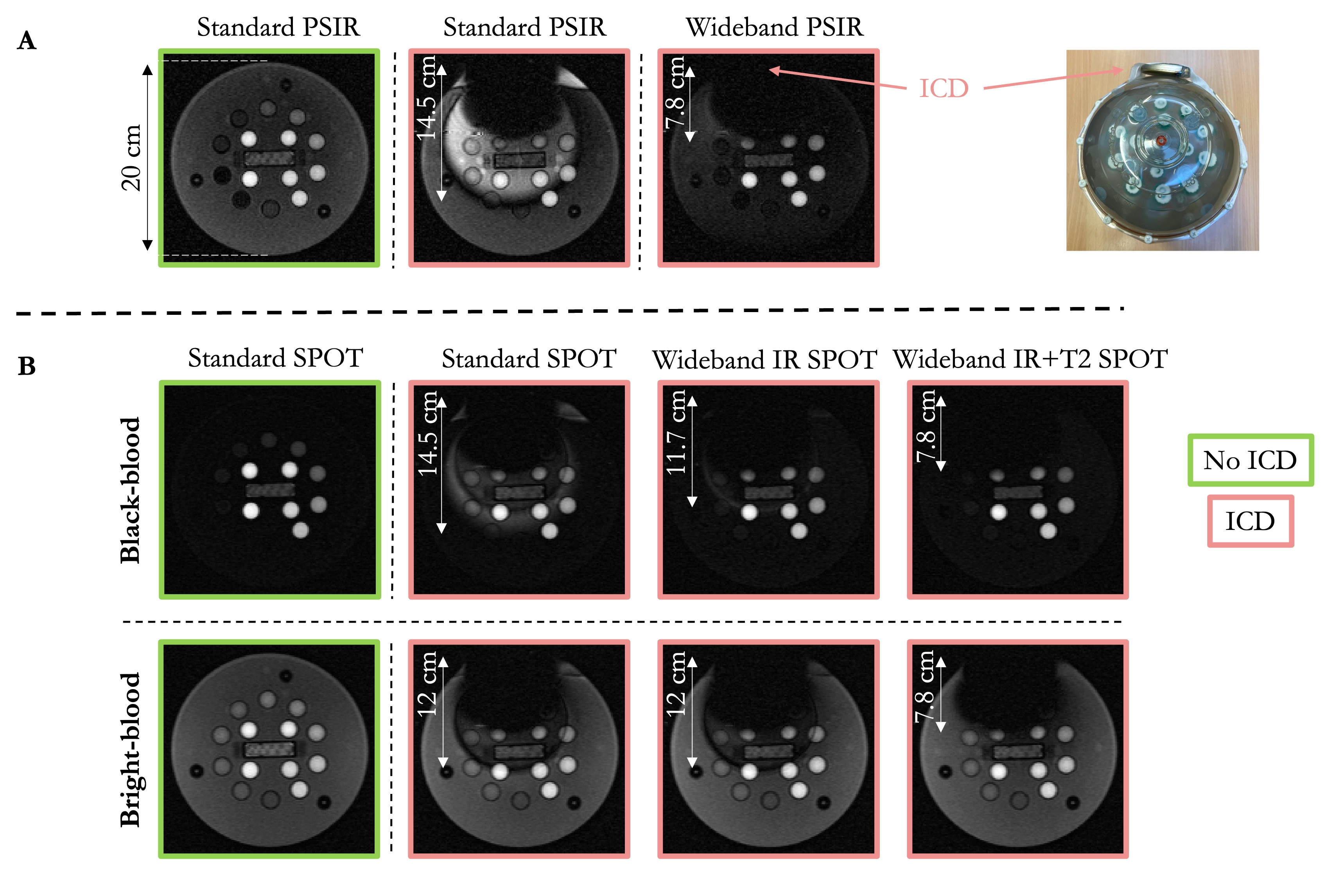
Fig.2. Phantom experiment. The artefact extent is shown with a white arrow. A. PSIR images. 1st column: standard PSIR without CIED; 2nd column: standard PSIR with CIED; 3rd column: wideband PSIR with CIED. B. SPOT images. 1st row: black-blood (BL) images; 2nd row: bright-blood (BR) images. 1st column: standard SPOT without CIED; 2nd column: standard SPOT with CIED; 3rd column: wideband IR SPOT with CIED; 3rd column: wideband IR+T2 SPOT with CIED. Abbreviations: CIED, cardiac implantable electronic device.
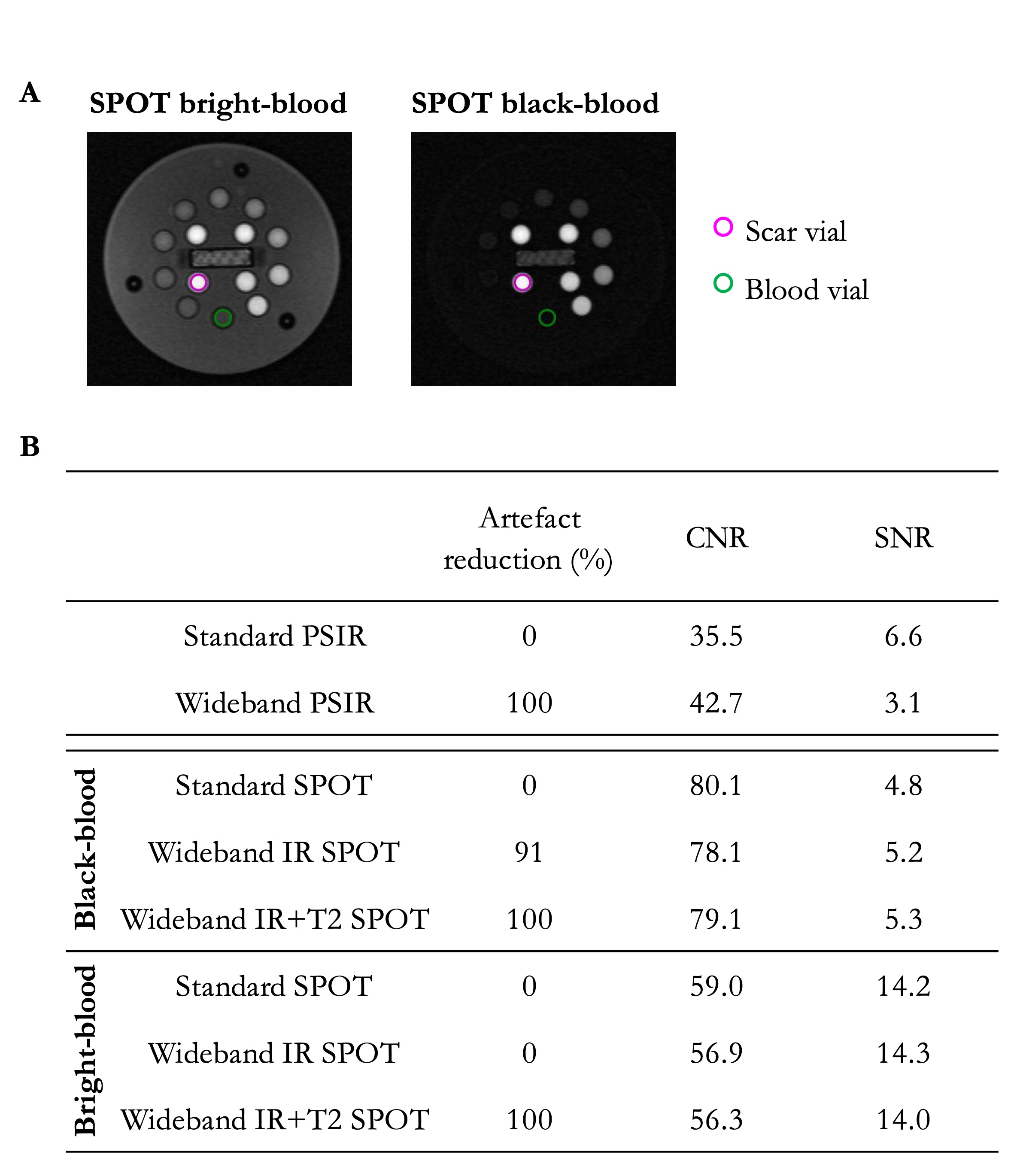
Fig.3. A. Selected tubes for CNR calculation. The green tube represents the signal from healthy myocardium and the pink tube represents the signal from scar tissue. B. Results of the percentage and extent of artefacts, CNR and SNR, in all sequences.
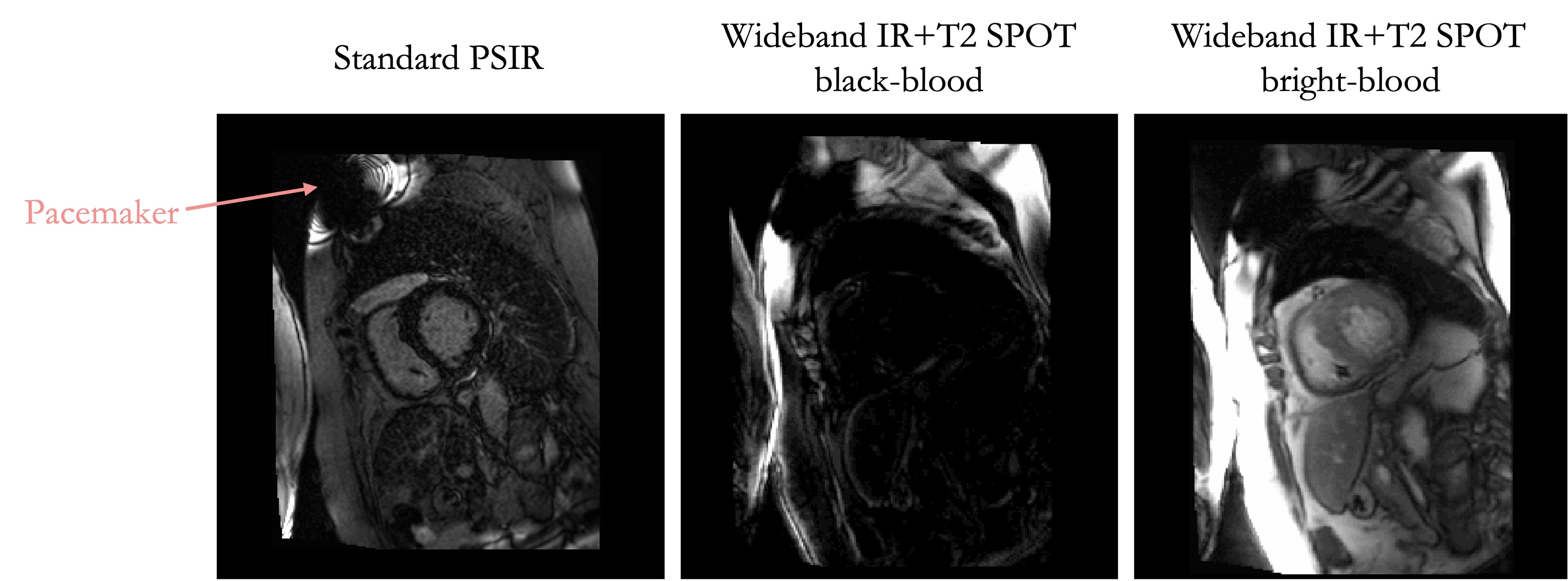
Fig.4. Patient with a pacemaker. Left: standard PSIR; middle: wideband IR+T2 SPOT, black-blood image; right: wideband IR+T2 SPOT, bright-blood image.