4265
Comparison of multiplexed sensitivity encoding and single-shot diffusion-weighted echo-planar imaging of the lung: Preliminary study
Longjiang Fang1, Wenjing Zhao1, Yujing Chu1, Qi Wang1, and Dmytro Pylypenko2
1Department of Radiology, Weifang People's Hospital, Weifang, China, 2GE Healthcare, Beijing, China
1Department of Radiology, Weifang People's Hospital, Weifang, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Lung, Diffusion/other diffusion imaging techniques
This study aims to compare multiplexed sensitivity encoding (MUSE) and single-shot diffusion-weighted echo planar imaging (SS DWEPI) techniques in lung MRI. A total of 22 patients with lung lesions were recruited in the study. Qualitative parameters included anatomic details, suscepti-bility artifacts, and diagnostic confidence; quantitative parameters included SNR and ADC of the lesions. The statistical studies demonstrated results that prove MUSE can provide better anatomic detail, lower susceptibility artifacts, higher diagnostic confidence, and improved SNR of the lung. MUSE is a promising technique for both clinical MRI diagnosis and treatment planning for lung lesions.Introduction
Diffusion-weighted imaging (DWI) is useful for differential diagnosis between lung cancers and benign pulmonary nodules and masses1. Single-shot diffusion-weighted echo-planar imaging (SS DWEPI) is commonly used for lung DWI. Echo planar imaging (EPI) is prone to geometric distortion from susceptibility differences, especially for the lung2. Another disadvantage of single-shot EPI is the relatively low spatial resolution.
Multiplexed sensitivity encoding (MUSE) is one of the best methods for increasing spatial resolution and reducing the occurrence of EPI acquisition distortion artifacts. The MUSE method first uses the conventional SENSE technique to estimate the motion-induced phase variations among multiple EPI segments, and then jointly calculates the magnitude signals of aliased voxels simultaneously from all segments of interleaved EPI. MUSE can achieve high spatial resolution, high SNR, high spatial fidelity, and minimal motion-induced phase errors3.
MUSE has not yet been investigated in the lung. The present study aims to compare performances of MUSE and SS DWEPI techniques in the lung.
Materials and Methods
Subjects
A total of 22 patients (12 males, 10 females, aged 34–80 years, median 64 years) with lung lesions were recruited in this study. All patients underwent chest MRI and CT in 3 days. These patients were diagnosed with adenocarcinoma (n=7), squamous cell carcinoma (n=7), small cell lung cancer (n=1), pneumonia (n=3), lung abscess (n=2), atelectasis (n=1) and solid nodule (n=1).
MRI Imaging
A 3.0-T MR scanner (Signa Architect, GE Healthcare) with a 30-channel AIR coil was used for all subjects. Routine scanning protocol included ZTE, coronal FSE T2WI, transverse PROPELLER with fat suppression T2WI, MUSE, SS-DWEPI and Flex T1WI. DWI was obtained at b values of 0 and 800 s/mm2. All sequences were respiratory-triggered. The scan parameters are presented in Table 1.
Data analysis
Two chest radiologists, with at least 5 years’ experience, independently reviewed all images, while remain-ing blinded to the method of acquisition. Finally, 20 patients were included in the qualitative and quantita-tive analysis, with two patients eliminated because ROIs could not be placed, one with pneumonia and one with small nodules.
Qualitative analysis
The CT images were used as reference to compare ZTE, MUSE and SS DWEPI. ZTE, MUSE and SS DWEPI were scored based on three qualitative image criteria: anatomic detail, susceptibility artifacts and diagnosis confidence. All criteria were scored from 1 (poor) to 5 (excellent).
Quantitative analysis
Apparent diffusion coefficient (ADC) maps were generated using vendor-provided software on GE ADW4.7 workstation. In each patient, ROIs were placed on lesions in ADC maps by two radiologists. SNR of the lesion were calculated as follows: (mean signal intensity of the lesion [SI lesion])/SD lesion4. The mean level of each metric was obtained for further analysis.
Statistical analysis
SPSS 26.0 statistic software was used. The intra-class correlation coefficients analysis was applied to assess the inter-observer agreement of parameter measurement over two radiologists. The Wilcoxon signed-rank (WSR) test was used to compare anatomic detail, susceptibility artifacts, diagnostic confidence, SNR and ADC. P<0.05 was considered statistically significant.
Results
Excellent inter-observer agreement of each parameter measurement was confirmed by high ICC (with r>0.79 for each parameter).
Qualitative results
The anatomic detail of the lung between ZTE and CT had no significant difference (P=0.81). The statistical studies demonstrated better anatomic detail in MUSE than in SS DWEPI (P < 0.05), lower susceptibility artifacts in MUSE than in SS DWEPI (P < 0.05), and higher diagnostic confidence in MUSE than in SS DWEPI (P< 0.05) (Table 2) (Figure 1).
Quantitative results
The ADC values of malignant lesions had significant difference between MUSE and SS DWEPI(P<0.05); the ADC values of benign lesions had no significant difference between MUSE and SS DWEPI(P=0.68). The SNR of the lesions were significantly higher in MUSE than in SS DWEPI (P < 0.05) (Table 3).
Discussion and Conclusions
The results of this study showed, that MUSE can provide better anatomic details, lower susceptibility artifacts, higher diagnostic confidence, and improved SNR of the lung compared to SS DWEPI. ADC val-ues measured using MUSE were significantly lower than those measured using SS-DWEPI for malignant lesions, but not benign lesions.
In conclusion, the image quality of MUSE was superior to that of SS-DWEPI, although there was an increase in acquisition time. MUSE is a promising technique for both clinical diagnostic MRI and for treat-ment planning in lung lesions. Further investigation is required to evaluate the T stage of lung cance, re-sponse of treatment and treatment plan in radiation oncology.
Diffusion-weighted imaging (DWI) is useful for differential diagnosis between lung cancers and benign pulmonary nodules and masses1. Single-shot diffusion-weighted echo-planar imaging (SS DWEPI) is commonly used for lung DWI. Echo planar imaging (EPI) is prone to geometric distortion from susceptibility differences, especially for the lung2. Another disadvantage of single-shot EPI is the relatively low spatial resolution.
Multiplexed sensitivity encoding (MUSE) is one of the best methods for increasing spatial resolution and reducing the occurrence of EPI acquisition distortion artifacts. The MUSE method first uses the conventional SENSE technique to estimate the motion-induced phase variations among multiple EPI segments, and then jointly calculates the magnitude signals of aliased voxels simultaneously from all segments of interleaved EPI. MUSE can achieve high spatial resolution, high SNR, high spatial fidelity, and minimal motion-induced phase errors3.
MUSE has not yet been investigated in the lung. The present study aims to compare performances of MUSE and SS DWEPI techniques in the lung.
Materials and Methods
Subjects
A total of 22 patients (12 males, 10 females, aged 34–80 years, median 64 years) with lung lesions were recruited in this study. All patients underwent chest MRI and CT in 3 days. These patients were diagnosed with adenocarcinoma (n=7), squamous cell carcinoma (n=7), small cell lung cancer (n=1), pneumonia (n=3), lung abscess (n=2), atelectasis (n=1) and solid nodule (n=1).
MRI Imaging
A 3.0-T MR scanner (Signa Architect, GE Healthcare) with a 30-channel AIR coil was used for all subjects. Routine scanning protocol included ZTE, coronal FSE T2WI, transverse PROPELLER with fat suppression T2WI, MUSE, SS-DWEPI and Flex T1WI. DWI was obtained at b values of 0 and 800 s/mm2. All sequences were respiratory-triggered. The scan parameters are presented in Table 1.
Data analysis
Two chest radiologists, with at least 5 years’ experience, independently reviewed all images, while remain-ing blinded to the method of acquisition. Finally, 20 patients were included in the qualitative and quantita-tive analysis, with two patients eliminated because ROIs could not be placed, one with pneumonia and one with small nodules.
Qualitative analysis
The CT images were used as reference to compare ZTE, MUSE and SS DWEPI. ZTE, MUSE and SS DWEPI were scored based on three qualitative image criteria: anatomic detail, susceptibility artifacts and diagnosis confidence. All criteria were scored from 1 (poor) to 5 (excellent).
Quantitative analysis
Apparent diffusion coefficient (ADC) maps were generated using vendor-provided software on GE ADW4.7 workstation. In each patient, ROIs were placed on lesions in ADC maps by two radiologists. SNR of the lesion were calculated as follows: (mean signal intensity of the lesion [SI lesion])/SD lesion4. The mean level of each metric was obtained for further analysis.
Statistical analysis
SPSS 26.0 statistic software was used. The intra-class correlation coefficients analysis was applied to assess the inter-observer agreement of parameter measurement over two radiologists. The Wilcoxon signed-rank (WSR) test was used to compare anatomic detail, susceptibility artifacts, diagnostic confidence, SNR and ADC. P<0.05 was considered statistically significant.
Results
Excellent inter-observer agreement of each parameter measurement was confirmed by high ICC (with r>0.79 for each parameter).
Qualitative results
The anatomic detail of the lung between ZTE and CT had no significant difference (P=0.81). The statistical studies demonstrated better anatomic detail in MUSE than in SS DWEPI (P < 0.05), lower susceptibility artifacts in MUSE than in SS DWEPI (P < 0.05), and higher diagnostic confidence in MUSE than in SS DWEPI (P< 0.05) (Table 2) (Figure 1).
Quantitative results
The ADC values of malignant lesions had significant difference between MUSE and SS DWEPI(P<0.05); the ADC values of benign lesions had no significant difference between MUSE and SS DWEPI(P=0.68). The SNR of the lesions were significantly higher in MUSE than in SS DWEPI (P < 0.05) (Table 3).
Discussion and Conclusions
The results of this study showed, that MUSE can provide better anatomic details, lower susceptibility artifacts, higher diagnostic confidence, and improved SNR of the lung compared to SS DWEPI. ADC val-ues measured using MUSE were significantly lower than those measured using SS-DWEPI for malignant lesions, but not benign lesions.
In conclusion, the image quality of MUSE was superior to that of SS-DWEPI, although there was an increase in acquisition time. MUSE is a promising technique for both clinical diagnostic MRI and for treat-ment planning in lung lesions. Further investigation is required to evaluate the T stage of lung cance, re-sponse of treatment and treatment plan in radiation oncology.
Acknowledgements
No acknowledgement found.References
1. Usuda K, Iwai S, Yamagata A, et al. How to Discriminate Lung Cancer From Benign Pulmonary Nodules and Masses? Usefulness of Diffusion-Weighted Magnetic Resonance Imaging With Ap-parent Diffusion Coefficient and Inside/Wall Apparent Diffusion Coefficient Ratio. Clin Med In-sights Oncol. 2021;15:11795549211014863. Published 2021 Jul 7. doi:10.1177/117955492110148632. Dietrich O, Biffar A, Baur-Melnyk A, Reiser MF. Technical aspects of MR diffusion imaging of the body. Eur J Radiol. 2010;76(3):314-322. doi:10.1016/j.ejrad.2010.02.018
3. Chen NK, Guidon A, Chang HC, Song AW. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage. 2013;72:41-47. doi:10.1016/j.neuroimage.2013.01.038
4. Dietrich O, Raya JG, Reeder SB, Reiser MF, Schoenberg SO. Measurement of signal-to-noise ra-tios in MR images: influence of multichannel coils, parallel imaging, and reconstruction filters. J Magn Reson Imaging. 2007;26(2):375-385. doi:10.1002/jmri.20969
Figures
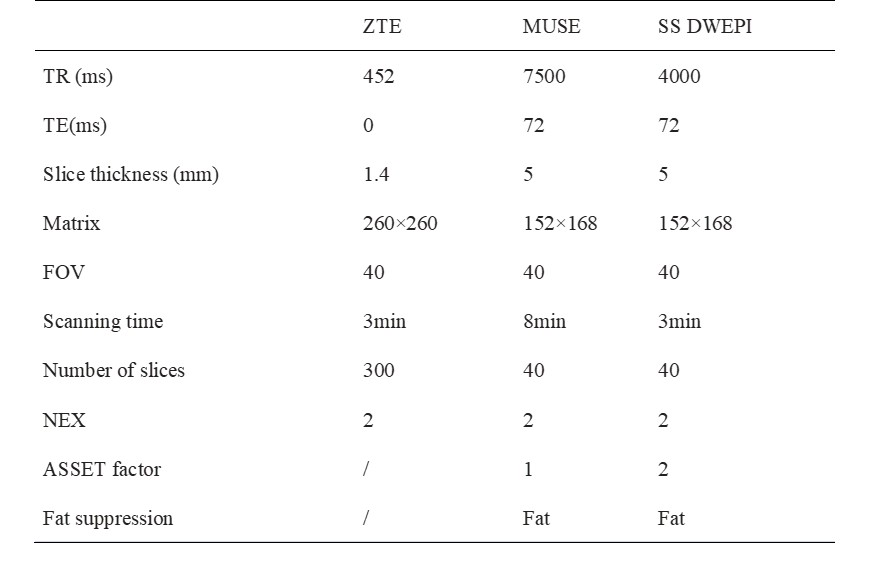
Table 1 Scan parameters
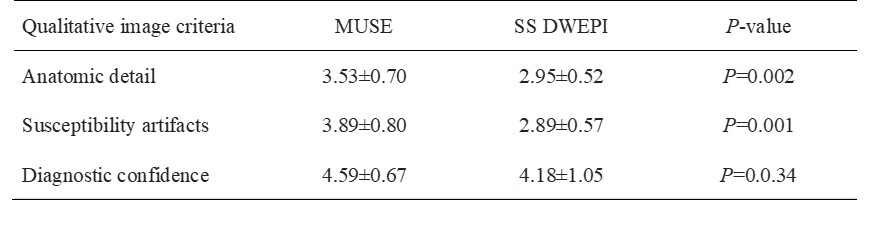
Table 2 Qualitative comparison results
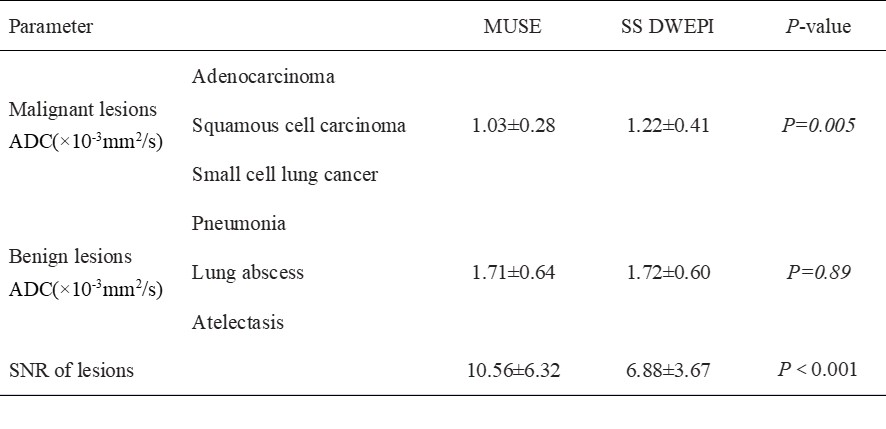
Table 3 Quantitative comparison results

Figure 1: A 52-year-old male, lung adenocarcinoma with atelectasis in the left upper lobe on CT (A) and ZTE-MRI (B), MUSE(C), SS-DWEPI(D) showing complex shape. MUSE can clearly dis-tinguish adenocarcinoma form atelectasis.
DOI: https://doi.org/10.58530/2023/4265