4264
Blood plasma metabolomics study of metastases prostate cancer patients reflects liver alterations involving carbon and nitrogen metabolism
Pradeep Kumar1, Rajeev Kumar2, Sanjay Thulkar3, Sanjay Sharma4, Maroof Ahmad Khan5, and Virendra Kumar1
1NMR and MRI Facility, AIIMS, New Delhi, India, 2Urology, AIIMS, New Delhi, India, 3Radiology , IRCH, AIIMS, New Delhi, India, 4Radiadiagnosis,RPC, AIIMS, New Delhi, India, 5Biostatistics, AIIMS, New Delhi, India
1NMR and MRI Facility, AIIMS, New Delhi, India, 2Urology, AIIMS, New Delhi, India, 3Radiology , IRCH, AIIMS, New Delhi, India, 4Radiadiagnosis,RPC, AIIMS, New Delhi, India, 5Biostatistics, AIIMS, New Delhi, India
Synopsis
Keywords: Prostate, Blood, Metabolomics
Prostate cancer (PCa) with metastases remains incurable diseases requiring early diagnosis and effective treatments. To investigate and integrate the blood plasma metabolomic profiles with clinical parameters to distinguish PCa patients with metastasis from those without bone metastasis using 1H-NMR spectroscopy for establishing potential biomarker/s. Significant changes in liver enzyme ALP, ALT, and AST levels were observed in metastatic PCa. Pathway analysis revealed dysregulation of nitrogen and carbon metabolism. The discovery of metabolites in blood associate with clinical parameters for understanding PCa related pathophysiological mechanisms of bone and liver metastases.Introduction
Metastatic prostate cancer (PCa), remains incurable with a 5-year survival rate of 30%. The most common metastatic sites are bone (84%), distant lymph nodes (10.6%), liver (10.2%), and thorax (9.1%) etc1. PCa patients are more prone to liver and bone metastasis because in these patients elevated levels of liver function tests and these liver enzymes more specific for pathological changes in liver and bones2. Sensitive and specific diagnostic and prognostic tumor biomarker/s for PCa bone metastases will help in clinical management. Thus, the present study is based on 1H-NMR, investigates and integrated for the differences in the metabolic profiling of blood plasma and clinical parameters PCa patients with bone metastases and non-metastases
Method
Total 50 subjects included in this study. Blood samples were collected from bone metastases PCa patients [(n = 20 mean age: 63.5 ±10.0 years; PSA: 134.3 (43.95-1360) ng/mL; GS (7-10)] and PCa patients without metastases [(n =30, mean age: 67 ± 8.3 years; PSA: 14.67 (5.02-111.90) ng/mL); GS (6-9)], in morning pre-prandial after overnight fasting. Liver function tests, liver enzyme (ALP, ALT &AST), proteins and ratio were obtained. Each blood sample was centrifuged at 5000 rpm for 10 minutes at 4°C and plasma was separated and stored at -80°C until NMR experiments were carried out. Proton spectra of blood plasma samples were carried out at 700 MHz spectrometer (Agilent, USA) using 1D CPMG with pre-saturation. The following parameters were used for 1D NMR experiment: 64 scans with a 70s relaxation delay and a spectral width of 9124.1 Hz with an echo time of 15ms. 2D TOCSY and COSY experiment were carried out for assignments of metabolite peaks. Metabolites levels were compared in two groups using unpaired Man Whitney U test. A p-value <0.05 was considered significant. Univariate (ROC) curve analysis and multivariate (OPLS-DA and VIP) score statistical and pathway analysis were carried out using MetaboAnalyst 5.0.
Result
Figure 1 shows the representative 1D-CPMG 1H spectrum of blood plasma sample of a PCa patient with metastases (A) and from patient without metastases (B). In all, 24 metabolites were assigned using 1D and 2D NMR. NMR based metabolomics profile analysis. VIP score and AUC are shown in Figure1. Significantly higher concentration 3HOB, lactate, alanine, acetate, acetoacetate, glutamate, pyruvate, glutamine, DMA, creatine, phosphocreatine, choline, GPC, glycine, creatinine, glucose and betaine was found in metastases PCa as compared to non-metastases patients (Table 1). Furthermore analysis, statistically significant difference between alanine transaminase (ALT) and aspartate transaminase (AST), alkaline phosphatase (ALP) in patients (Table 2). Heatmap correction (liver enzyme, proteins ratio) and Box & whisker plots (ALT, AST and ALP) presentation are shown in Figure2. Pathway enrichment analysis using the KEGG and SMPDB revealed potential involvement of nitrogen and carbon metabolism in PCa (Figure3).
Discussion
The present study revealed significantly higher concentration of Alanine, pyruvate, glutamine and glutamate in blood plasma of PCa patients with metastases as compared to non-metastases. Accordingly, enzyme ALT, AST and ALP higher levels were directly correlated to disease severity and prognosis1. An increase in AST levels may indicate liver damage, disease or muscle damage. Both alanine and aspartate aminotransferases catalyze the conversion of alpha-ketoglutarate and amino acid to glutamate and another product. In the case of ALT, the amino acid and product are alanine and pyruvate2. In the case of AST, the amino acid and product are aspartate and oxaloacetate and both are involved in TCA and urea cycle of the hepatic cells. Altered ALT and AST enzymes may change the carbon and nitrogen metabolism3. ALP is an enzyme found in the liver and bone and is important for breaking down proteins4. Thus, ALP may be an indicator of bone metastatic tumor load5. A higher level of ketone body acetoacetate, acetate and 3HOB were seen in bone metastases PCa patients. These are produced by liver from fatty acids oxidation and converted into acetyl CoA, which then enters the TCA cycle. Higher level of acetate may be reflecting increased utilization of lipid demands to meet the energy requirements for cell growth and proliferation in metastatic cancer cells6. A significantly increased concentration of membrane metabolite choline, GPC, betaine and DMA in bone PCa patients with metastases indicating a higher proliferation of metastatic PCa cells. Furthermore, alteration of glucose metabolism (glucose and lactate) energy metabolism (creatine, phosphocreatine, creatinine), and nucleic acid metabolism (glycine) were observed in bone metastases with PCa patients7. These metabolic reprogramming of the amino acids, glycolysis, Krebs cycle and interconnected with fatty acids, ketone body and nucleic acid metabolism. Altered nitrogen and carbon metabolism were found from our data being present between the top-enriched pathways in patients.
Conclusion
This preliminary study demonstrated that NMR based integrated metabolomics with clinical parameters may be useful for distinguishing metastases PCa patients and non- metastases patients. Further our results provided a better understanding of the metabolic pathway alterations through changes in amino acids, ketone bodies, phospholipids, and energy metabolites with may be associated cell growth and progression to lethal conditions of the patients. The variations found in the blood plasma metabolomic may reflect a more complex systemic perturbation induced by bone metastases, which might affect carbon and nitrogen metabolism in liver.
Metastatic prostate cancer (PCa), remains incurable with a 5-year survival rate of 30%. The most common metastatic sites are bone (84%), distant lymph nodes (10.6%), liver (10.2%), and thorax (9.1%) etc1. PCa patients are more prone to liver and bone metastasis because in these patients elevated levels of liver function tests and these liver enzymes more specific for pathological changes in liver and bones2. Sensitive and specific diagnostic and prognostic tumor biomarker/s for PCa bone metastases will help in clinical management. Thus, the present study is based on 1H-NMR, investigates and integrated for the differences in the metabolic profiling of blood plasma and clinical parameters PCa patients with bone metastases and non-metastases
Method
Total 50 subjects included in this study. Blood samples were collected from bone metastases PCa patients [(n = 20 mean age: 63.5 ±10.0 years; PSA: 134.3 (43.95-1360) ng/mL; GS (7-10)] and PCa patients without metastases [(n =30, mean age: 67 ± 8.3 years; PSA: 14.67 (5.02-111.90) ng/mL); GS (6-9)], in morning pre-prandial after overnight fasting. Liver function tests, liver enzyme (ALP, ALT &AST), proteins and ratio were obtained. Each blood sample was centrifuged at 5000 rpm for 10 minutes at 4°C and plasma was separated and stored at -80°C until NMR experiments were carried out. Proton spectra of blood plasma samples were carried out at 700 MHz spectrometer (Agilent, USA) using 1D CPMG with pre-saturation. The following parameters were used for 1D NMR experiment: 64 scans with a 70s relaxation delay and a spectral width of 9124.1 Hz with an echo time of 15ms. 2D TOCSY and COSY experiment were carried out for assignments of metabolite peaks. Metabolites levels were compared in two groups using unpaired Man Whitney U test. A p-value <0.05 was considered significant. Univariate (ROC) curve analysis and multivariate (OPLS-DA and VIP) score statistical and pathway analysis were carried out using MetaboAnalyst 5.0.
Result
Figure 1 shows the representative 1D-CPMG 1H spectrum of blood plasma sample of a PCa patient with metastases (A) and from patient without metastases (B). In all, 24 metabolites were assigned using 1D and 2D NMR. NMR based metabolomics profile analysis. VIP score and AUC are shown in Figure1. Significantly higher concentration 3HOB, lactate, alanine, acetate, acetoacetate, glutamate, pyruvate, glutamine, DMA, creatine, phosphocreatine, choline, GPC, glycine, creatinine, glucose and betaine was found in metastases PCa as compared to non-metastases patients (Table 1). Furthermore analysis, statistically significant difference between alanine transaminase (ALT) and aspartate transaminase (AST), alkaline phosphatase (ALP) in patients (Table 2). Heatmap correction (liver enzyme, proteins ratio) and Box & whisker plots (ALT, AST and ALP) presentation are shown in Figure2. Pathway enrichment analysis using the KEGG and SMPDB revealed potential involvement of nitrogen and carbon metabolism in PCa (Figure3).
Discussion
The present study revealed significantly higher concentration of Alanine, pyruvate, glutamine and glutamate in blood plasma of PCa patients with metastases as compared to non-metastases. Accordingly, enzyme ALT, AST and ALP higher levels were directly correlated to disease severity and prognosis1. An increase in AST levels may indicate liver damage, disease or muscle damage. Both alanine and aspartate aminotransferases catalyze the conversion of alpha-ketoglutarate and amino acid to glutamate and another product. In the case of ALT, the amino acid and product are alanine and pyruvate2. In the case of AST, the amino acid and product are aspartate and oxaloacetate and both are involved in TCA and urea cycle of the hepatic cells. Altered ALT and AST enzymes may change the carbon and nitrogen metabolism3. ALP is an enzyme found in the liver and bone and is important for breaking down proteins4. Thus, ALP may be an indicator of bone metastatic tumor load5. A higher level of ketone body acetoacetate, acetate and 3HOB were seen in bone metastases PCa patients. These are produced by liver from fatty acids oxidation and converted into acetyl CoA, which then enters the TCA cycle. Higher level of acetate may be reflecting increased utilization of lipid demands to meet the energy requirements for cell growth and proliferation in metastatic cancer cells6. A significantly increased concentration of membrane metabolite choline, GPC, betaine and DMA in bone PCa patients with metastases indicating a higher proliferation of metastatic PCa cells. Furthermore, alteration of glucose metabolism (glucose and lactate) energy metabolism (creatine, phosphocreatine, creatinine), and nucleic acid metabolism (glycine) were observed in bone metastases with PCa patients7. These metabolic reprogramming of the amino acids, glycolysis, Krebs cycle and interconnected with fatty acids, ketone body and nucleic acid metabolism. Altered nitrogen and carbon metabolism were found from our data being present between the top-enriched pathways in patients.
Conclusion
This preliminary study demonstrated that NMR based integrated metabolomics with clinical parameters may be useful for distinguishing metastases PCa patients and non- metastases patients. Further our results provided a better understanding of the metabolic pathway alterations through changes in amino acids, ketone bodies, phospholipids, and energy metabolites with may be associated cell growth and progression to lethal conditions of the patients. The variations found in the blood plasma metabolomic may reflect a more complex systemic perturbation induced by bone metastases, which might affect carbon and nitrogen metabolism in liver.
Acknowledgements
ICMR-RA for the Fellowship (Code No. 2020-8295)References
1. Gandaglia G, Abdollah F, Schiffmann J et al. Prostate. 2014;74(2):210-216.
2. Huang XJ, Choi YK, Im HS et al.Sensors (Basel). 200, 31;6(7):756–82.
3. McGill MR. EXCLI J. 2016, 15; 15:817-828.
4. Moussa M, Chakra MA. J Surg Case Rep. 2019 10;2019(10):rjz291.
5. Lorente JA, Morote J, Raventos C et al. J Urol. 1996;155(4):1348-1351.
6. Salciccia S, Capriotti AL, Laganà A, et al . Int J Mol Sci. 2021;22(9):4367.
7. Giskeødegård GF, Hansen AF Bertilsson H et al. Bri J Cancer. 2015; 113(12):1712–1719.
Figures
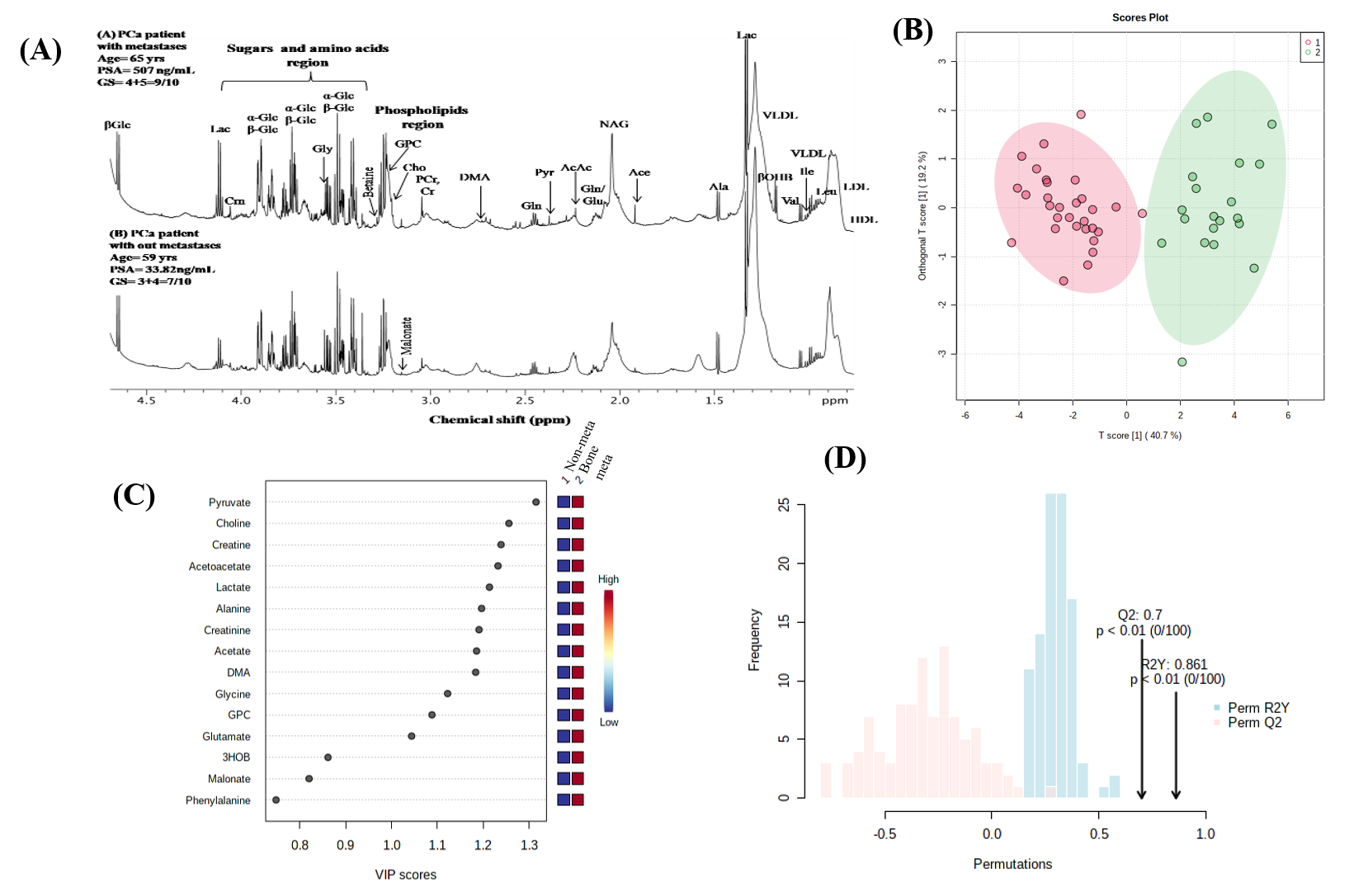
Figure1: Representative one
dimensional (1D) aliphatic region of 1H NMR (700MHz) spectrum of
blood plasma of PCa patients with bone metastases (upper) from non- metastases (lower) (A), OPLS- DA score plot showing discrimination
of bone metastases patients (red) from non-metastases patients (green) in blood
plasma (B), VIP scores for 15 blood born
metabolites with highest contribution of to the separation of the present study
groups (C) and permutation test for
validate model (D).
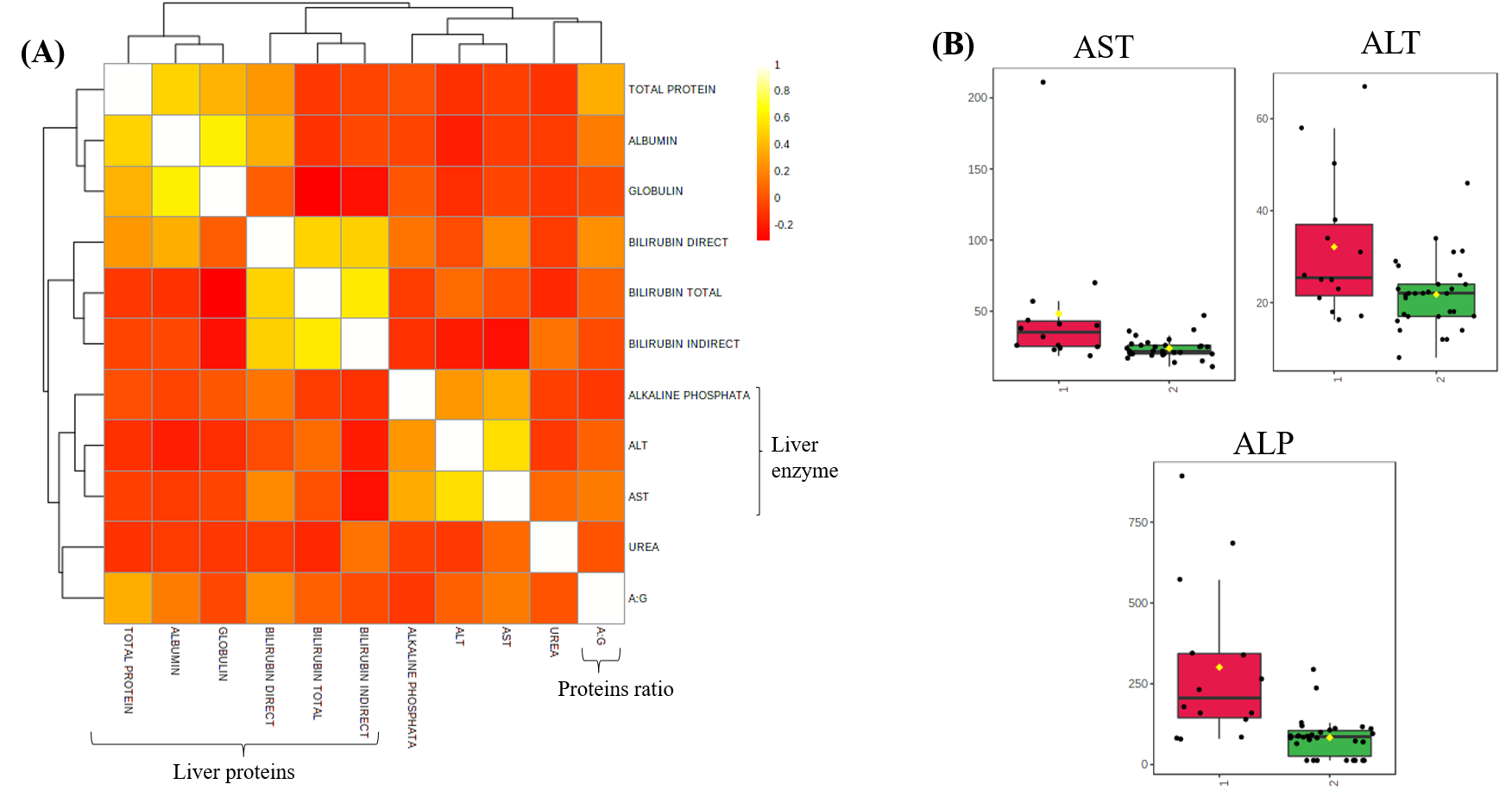
Figure2: Heat map
of correlation between liver enzyme, protein and their ratio (A), Box and
Whisker plot of enzyme AST ALT and ALP of bone metastasis with PCa patients as compare
to non-metastasis (B).
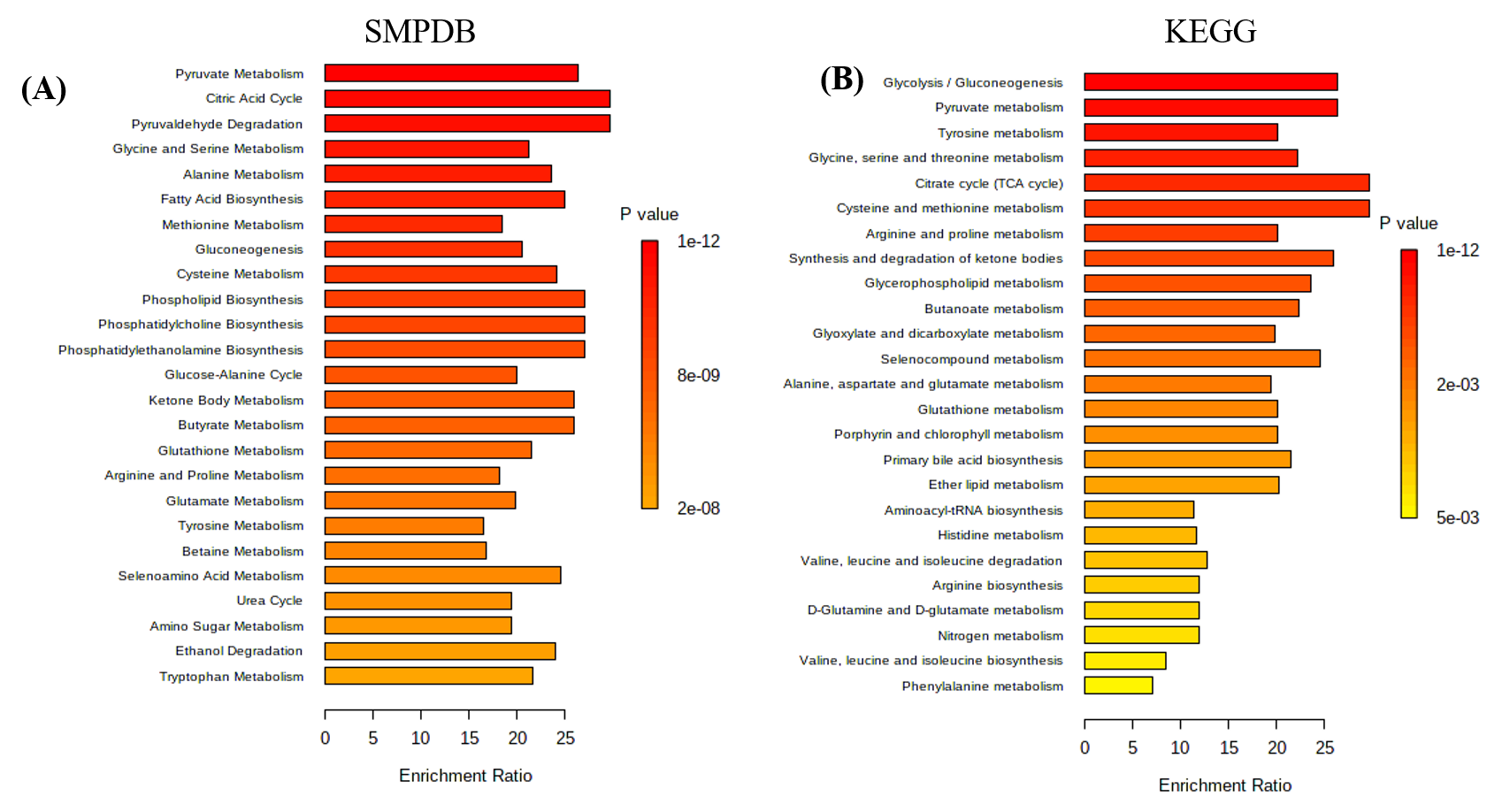
Figure3: Metabolic Set Enrichment Analysis (MSEA) showing
altered significant metabolites revealed in bone metastases PCa patients using SMPDB
and KEGG.
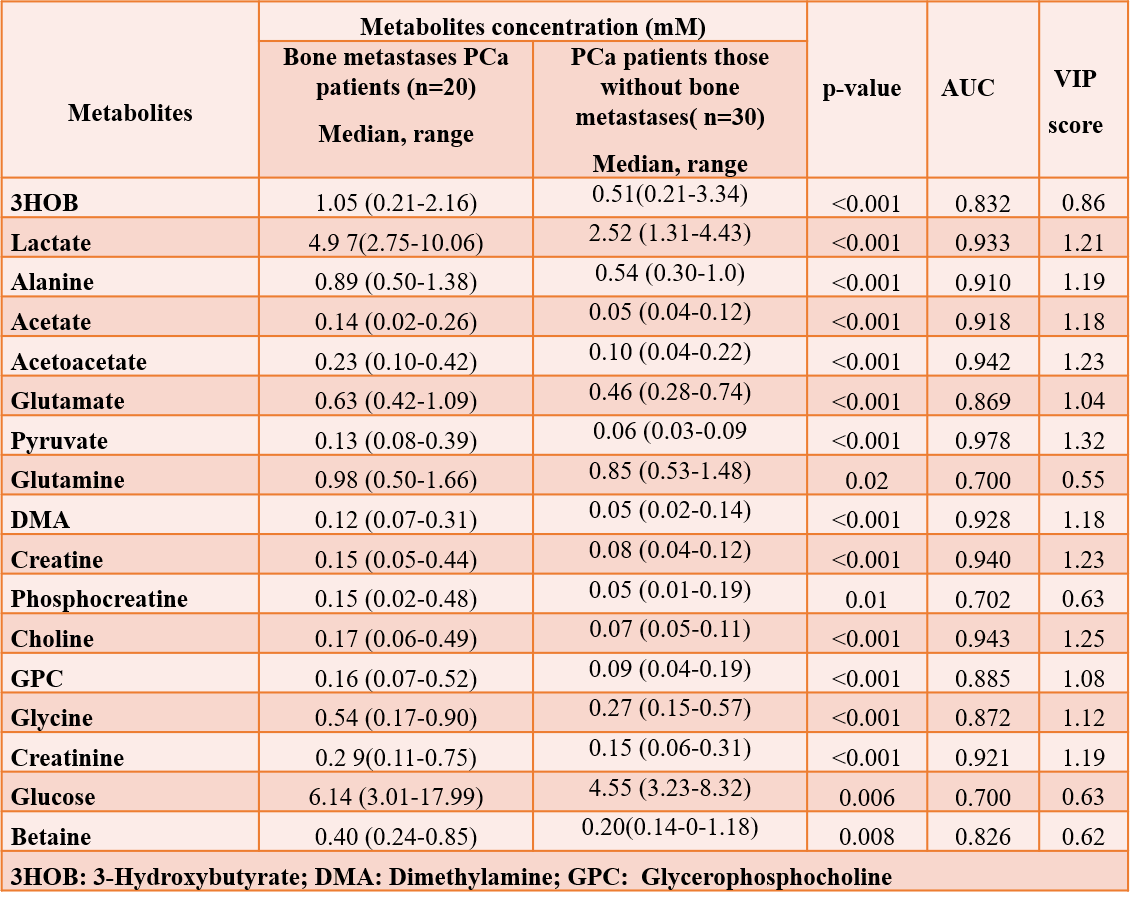
Table1: Concentration of
metabolites (mM) in blood plasma sample of bone metastasis with PCa patients compared to non-metastases condition.
AUC values were obtained from ROC curve analyses and VIP scores from PLS-DA.
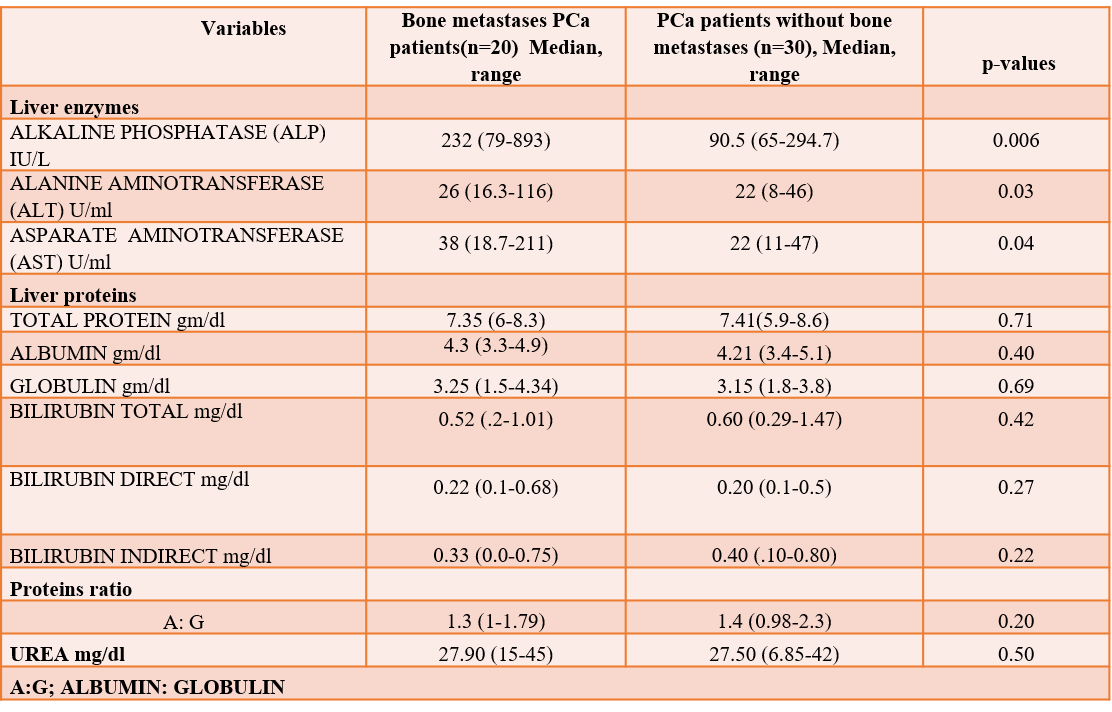
Table2: Summary of enzymes, proteins, and their ratio patterns
in liver of bone metastases with PCa patients as compared to non-metastases
patients.
DOI: https://doi.org/10.58530/2023/4264