4202
Deep Learning Denoising Reconstruction Enables up to 2X Scan Time Reduction while Maintaining Image Quality for Musculoskeletal Imaging
Hung Phi Do1, Dawn Berkeley1, Brian Tymkiw1, Wissam AlGhuraibawi1, and Mo Kadbi1
1Canon Medical Systems USA, Inc., Tustin, CA, United States
1Canon Medical Systems USA, Inc., Tustin, CA, United States
Synopsis
Keywords: MSK, MSK
Two-average (2NAQ) scans are often required to acquire high resolution images with adequate Signal-to-Noise Ratio (SNR). Deep Learning Denoising Reconstruction (DLR) effectively removes noise hence improving the SNR of reconstructed images. The SNR gain could be used to increase resolution and/or reduce scan time. This study demonstrates that the DLR-reconstructed one-average (1NAQ) images have similar image quality to those acquired with 2NAQ and reconstructed with conventional reconstruction. As a result, approximately 2X scan time reduction is achieved with DLR.Introduction
Deep Learning Denoising Reconstruction (DLR) can efficiently remove noise hence improving the Signal-to-Noise Ratio (SNR) of MRI images. The SNR gain can be used to increase spatial resolution and/or shorten the scan time. In practice, two signal averages are often utilized to acquire high-resolution images with adequate SNR. This study demonstrates the feasibility of using DLR to shorten musculoskeletal (MSK) scan time by allowing the acquisition of high-resolution images with one average.Methods
Healthy volunteers’ knees, ankles, and shoulders were scanned using a 3T MRI scanner. Shorten protocols of five sequences with one average (1NAQ) were scanned and compared with those acquired with 2NAQ protocols. The 2NAQ acquisitions were reconstructed with conventional reconstruction while the 1NAQ reconstructions were reconstructed with DLR (an FDA 510(k)-cleared Deep Learning Denoising Reconstruction).To evaluate how well DLR removes noise, the 1NAQ acquisitions were also reconstructed with conventional reconstruction (i.e., without DLR) and compared with those reconstructed with DLR by performing image subtraction. The apparent SNR of bone marrow and muscle, as well as the Contrast-to-Noise Ratio (CNR) of bone marrow to muscle, were measured and compared for the knee data. Sequence parameters of the 1NAQ and 2NAQ protocols are shown in Figure 1.
Results
Figures 2, 3, and 4 show resulting images on a knee, an ankle, and a shoulder using the 1NAQ and 2NAQ protocols shown in Figure 1. Images acquired with a 1NAQ protocol reconstructed with DLR (top row) and those acquired with 2NAQ protocol reconstructed with conventional reconstruction. While 2NAQ images were acquired with ~2X longer scan time, they have similar image quality as those acquired with 1NAQ reconstructed with DLR.Apparent SNR and CNR measurements from a knee scan are shown in Figure 2 (bottom table). Compared to images acquired using the 1NAQ protocol without DLR, DLR increased SNR by 40% and 54% in bone marrow and muscle, respectively. Compared to 2NAQ images, DLR has enabled 11% and 7% higher SNR in bone marrow and muscle, respectively. For 1NAQ images, DLR increases CNR by 59% compared to those reconstructed without DLR and has a similar CNR to those acquired with the 2NAQ protocol.
Figure 5 shows how DLR effectively removes noise while maintaining anatomical details by subtracting images reconstructed without DLR (middle row) from those reconstructed with DLR (top row). The resulting subtraction images only contain noise. Similar observations were seen with the subtraction images of knee and ankle scans.
Discussion and Conclusion
The preliminary results from this study demonstrate that DLR may shorten the scan time up to 2X by acquiring data with one average (1NAQ) while maintaining similar image quality with those acquired with two averages (2NAQ). High SNR and resolution images in shorter scan time would allow more comfort and accessible MRI.Acknowledgements
No acknowledgement found.References
No reference found.Figures
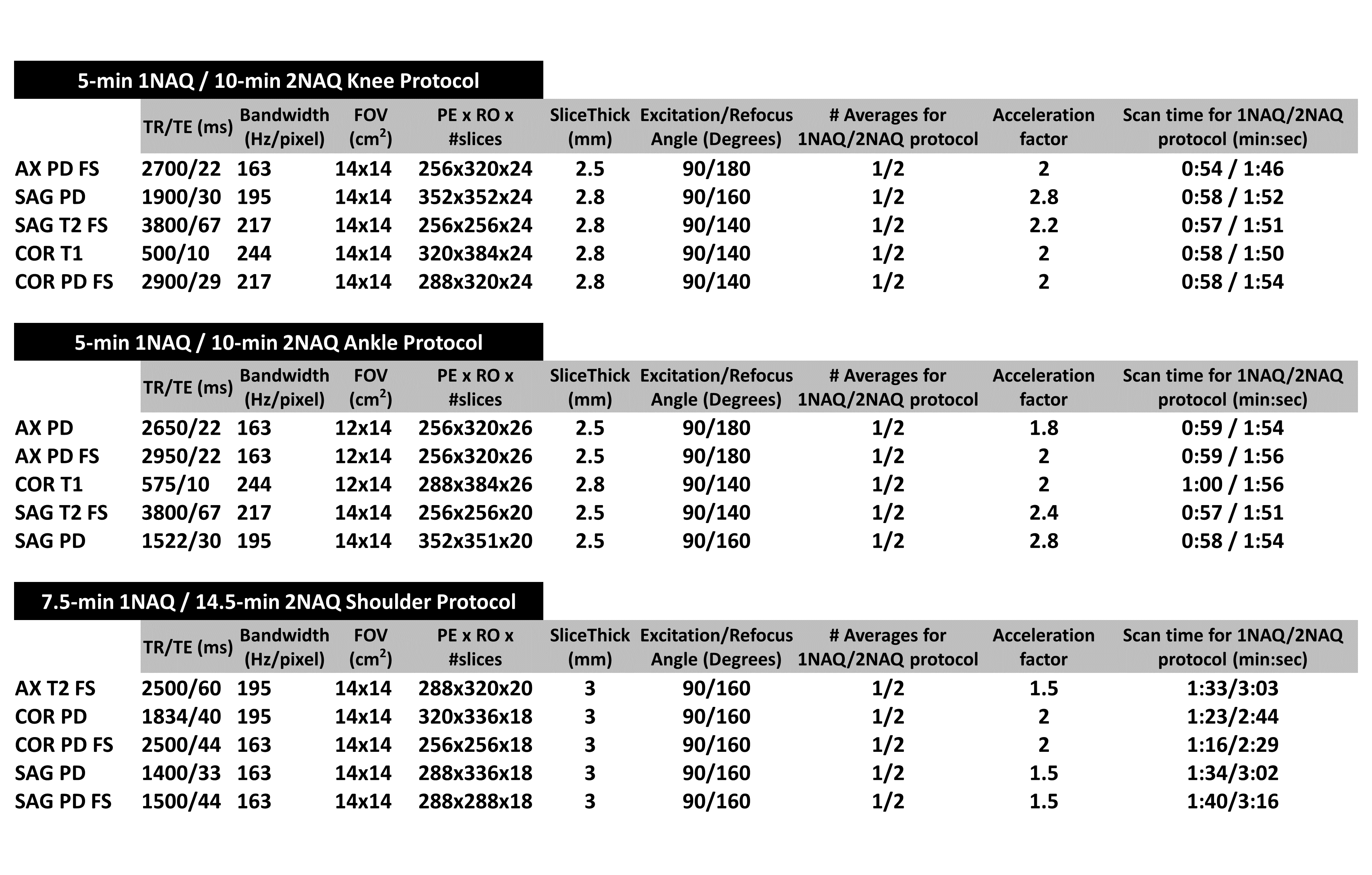
Figure 1: Sequence parameters of the one-average (1NAQ)
and two-average (2NAQ) protocols of the knee, ankle, and shoulder. The 1NAQ
protocol has approximately 2X shorter scan time than the 2NAQ one.
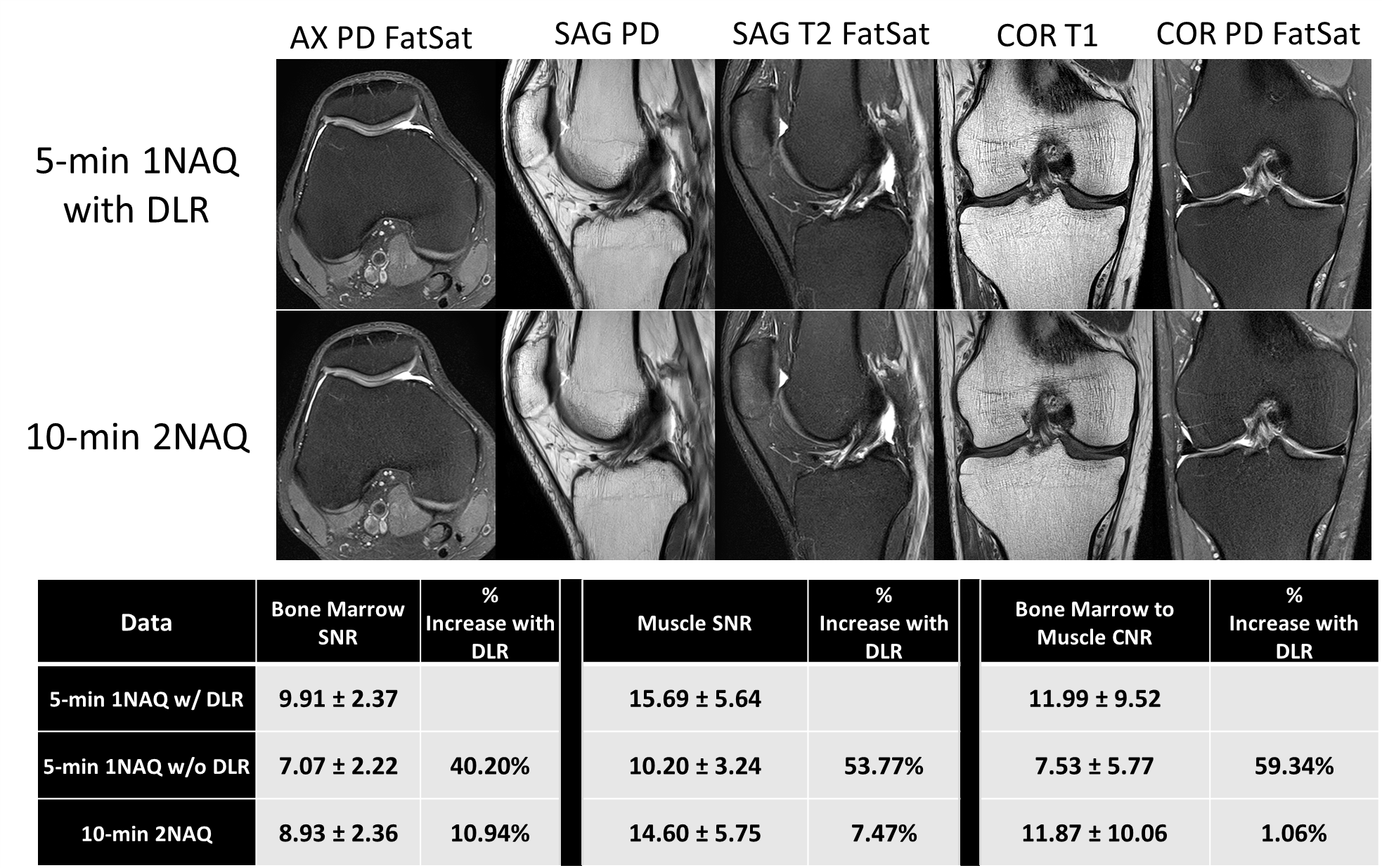
Figure 2: Knee images acquired using a 5-min 1NAQ protocol
(~1 min per sequence) reconstructed with DLR (top row) and those acquired using
a 10-min 2NAQ protocol (bottom row). The associated table shows SNR and CNR increases
with DLR compared to images without DLR and to images acquired with 2NAQ (i.e.,
~2X longer scan time). SNR and CNR are reported as mean ± standard deviation across five
contrasts.
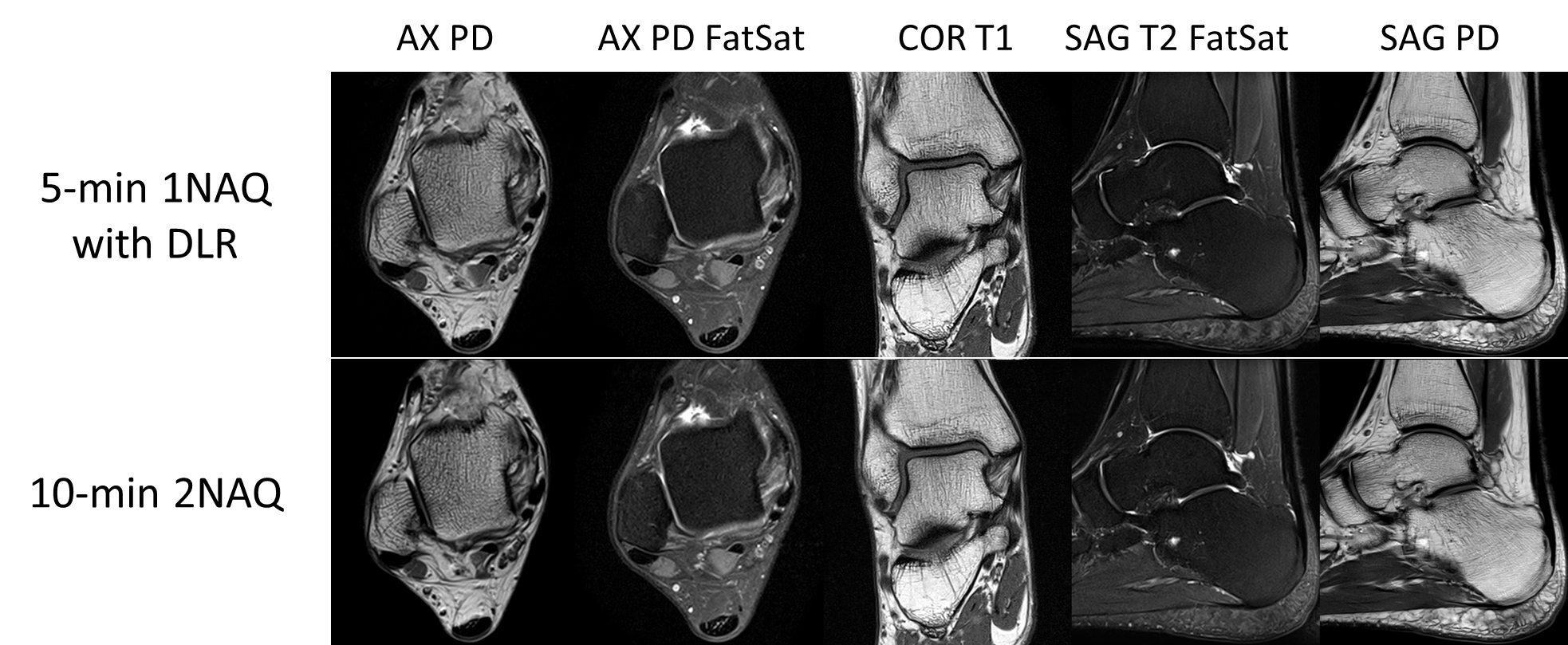
Figure 3: Ankle images acquired using a 5-min 1NAQ protocol
(~1 min per sequence) reconstructed with DLR (top row) and those acquired using
a 10-min 2NAQ protocol (bottom row). The 2NAQ protocol is ~2X longer than the
1NAQ one.
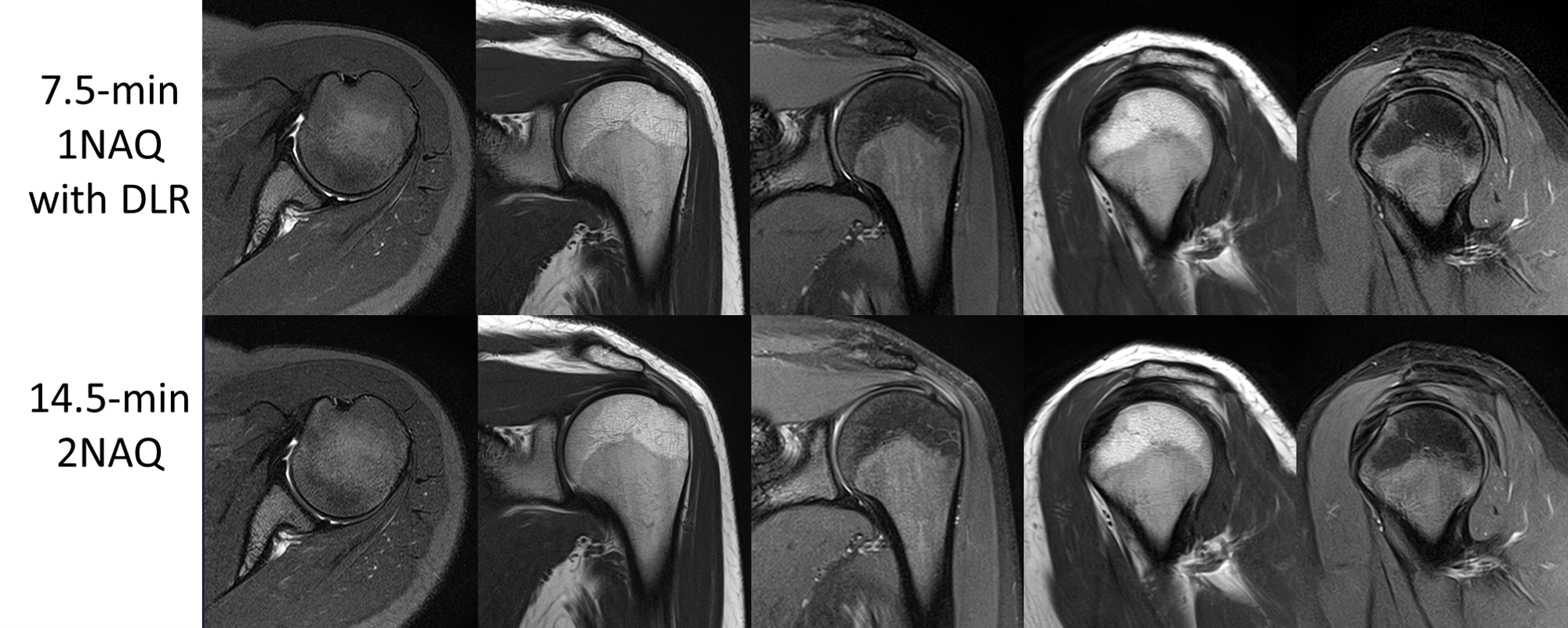
Figure 4: Shoulder images acquired using a 7.5-min
1NAQ protocol (~1.5 min per sequence) reconstructed with DLR (top row) and
those acquired using a 14.5-min 2NAQ protocol (bottom row). The 2NAQ protocol
is ~2X longer than the 1NAQ one.
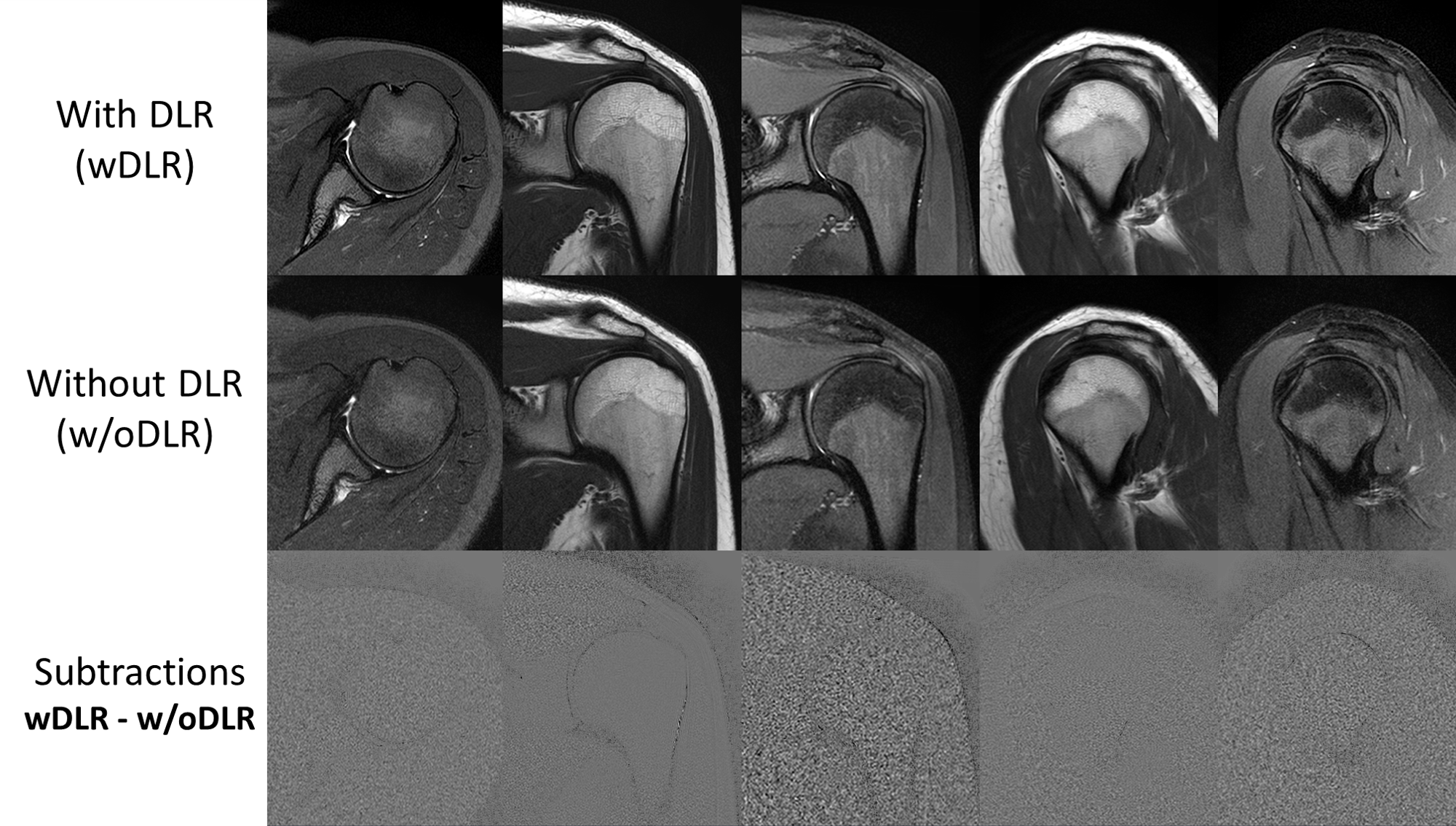
Figure 5: Shoulder images acquired using a 7.5-min
1NAQ protocol reconstructed with DLR (top row) and without DLR (middle row). The
subtractions (with DLR minus without DLR) demonstrate how DLR effectively
removes noise while maintaining anatomical details.
DOI: https://doi.org/10.58530/2023/4202