4200
Increased Resolution and Shortened Scan Time of T2 weighted Prostate MRI using Deep Learning Denoising Reconstruction at 1.5T
Hung Phi Do1, Dawn Berkeley1, Brian Tymkiw1, Wissam AlGhuraibawi1, and Mo Kadbi1
1Canon Medical Systems USA, Inc., Tustin, CA, United States
1Canon Medical Systems USA, Inc., Tustin, CA, United States
Synopsis
Keywords: Prostate, Prostate
In prostate MRI, high SNR images are desired for a better depiction of anatomical and pathological structures; however, it often requires a longer scan time, especially at 1.5T. Deep Learning Denoising Reconstruction (DLR) has been shown to effectively remove noise, allowing high SNR with higher resolution and shortened scan time simultaneously. This study demonstrates that DLR enables the acquisition of high SNR images with 29.48% scan time reduction and 31.51% increase in spatial resolution at 1.5T.Introduction
Clinical images with high resolution and high signal-to-noise ratio (SNR) are desired in prostate MRI for better delineation of anatomical and pathological structures. Prostate MRI at 1.5 T and 3T has been well established, however, the PI-RADS Committee prefers the use of 3T because of its SNR benefits [1]. To compensate for the lower SNR at1.5T, imaging protocols are often longer and acquired with lower resolution compared to 3T protocols. Conventionally, increasing resolution often results in an unavoidable tradeoff of lengthened scan time and lower SNR. Deep Learning Denoising Reconstruction (DLR) has been shown to effectively remove noise, hence, improving SNR. SNR gain from DLR could be used to increase resolution and/or reduce scan time. The goal of this study is to optimize 1.5T T2 weighted sequences to achieve higher resolution in a shorter scan time using DLR.Methods
In this study, seven subjects were scanned using a 1.5T scanner. Prostate routine clinical sequences of SAG T2, AX T2, and COR T2 were acquired with two averages (2NAQ). The DLR-optimized protocol contained the same three sequences but with one average (1NAQ) and a larger matrix size. Sequence parameters are shown in Figure 1. The routine protocol was reconstructed using the conventional reconstruction filter and the DLR-optimized protocol was reconstructed using an FDA 510(k)-cleared Deep Learning Denoising Reconstruction (DLR).To demonstrate how well DLR removes noise and improves image quality, the DLR-optimized protocol was additionally reconstructed using conventional reconstruction and compared with those reconstructed with DLR. Regions of interest (ROIs) were drawn on a homogeneous region on the prostate. The mean and standard deviation (SD) of signal intensities within each ROI were recorded for apparent SNR and CNR calculations. Because of the lack of noise-only region within the scanned images, apparent SNR was calculated as mean signal intensity divided by SD within each ROI.
Results
Figure 1 shows the sequence parameters of the routine (two averages) protocol and the DLR-optimized (one average for shorter scan time and at a higher resolution) protocol. Additionally, the percentage of resolution improvement and scan time reduction are shown for each sequence. On average, scan time is shortened by 29.48% and spatial resolution is increased by 31.51% for the three T2-weighted sequences.As shown in Figure 2 DLR-optimized images (bottom row) are sharper and have better delineations of anatomical details compared to routine images (top row) likely because of the increased resolution in DLR acquisitions. The anatomical structures of the two acquisitions are slightly different due to inter-scan motions. Despite higher resolution and shorter scan time, DLR images (bottom) have similar SNR compared to routine images (top).
Figure 3 shows images acquired using the DLR-optimized protocol while reconstructed using the conventional reconstruction method (top row) and DLR (bottom row). For all the scanned sequences SAG T2, AX T2, and COR T2, DLR enabled SNR to increase by 27.57%, 19.71%, and 27.13%, respectively.
Discussion
As shown in Figure 2, the higher-resolution images acquired using the DLR-optimized protocol improve the depiction of anatomical structures compared to routine images. Despite ~32% higher resolution and ~29% shorter scan time, DLR images (bottom) have similar SNR compared to routine images.Figure 3 demonstrates DLR’s effectiveness in removing noise from the DLR-optimized protocol. DLR-reconstructed images (bottom row) demonstrate higher SNR, higher image quality, and better delineation of anatomical structures in comparison to those reconstructed using the conventional reconstruction method (top row). In this subject, DLR improves SNR by an average of 23.64 ± 5.56 % compared to images reconstructed using the conventional method.
Conclusion
The PI-RADS Steering Committee prefers the use of 3T for prostate MRI due to its higher SNR [1]. In practice, however, prostate programs at both 3T and 1.5T are well established. For the 1.5T program, lower resolution and longer scan time are recommended to compensate for the lower SNR. This study demonstrates that DLR can allow the acquisition of T2-weighted prostate images with higher resolution and shorter scan time compared to those routinely acquired at 1.5T.Acknowledgements
No acknowledgement found.References
[1] Barrett, Tristan, et al. "PI-RADS version 2.1: one small step for prostate MRI." Clinical radiology 74.11 (2019): 841-852.Figures
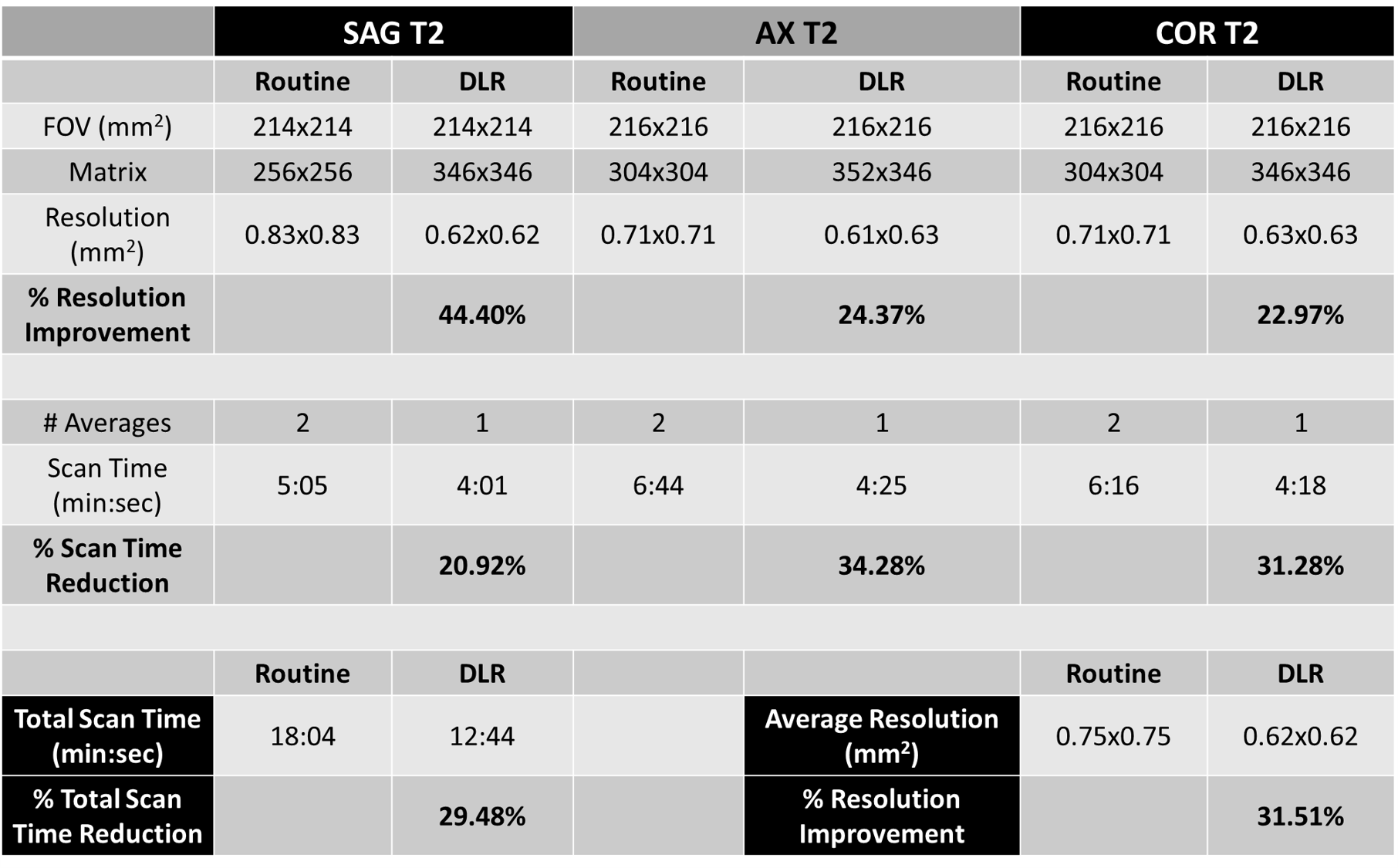
Figure 1: Sequence parameters of routine and DLR-optimized protocols. DLR
enabled scan time reduction by 29.48% with an average improvement in spatial
resolution of 31.51%.
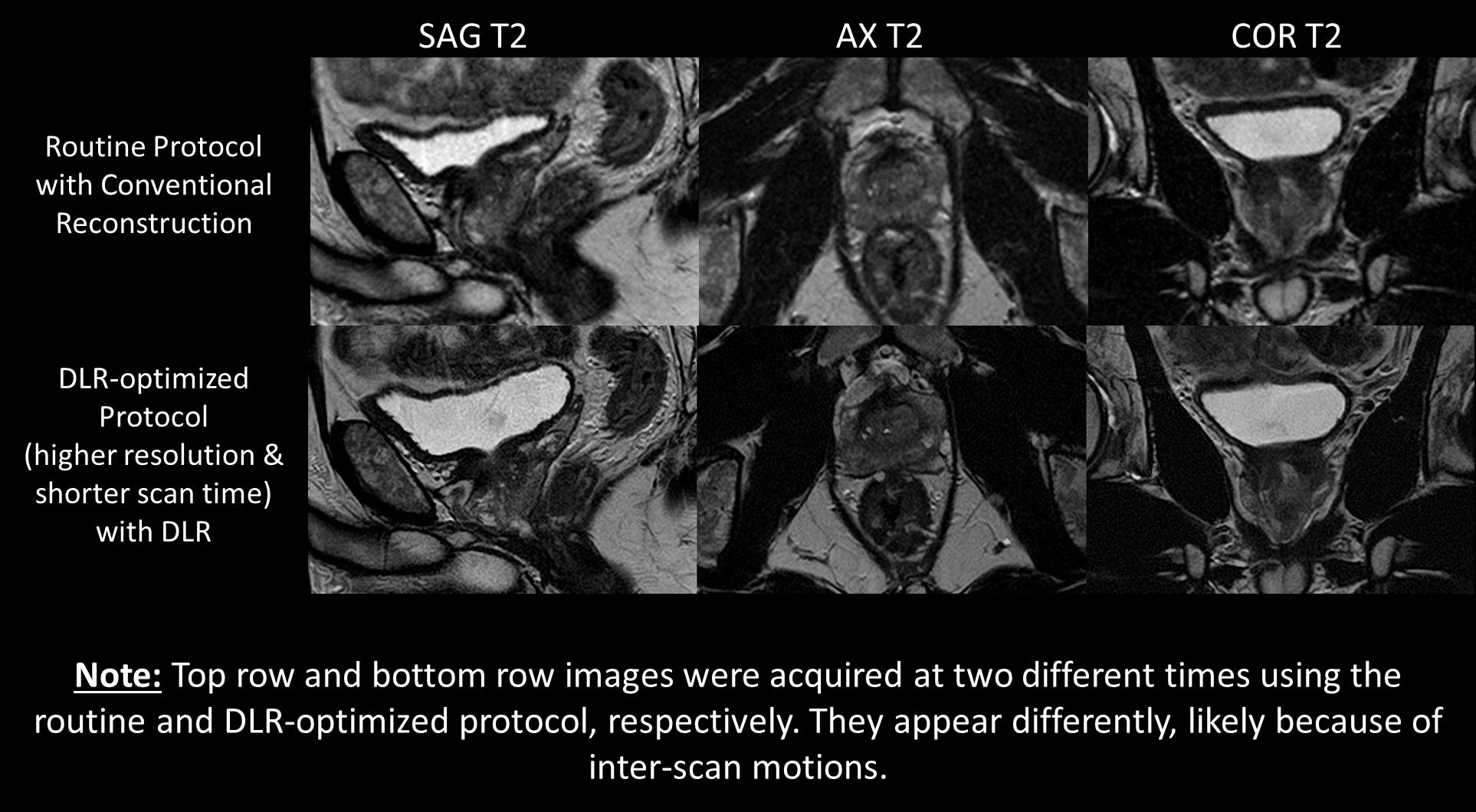
Figure 2: Representative images acquired using the
routine protocol reconstructed with the conventional reconstruction (top row)
and those acquired using the DLR-optimized protocol reconstructed with DLR
(bottom row). Despite the higher resolution and shorter scan time, DLR images
have similar SNR compared to routine images. The anatomical details are sharper
and better delineated in the DLR images likely because of higher resolution.
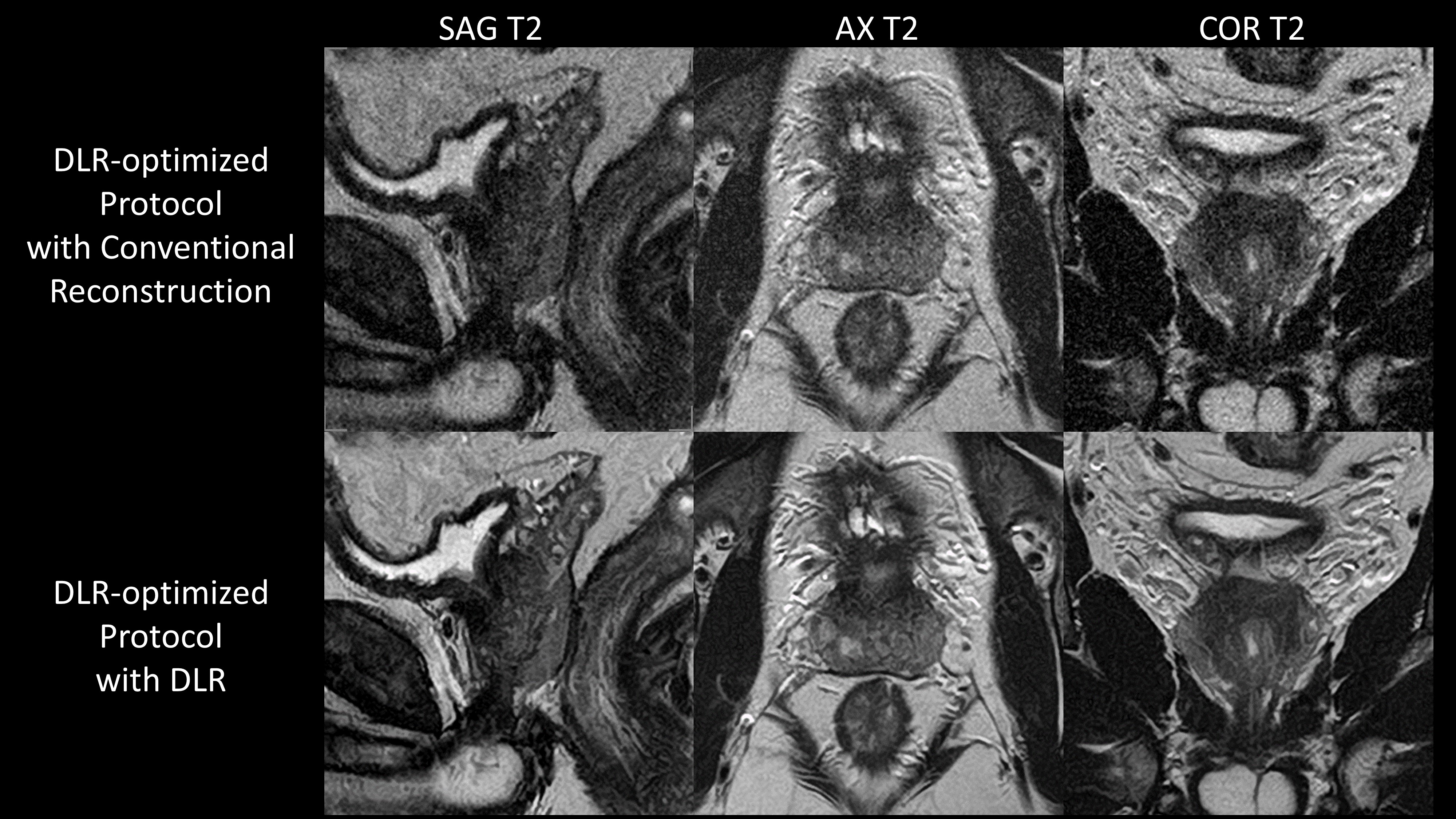
Figure 3: Images acquired using the DLR-optimized
protocol reconstructed using the conventional reconstruction (top row) and DLR
(bottom row). DLR increased SNR by 27.57%, 19.71%, and 27.13% for SAG T2, AX
T2, and COR T2, respectively.
DOI: https://doi.org/10.58530/2023/4200