4170
Feasibility and Preliminary Evaluation of Breath Hold and Free Breathing Quantitative Susceptibility Mapping of the Liver
Julia V Velikina1, Collin J Buelo1,2, Yan Wu3, Marcus T Alley3, Moniba Nazeef4, Michael Jeng3, Alexey A Samsonov1, Scott B Reeder1,2,4,5,6, Shreyas S Vasanawala3, and Diego Hernando1,2
1Radiology, University of Wisconsin - Madison, Madison, WI, United States, 2Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 3Stanford University, Stanford, CA, United States, 4Medicine, University of Wisconsin - Madison, Madison, WI, United States, 5Biomedical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 6Emergency Medicine, University of Wisconsin - Madison, Madison, WI, United States
1Radiology, University of Wisconsin - Madison, Madison, WI, United States, 2Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 3Stanford University, Stanford, CA, United States, 4Medicine, University of Wisconsin - Madison, Madison, WI, United States, 5Biomedical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 6Emergency Medicine, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Keywords: Susceptibility, Liver
Quantitative susceptibility mapping (QSM) is a promising non-invasive technique for quantification of liver iron concentration. Abdominal QSM typically requires a breath-hold acquisition since respiration induces liver motion, which leads to blurring artifacts. However, some patients have trouble even with a short breath-hold, which necessitates development of free-breathing approaches. In this work, we report initial results on the feasibility of using the modified “butterfly” navigator approach in multi-echo imaging in conjunction with compressed sensing reconstruction to enable free-breathing liver QSM.Introduction
Excessive iron accumulation in the liver can lead to liver disease and eventual liver cirrhosis, hepatocellular carcinoma, diabetes mellitus or other endocrine disorders. Quantification of liver iron concentration (LIC) is needed for management of liver iron overload1. Liver biopsy is the most direct quantitative method of evaluating iron content; however, biopsy is an invasive procedure that carries its own risks, has limited reproducibility, and is not appropriate for long-term observation. Quantitative susceptibility mapping (QSM) has emerged as a promising non-invasive technique for assessment of iron content in the liver2-5.Typically, abdominal QSM acquisition is performed using multi-echo 3D SGRE acquisition during a breath hold as respiration induces liver motion with an amplitude of 5-9 mm, which translates into blurring and ghosting artifacts. The need for breath hold (BH) limits achievable spatial resolution, which may lead to bias in susceptibility measurements6-7. Further, some patients, especially pediatric ones, may have trouble holding their breath for 20 s. Thus, there is an unmet need for free-breathing (FB) QSM.
The so-called “butterfly” navigator has been proposed8 to measure local translational motion in FB acquisitions with negligible overhead. It has been successfully applied for retrospective motion correction in abdominal structural imaging. In this work, we report initial results on the feasibility of using the modified “butterfly” navigator approach in multi-echo imaging in conjunction with compressed sensing reconstruction9 to enable FB liver QSM.
Methods
With IRB approval and informed written consent, human subjects (n=6) with known or suspected iron overload were scanned at 3.0T (Premier, GE Healthcare) with FB and BH acquisitions.Free Breathing Data Acquisition and Reconstruction
Multi-echo 3D SGRE data were acquired with randomized order of phase encoding lines in k-space. A short navigator was acquired in the beginning of each echo. Respiratory motion signal was extracted from the navigator data as described in8 and used to bin all acquired data into four respiratory bins. Only the data corresponding to end expiration was used for reconstruction of source images for each echo time using compressed sensing with total variation constraint9 to compensate for the discarded k-space data. Total acquisition lasted about 6 min with FOV=340x310 mm2, 112 slices, voxel size=1.3x1.2x3 mm3, TR = 5.4 ms, FA=8°, five echoes with TEinit/ΔTE=1.4/0.6 ms.
Breath Hold Data Acquisition
Multi-echo 3D SGRE sequence was performed during a 22 s breath-hold the following parameters: axial orientation, FOV=420x336 mm2, 68 slices, voxel size=1.6x1.3x4 mm3, TR=5.5 ms, FA=8°, six echoes with TEinit/ΔTE=0.74/0.57 ms.
QSM Processing
The reconstructed source images from both FB and BH acquisitions were processed with a chemical shift encoded water/fat separation technique10 to estimate the field map, which was used, along with PDFF and R2*, as input data for the data-adaptive QSM algorithm11.
Results
Figure 1 illustrates the importance of navigator data for removing spatial blur in FB acquisitions. Although navigator-gated images (right) are reconstructed from only part of the acquired k-space data (reduction factor ~2.25), its self-consistency together with compressed sensing reconstruction result in sharper source images. Figure 2 demonstrates the benefit of using FB acquisition in a human subject who had trouble holding breath, which led to artifacts in BH acquisition. Figure 3 shows examples of susceptibility maps obtained from FB (left) and BH (right) acquisitions from subjects with different LIC values. Susceptibility measurements in ROIs not affected by motion (ovals) produce similar values ($$$\chi_{BH}=$$$1.06/-0.213/-0.393 ppm, $$$\chi_{FB}=$$$1.09/-0.212/-0.402 ppm).Discussion and Conclusions
Our preliminary results suggest that free breathing acquisition with “butterfly” navigator for motion estimation and compressed sensing image reconstruction may be a viable alternative to obtain multi-echo source images for subsequent QSM processing. Such approach may be necessary for liver QSM in pediatric population and subject who have trouble with breath holds. Our future work includes evaluation of reproducibility of susceptibility measurements obtained in BH and FB acquisitions in a large cohort of human subjects with a wide range of LIC values.Acknowledgements
The authors wish to acknowledge support from the NIH (R01 DK117354, R01 DK100651). Also, GE Healthcare provides research support to the University of Wisconsin.References
- Brittenham GM, Badman DG. Noninvasive measurement of iron: report of an NIDDK workshop, Blood, 2003;101(1):15-19.
- Chu Z, Cohen AR, Muthupillai R, Chung T, Wang ZJ. MRI measurement of hepatic magnetic susceptibility—phantom validation and normal subject studies. Magn Reson Med. 2004;52:1318–1327.
- Hernando D, Cook RJ, Diamond C, Reeder SB. Magnetic susceptibility as a B0 field strength independent MRI biomarker of liver iron overload. Magn Reson Med. 2013;70:648–656.
- Sharma SD, Hernando D, Horng DE, Reeder SB. Quantitative susceptibility mapping in the abdomen as an imaging biomarker of hepatic iron overload. Magn Reson Med. 2015;74(3):673-83.
- Jafari R, Sheth S, Spincemaille P, Nguyen TD, Prince MR, Wen Y, Guo Y, Deh K, Liu Z, Margolis D, Brittenham GM, Kierans AS, Wang Y. Rapid automated liver quantitative susceptibility mapping. J Magn Reson Imag. 2019;50(3):725–32.
- Karsa A, Punwani S, Shmueli K. The effect of low resolution and coverage on the accuracy of susceptibility mapping. Magn Reson Med. 2019; 81(3):1833–48.
- Zhu A, Colgan TJ, Reeder SB, Hernando D, Characterization of bias in quantitative susceptibility mapping with anisotropic imaging resolution: Studies in a numerical phantom, 3D printed liver phantom, and in vivo patient scans. In Proceedings of 27th Annual Meeting of ISMRM, (Montreal, Canada), p. 4925, 2019.
- Cheng JY, Alley MT, Cunningham CH, Vasanawala SS, Pauly JM, Lustig M. Non-rigid Motion Correction in 3D Using Autofocusing with Localized Linear Translations. Magn Reson Med. 2012;68(6) 1785–97.
- Candes EJ, Romberg J, Tao T. Robust uncertainty principles: exact signal reconstruction from highly incomplete frequency information. IEEE Trans. Inf. Theory 2006;52(3):489–509.
- Hernando D, Kellman P, Haldar JP, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010;63(1):79-90.
- Velikina JV, Zhao R, Buelo CJ, Samsonov AA, Reeder SB, Hernando D. Data Adaptive Regularization for Abdominal Quantitative Susceptibility Mapping. Published online July 23, 2022. Accessed September 17, 2022. http://arxiv.org/abs/2207.11416
Figures
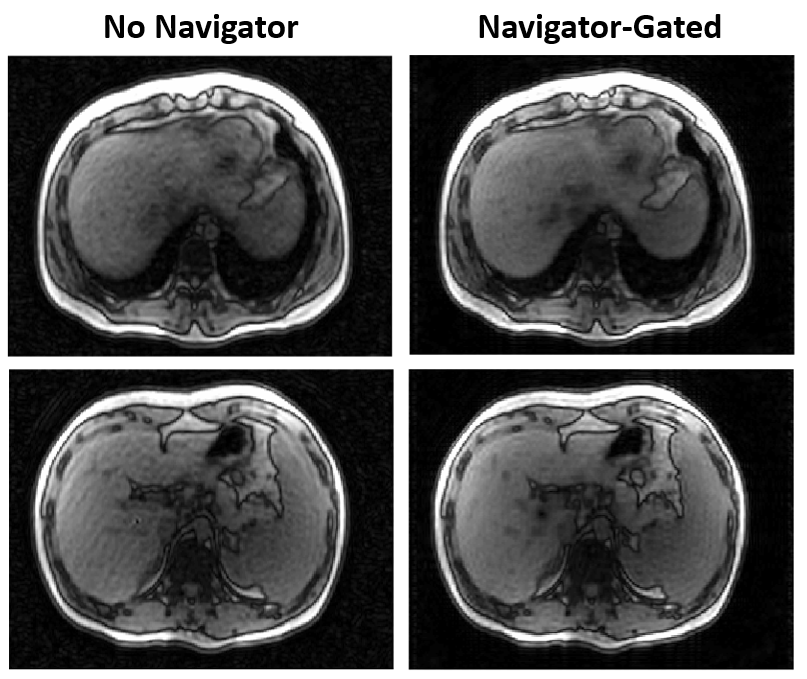
Figure 1. Free-breathing images reconstructed
from all acquired k-space data (left column, two slices shown) exhibit residual
artifacts and loss of spatial resolution, especially prominent in blurring of vessels and liver boundary. Binning the acquired data into
distinct respiratory states based on motion signal derived from “butterfly”
navigator allows freezing motion and improves image sharpness (right column).
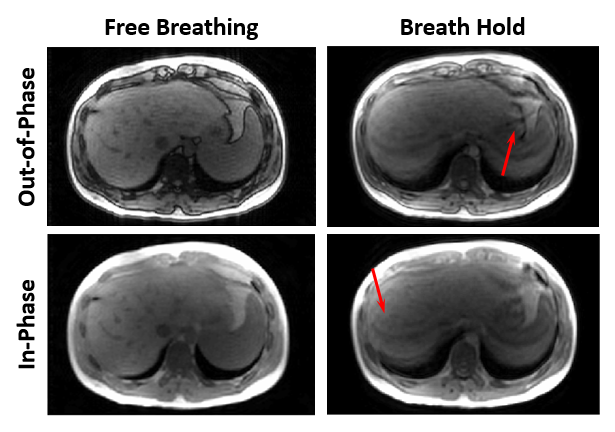
Figure 2.
Representative source images from examination of a human subject who had
trouble complying with breath hold directions. BH images (right column) suffer
from blurring and ghosting artifacts (arrows), while “butterfly” navigator-gated
FB images (left column) freeze motion in end-expiration position.
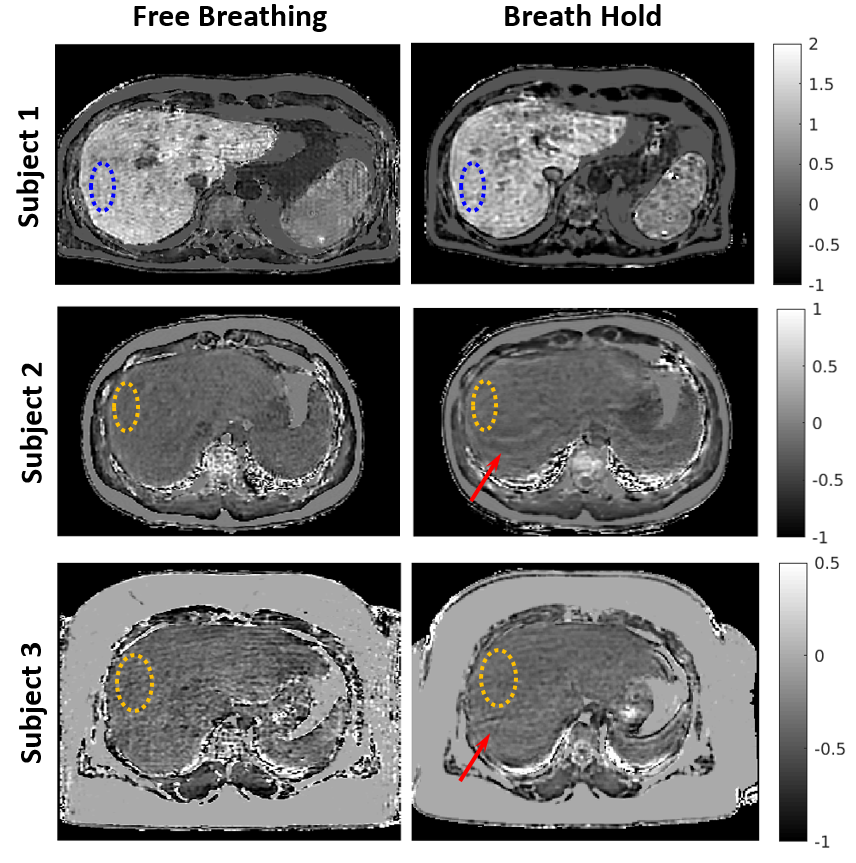
Figure 3. Examples of
susceptibility maps obtained from FB (left) and BH (right) acquisitions from
subjects with different LIC values. Note residual ghosting artifacts (arrows)
present in two out of three BH maps.
DOI: https://doi.org/10.58530/2023/4170