4156
Time-dependent diffusion MRI study of chemoradiation treatment response in patients with HPV positive oropharyngeal carcinoma
Eddy Solomon1, Steven H. Baete2, Joseph K. Kim3, Moses Tam3, Zujun Li4, Kenneth Hu3, Elcin Zan2, and Sungheon Gene Kim1
1Radiology, Weill Cornell Medical College, New York, NY, United States, 2Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Radiation Oncology, New York University Grossman School of Medicine, New York, NY, United States, 4Medical Oncology, New York University Grossman School of Medicine, New York, NY, United States
1Radiology, Weill Cornell Medical College, New York, NY, United States, 2Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Radiation Oncology, New York University Grossman School of Medicine, New York, NY, United States, 4Medical Oncology, New York University Grossman School of Medicine, New York, NY, United States
Synopsis
Keywords: Diffusion/other diffusion imaging techniques, Treatment
In this study, we evaluated the time-dependence of diffusivity and kurtosis in HPV-positive oropharyngeal squamous cell carcinoma patients before and during chemo-radiation treatment, as part of a study for adaptive de-escalation of the therapy. The non-deescalated patients with less than 40% nodal shrinkage had significantly higher diffusivity and lower kurtosis at pre-treatment than the de-escalated patients with more than 40% nodal volume shrinkage. The water exchange times were longer in the de-escalated patients than in the non-deescalated patients, although not significant. The prognostic accuracy of the pre-treatment imaging parameters was between 0.7 and 0.85.Introduction
Recent studies showed that a subgroup of head and neck cancer patients with human-papilloma virus (HPV)-positive oropharyngeal squamous cell carcinoma (OP-SCC) have significantly better prognosis1. These data lead to important considerations to de-intensify treatment for this low risk younger population, in order to reduce acute and chronic toxicity without compromising disease control. Diffusivity and diffusional kurtosis have been proposed as imaging markers to assess cell viability to evaluate the early treatment response2-6. However, most of previous studies were conducted with short diffusion times (~100 ms), and have not explored the full potential of diffusion MRI to measure specific tissue microstructural properties. In this study, we evaluate the prognostic value of time-dependent diffusional kurtosis as a measure of HPV-positive OPSCC with a wide range of long diffusion times (100-700 ms) for metastatic nodal shrinkage.Methods
The patients were recruited from an ongoing phase II institutional clinical research protocol, “Adaptive de-escalation of radiation therapy dose in HPV-positive oropharyngeal carcinoma (ART) demonstrating favorable mid-treatment response”. During the course of radiotherapy, all patients had a repeat CT and MRI scans at four weeks (week 4) of treatment to evaluate patient’s treatment response to chemo-radiation. Patients who had lymph node shrinkage > 40% at week 4 were given a dose de-escalated treatment regimen for a total dose of 60 Gy. Patients who did not meet the criteria received the standard treatment for a total of 70 Gy as initially planned (Figure 1).Thirty OPSCC patients (9 non-deescalated and 21 deescalated) were imaged on a Siemens 3T PRISMA system using a 20-channel head/neck coil. An in-house developed stimulated echo acquisition mode (STEAM) EPI sequence was used to acquire 5 diffusion times, [t=100,200,300,500,700 ms], over 4 b-shells [b=500,1000,2000,3000 s/mm2] with 3 diffusion directions along x, y, and z axes. The mixing time, tm, was [80,180,280,480,680 ms] varying with t. Other parameters included: TR=5000ms, TE=66 ms, resolution=1.5x1.5x4.0 mm3, FOV=190 mm, partial Fourier 6/8, and GRAPPA with R=2. Each patient was imaged twice: once before chemo-radiation treatment and then 4-weeks after starting the therapy.
Each set of images was registered over all b and t using an in-house deformable image registration tool. Figure 2 shows example of anatomical and b=0 images for one non-deescalated and one deescalated patient. Following post-processing, multi-slice regions of interest (ROI) were drawn for the largest lymph node in each patient. For each voxel in the ROIs, diffusion and kurtosis maps were generated via a model-based method assuming that for the range of t in this experiment, diffusion through the tumor can be considered Gaussian, where D(t) remains constant. In this regime, D is sensitive towards exchanging volume fractions, $$$ve$$$, whose water exchange time13 could be determined by modeling K(t) using the Karger model7:
$$D=(1-v_e ) D_e+v_e D_i=const$$
$$K(t)=K_∞+K_0\frac{2τ_{ex}}{t} [1-\frac{τ_{ex}}{t} (1-e^{-t⁄τ_{ex}} )]$$
where $$$K_∞$$$ marks the floor of diffusion kurtosis pertaining to the intrinsic tissue heterogeneity. From D and K(t), we can predict the diffusion weighted signal $$$Sp(t, b)$$$ using the cumulant expansion of signal including both D and K. Then, estimation of four parameters is conducted by minimizing the sum of squared differences between the predicted and measured signals for each voxel:
$$\left\{K_0, K_∞, τ_{ex},D_C\right\}=arg min ∑_{t,b}(S_p (t,b) - S_m (t,b))^2 $$
Results
The $$$D_C$$$, $$$K_0 $$$, and $$$K_∞$$$ of the de-escalated group at pre-treatment were significantly different (lower diffusivity and higher kurtosis) than those of the non-deescalated group (Fig. 3). The $$$K_0 $$$ of the de-escalated group at week-4 was found significantly higher than the non-deescalated group. The water exchange rates of the de-escalated group were also higher than the non-deescalated group, although without statistical significance. The prognostic value of the pre-treatment parameters were assessed using the receiver operating characteristic (ROC) curves (Fig. 4) and the prognostic performance measures (Table 1). The pre-treatment $$$D_C$$$ has the highest sensitivity (90%) and accuracy (0.85), while the kurtosis measures have 100% specificity.Discussion
The results of this study in terms of diffusivity are in agreement with previous studies which showed that lower diffusivity at pre-treatment was associated with favorable response to chemoradiation treatment3. It is remarkable that similar trend of diffusivity can be found among HPV-positive OPSCC patients who are known to have good prognosis in general. In addition, our results suggest that the diffusional kurtosis measures at week-4 can also be helpful to identify patients with good response. Further study is required to investigate how both diffusivity and kurtosis could be used at different treatment time points to reliably improve prediction and evaluate the treatment response. The water exchange times measured in this study at voxel-level appears to be in the expected range for cancer cells8-10. They also have the expected trend of longer exchange time with the de-escalated patients. Future studies will assess a potential association of the water exchange time as well as other diffusion parameters with long-term outcome of the treatment.Conclusion
This study with a small cohort of HPV-positive OPSCC patients demonstrates the feasibility of using diffusion MRI at relatively long diffusion times and the use of Karger’s model analysis to predict and evaluate the response to chemo-radiation therapy, and the potential of utilizing these parameters for identifying patients eligible for de-escalation treatment.Acknowledgements
NIH UH3CA228699, R01CA160620, R01CA219964, R01-EB028774, P41EB017183References
- Denis F., Garaud P., Bardet E., Alfonsi M., Sire C., Bergerot T.G., Rhein B., Tortochaux J., Calais G., Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 2004;22(1):69-76. 2.
- Padhani A.R., Liu G., Koh D. M., Chenevert T.L., Thoeny H.C., Takahara T., Dzik-Jurasz A., Ross B.D., Cauteren M.V., Collins D., Hammoud D.A., Rustin G.J.S., Taouli B., Choyke P.L., Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia 2009;11(2):102-125. 3.
- Kim S., Loevner L., Quon H., Sherman E., Weinstein G., Kilger A., Poptani H., Diffusion-weighted magnetic resonance imaging for predicting and detecting early response to chemoradiation therapy of squamous cell carcinomas of the head and neck. Clinical cancer research : an official journal of the American Association for Cancer Research 2009;15(3):986-994. 4.
- Thoeny H. C., and Ross B. D., Predicting and Monitoring Cancer Treatment Response with Diffusion-Weighted MRI. Journal of Magnetic Resonance Imaging 2010;32(1):2-16. 5.
- Jansen J. F., Stambuk H.E., Koutcher J.A., Shukla-Dave A., Non-gaussian analysis of diffusion-weighted MR imaging in head and neck squamous cell carcinoma: A feasibility study. AJNR American journal of neuroradiology 2010;31(4):741-748. 6.
- Goshima S., Kanematsu M., Kondo H., Yokoyama R. et al. Diffusion kurtosis imaging to assess response to treatment in hypervascular hepatocellular carcinoma. AJR American journal of roentgenology 2015;204(5):W543-549. 7.
- Jensen J.H., Helpern J.A., Ramani A., Lu H., Kaczynski K. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magnetic Resonance in Medicine 2005;53(6):1432-40. 8.
- Kim S, Quon H, Loevner LA, Rosen MA, Dougherty L, Kilger AM, Glickson JD, Poptani H, Transcytolemmal water exchange in pharmacokinetic analysis of dynamic contrast-enhanced MRI data in squamous cell carcinoma of the head and neck. Journal of Magnetic Resonance Imaging 2007; 26:1607-1617 9.
- Kim S, Loevner LA, Quon H, Kilger A, Sherman E, Weinstein G, Chalian A, Poptani H, Prediction of response to chemoradiation therapy in squamous cell carcinomas of the head and neck using dynamic contrast-enhanced MR imaging. AJNR 2010; 31:262-268 10.
- Springer CS, Li X, Tudorica LA, Oh KY, Roy N, Chui SY, Naik AM, Holtorf ML, Afzal A, Rooney WD, Huang W, Intratumor mapping of intracellular water lifetime: metabolic images of breast cancer? NMR in Biomedicine 2014; 27:760-773
Figures
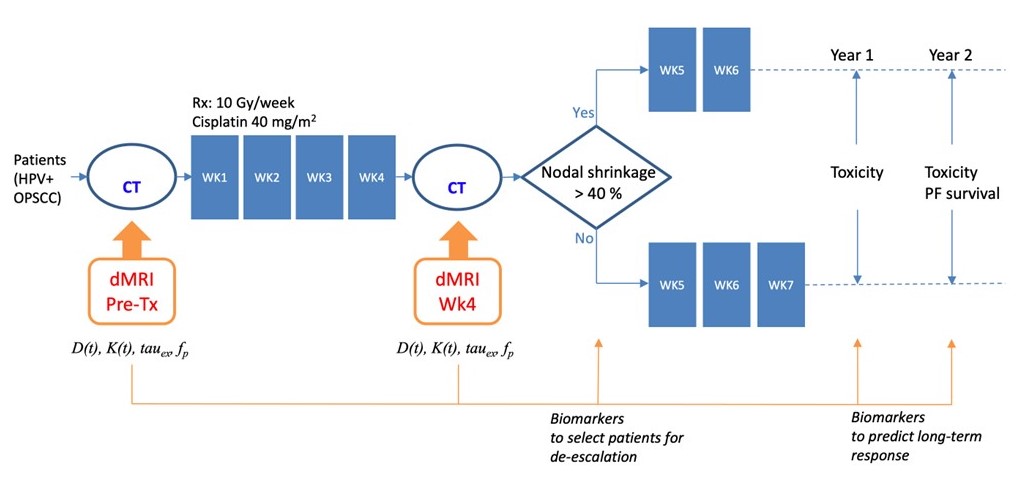
Figure 1. Schematic illustration of the diffusion MRI
study on de-escalation of chemoradiation therapy in HPV-positive oropharyngeal
squamous cell carcinoma.
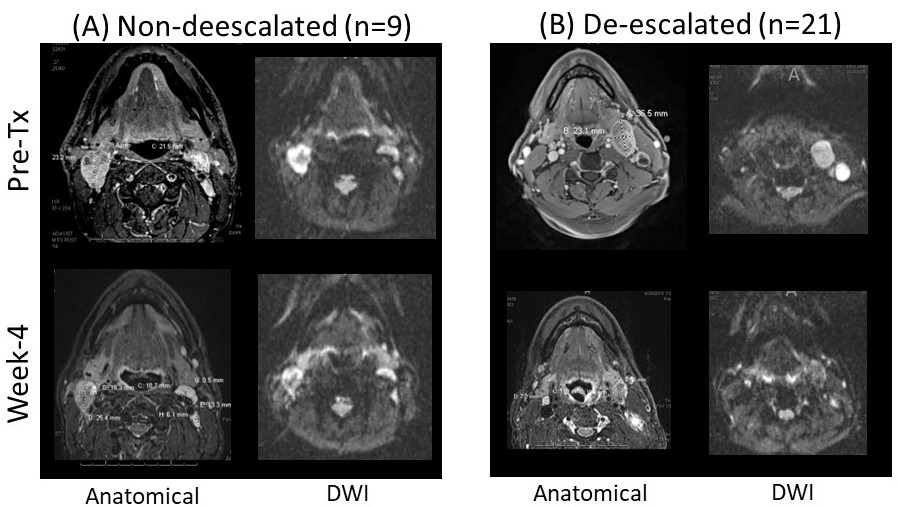
Figure 2. Example of anatomical and b=0 DWI images of a
non-deescalated and deescalated patients at pre-treatment and week-4 into the
treatment.
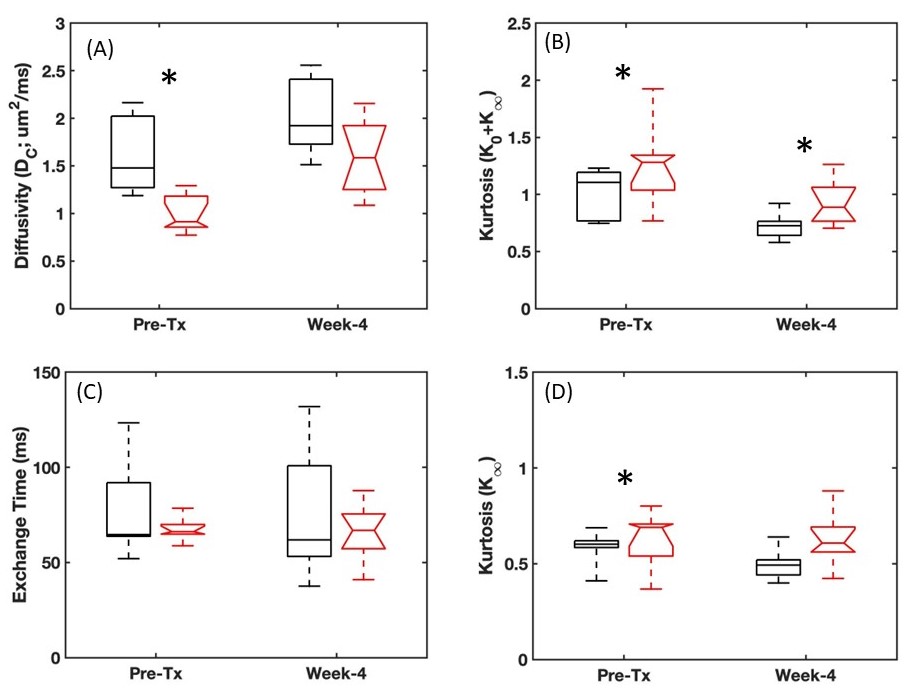
Figure 3. Box-whisker
plots of the Karger model parameters measured from the metastatic lymph nodes.
Black square boxes are for non-deescalated patients (n=9) and red boxes with
notches are for deescalated patients (n=21).
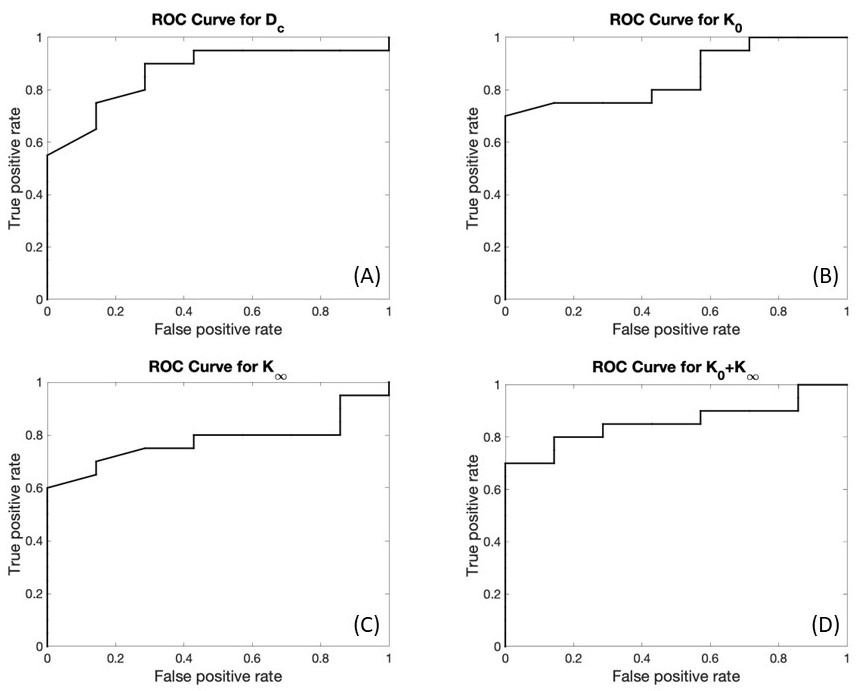
Figure 4. Receiver Operating Characteristic (ROC) curves of the
Karger model at pre-treatment MRI.
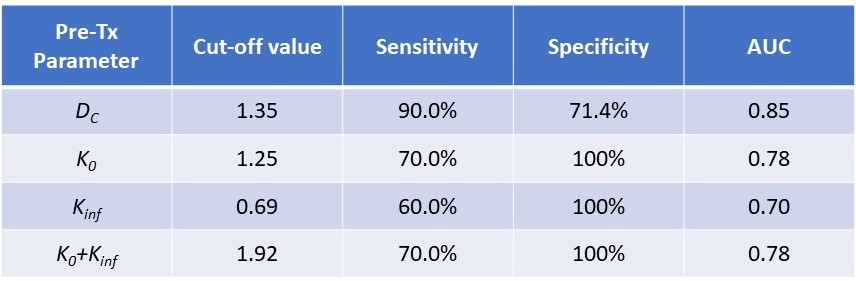
Table 1. Prognostic
performance of pre-treatment Karger model parameters for successful
de-escalation by meeting the requirement of nodal volume shrinkage > 40% by
Week-4.
DOI: https://doi.org/10.58530/2023/4156