4147
The predictive value of left ventricular strain analysis in myocardial infarction with ventricular remodeling1Graduate School of Dalian Medical University, Dalian Municipal Central Hospital, Dalian, China, 2The Affiliated Hospital of Dalian University of Technology, Dalian Municipal Central Hospital, Dalian, China, 3Graduate School of Dalian Medical University, Dalian Municipal Central Hospita, Dalian, China
Synopsis
Keywords: Cardiomyopathy, Ischemia, CMR-feature tracking
The subtle changes of myocardial strain in patients with myocardial infarction complicated with ventricular remodeling remain unclear. We used the CMR-FT technique to investigate the degree of strain damage, the degree of scar tissue penetration and the long-term prognostic value after ventricular remodeling in 41 patients with old myocardial infarction.The results showed that the myocardial strain was of great value in quantitatively assessing the degree of myocardial damage, identifying the degree of scar tissue penetration in infarcted myocardium and predicting the long-term end events, especially GLS, which was the best predictorBackground
Not all patients with acute myocardial infarction receive cardiac magnetic resonance (CMR) examination. For people with myocardial infarction for more than one month, the evolution of myocardial strain after ventricular remodeling is still unclear.Objective
To explore the value of cardiac magnetic resonance feature tracking (CMR-FT) in evaluating the degree of myocardial strain damage, the degree of scar tissue penetration, and the long-term prognosis after ventricular remodeling after myocardial infarction.Methods
41 patients with old myocardial infarction (n=41) and 28 healthy controls (n=28) were analyzed retrospectively. The left ventricular myocardial strain was measured by CMR-FT technique, including global peak longitudinal strain (GPLS), global peak circumferential strain (GPCS), global peak radial strain (GPRS), and 16 segment peak strain (PLS, PCS, PRS). Compare the difference in cardiac function and global peak strain between the two groups, evaluate the regional segmental strain of scar tissue in the myocardial infarction group and predict long-term adverse endpoint events (including all-cause death, heart failure, recurrent myocardial infarction, and malignant arrhythmia)Results
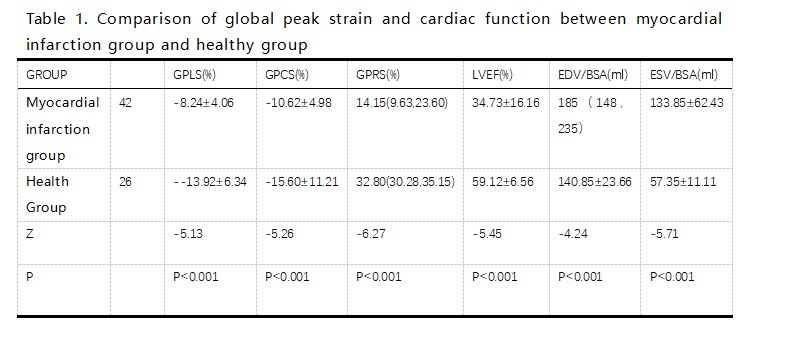
The comparison of cardiac function indexes and overall peak strain between the myocardial infarction group and the healthy control group is shown in Table 1. In the myocardial infarction group, GPLS, GPCS, GPRS, and LVEF were significantly damaged and were highly correlated with LVEF (r=-0.828, 0.890, -0.819, respectively, p<0.0001). Among them, GPLS and GPCS were negatively correlated with LVEF, while GPRS was positively correlated with LVEF(Table2). Segmental PLS and PCS were statistically significant in differentiating transmural scar tissue, non transmural scar tissue, and normal myocardial tissue. When PCS>- 8.8%, the sensitivity, and specificity of identifying transmural myocardial scar were 76% and 71% (AUC=0.77,95% CI 0.64-0.74, P<0.001), and when PLS>- 8.9%, the sensitivity, and specificity of identifying transmural myocardial scar were 75% and 60% (AUC=0.69,95% CI 0.721-0.816, P<0.001)(Fig1). Follow-up for 8-24 months in the infarct group showed that GLS, GCS, and infarct size (IS) were all valuable for predicting long-term endpoint events. The area under the curve (AUC) was 0.80 (95% CI 0.66 -0.93, p=0.002), 0.75 (95% CI 0.62 - 0.74, p=0.008), and 0.60 (95% CI 0.40 -0.80, p=0.036), respectively. The AUC of GLS and GCS is better than that of IS, and GLS has the best detection efficiency, with a cutoff value of -7.35%(Fig2).In multivariate logistic stepwise regression, only GLS can predict the occurrence of long-term endpoint events (0R: 1.1,95% CI 0.567-0.907, P=0.004)Conclusion
For patients with myocardial infarction and ventricular remodeling, the CMR-FT technology can quantitatively analyze the degree of myocardial damage, identify the degree of myocardial scar tissue penetration and predict the long-term endpoint event, especially GLS, which provides a reliable reference tool.Acknowledgements
No acknowledgement found.References
1.Driss A B, Lepage C, Sfaxi A, et al. Strain predicts left ventricular functional recovery after acute myocardial infarction with systolic dysfunction[J]. International Journal of Cardiology, 2020, 307.
2.Eitel I, Stiermaier T, Lange T, et al. Cardiac Magnetic Resonance Myocardial Feature Tracking for Optimized Prediction of Cardiovascular Events Following Myocardial Infarction[J]. JACC. Cardiovascular imaging, 2018: S1936878X17311762.
3.Reindl M, Tiller C, Holzknecht M, et al. Global longitudinal strain by feature tracking for optimized prediction of adverse remodeling after ST-elevation myocardial infarction[J]. Clinical Research in Cardiology, 2020(16).
4.Kammerlander A A , C Donà, Nitsche C , et al. Feature Tracking of Global Longitudinal Strain by Using Cardiovascular MRI Improves Risk Stratification in Heart Failure with Preserved Ejection Fraction[J]. Radiology, 2020, 296(2):200195.
5.Zghal F M, Boudiche S, Haboubi S, et al. Diagnostic accuracy of strain imaging in predicting myocardial viability after an ST-elevation myocardial infarction[J]. Medicine, 2020, 99.
6. Lange T, Stiermaier T, Backhaus S J, et al. CMR feature tracking remote myocardial strain analyses for optimized risk prediction following acute myocardial infarction[J]. European Heart Journal Cardiovascular Imaging, 2021, 22(Supplement_1).
7.Holzknecht M, Reindl M, Tiller C, et al. Cardiac magnetic resonance derived global longitudinal strain outperforms established functional parameters in prognostication after ST-elevation myocardial infarction[J]. European Heart Journal - Cardiovascular Imaging, 2021.
8.Bk A, Sds A, Sp B, et al. Tagged cine magnetic resonance imaging to quantify regional mechanical changes after acute myocardial infarction - ScienceDirect[J]. Magnetic Resonance Imaging, 2020, 66:208-218.
Figures
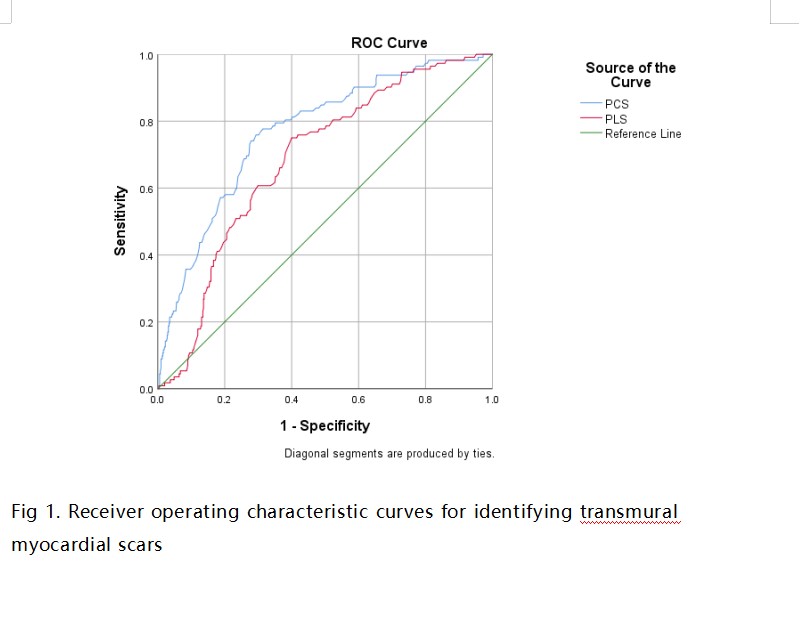
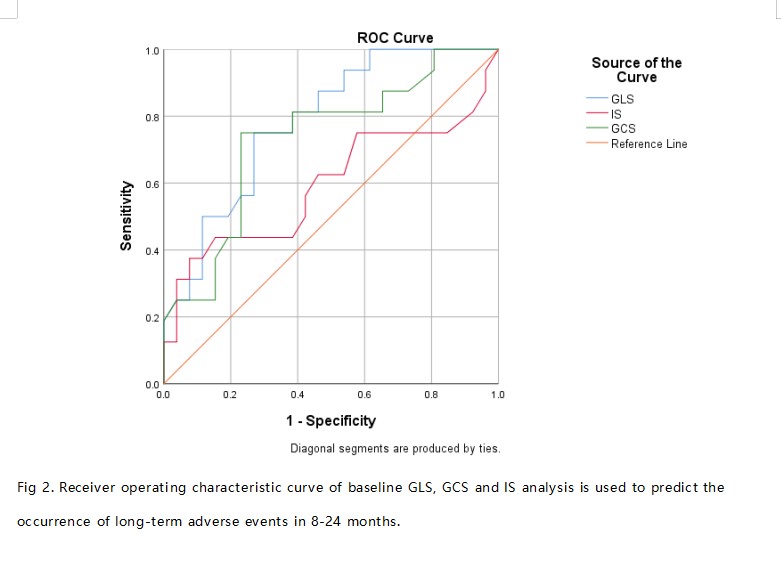
Figure2. Receiver operating characteristic curve of baseline GLS、GCS and IS analysis is used to predict the occurrence of long-term adverse event in 8-24 months