4145
Global Longitudinal and Global Circumferential Strain by Speckle-Tracking Echocardiography and Feature-Tracking CMRI: Comparison with LVEF
Jing Liang1, Dan Mu1, Xiance Zhao2, and Xiuzheng Yue3
1Department of Radiology, Affiliated Nanjing Drum Tower Hospital of Nanjing University Medical School, nanjing, China, 2Philips Healthcare, Shanghai, China, 3Philips Healthcare, beijing, China
1Department of Radiology, Affiliated Nanjing Drum Tower Hospital of Nanjing University Medical School, nanjing, China, 2Philips Healthcare, Shanghai, China, 3Philips Healthcare, beijing, China
Synopsis
Keywords: Atherosclerosis, Atherosclerosis
Understanding the relationship between left ventricular function and ventricular aneurysmafter myocardial infarction is crucial for surgical treatment and drug therapy. The CMR feature-tracking technique can quantitatively evaluate strain changes of LV and detect myocardial dysfunction. The study aims to use CMR-FT in patients with left VA after MI to assess strain changes and evaluate the clinical value for predicting patient prognosis. We found that the LV GLS, GCS, and GRS could be used for predicting the NYHA class after MI.Abstract
Ventricular aneurysm (VA) is a common mechanical complication of myocardial infarction (MI). It can be accompanied by ventricular appendage thrombosis, valvular regurgitation, ventricular wall rupture, ventricular tachycardia, or sudden cardiac death, with a high mortality rate and a poor clinical prognosis1. Effective and accurate detection of VA and the understanding of its relationship with left ventricular (LV) function could provide clinical guidance for surgical treatment and drug therapy. Cardiac magnetic resonance (CMR) feature-tracking techniques can quantitatively evaluate global longitudinal strain (GLS) and global circumferential strain (GCS) beyond the left ventricular ejection fraction (LVEF) and has higher sensitivity in the detection of myocardial dysfunction. The CMR feature tracking (CMR-FT) technique has been validated against the gold standard myocardial tagging and is now considered as a preferred CMR solution for strain assessment2. The purpose of this study is to use CMR-FT in patients with left VA after MI to assess strain changes and evaluate the clinical value for predicting patient prognosis. Methods Sixty-five patients, who underwent CMR with VA after MI from January 2018 to December 2019 in the Drum Tower Hospital Affiliated Hospital of Nanjing University School of Medicine, were selected for the study. They were divided into two groups based on the New York Heart Association (NYHA) classification after one year of follow-up: 25 cases of NYHA I as Group A and 40 cases of NYHA II-IV as Group B. CMR examinations were performed using an Ingenia CX 3.0T system (Philips Healthcare, Best, The Netherlands). A balanced steady-state free-precession (bSSFP) cine imaging with breath-hold and an ECG gating was acquired using a 32-element phased-array body coil. The LV strain and function parameters were generated based on cine imaging[1] . They were compared using Student's t-test (normal distribution) and Mann–Whiney's U test (nonnormal distribution) between Group A and Group B. The regression analysis was used to determine the significant parameters for predicting NYHA in patients with VA after cardiac infarction. Results The CMR characteristics for Group A and Group B are reported in Table 1. Patients in Group B (NYHA≥II) showed significantly lower LVEF (43.16 ± 7.73 vs. 36.84 ± 7.56; p=0.0018) and cardiac output (3.22 ± 0.94 vs. 2.68 ± 0.89; p=0.0234), and significantly more impaired LV GLS, GCS, and GRS (-12.34 ± 7.31 vs. -7.68 ± 6.11; p=0.0072, -21.31 ± 13.49 vs. -14.93 ± 10.44; p=0.0361, 37.13 ± 27.87 vs. 22.00 ± 20.05; p=0.0135) compared with patients in Group A (NYHA=I). The multivariate regression analysis indicated that GLS, GCS, and global radial strain (GRS) at baseline were independent and significant indicators of NYHA after cardiac infarction with VA (p=0.0015; p=0.0028; p=0.0013) (Table 2). After adjusting for age, sex, smoke, diabetes, hypertension, BNP, LDL, and medicine, GLS, GCS, and GRS at baseline remained independent and significant indicators of NYHA after cardiac infarction with VA (p=0.0007; p=0.0014; p=0.0012), as Table 3 demonstrates. Discussion&Conclusion[2] This study evaluates the myocardial strain in patients with VA after MI. We first found that the patients with poorer cardiac function have smaller LV GLS, GCS, and GRS, and the statistical results of strain parameters were consistent with the changes in CMR LVEF. Additionally, the LV GLS, GCS, and GRS could be used for predicting the NYHA class after MI. The strain analysis of VA after MI by CMR-FT could give early warnings to the NYHA of patients and provide important guidance for clinicians to judge the prognosis of patients, early drugs, surgery, and instrument treatment.Acknowledgements
All authors have no conflicts of interest.References
1. Durko AP, Budde RPJ, Geleijnse ML, Kappetein AP. Recognition, assessment and management of the mechanical complications of acute myocardial infarction. Heart. 2018;104(14):1216-1223.
2. Scatteia A, Baritussio A, Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance. Heart Fail Rev. 2017;22(4):465-476.
Figures
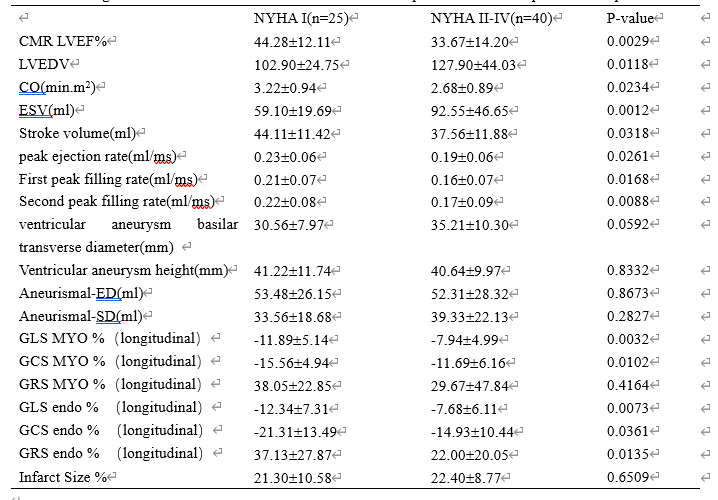
The significant
difference of cardiac strain and function parameters in Group A and Group B.
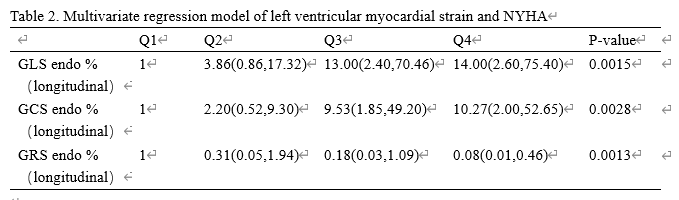
Multivariate regression model of left
ventricular myocardial strain and NYHA
DOI: https://doi.org/10.58530/2023/4145