4121
A comparative study of 2D SSFSE with deep learning based reconstruction and 3D FIESTA in the assessment of active inflammation in Crohn’s Disease
Yan Wang1, Jingyun Cheng1, Weiyin Vivian Liu2, and Yunfei Zha1
1Department of Radiology, Renmin Hospital of Wuhan University, Wuhan, China, 2MR Research, GE Healthcare, Beijing, China
1Department of Radiology, Renmin Hospital of Wuhan University, Wuhan, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: Digestive, Image Reconstruction
Higher resolution and better image quality of 3D FIESTA sequence is used for evaluating bowel inflammation in CD; however, we found 2D SSFSEDLwith significantly higher SNR and CNR of ileum and terminal ileum than 3D FIESTA and, of course, conventional 2D SSFSE. 2D SSFSEDL shortened scan time and also offered better image quality than 3D FIESTA in assessment of bowel inflammation in CD. The SSFSE sequence alone has been considered sufficient in lesion detection[2]; SSFSE with DLR has great potential in elevation of detection rate without extra imaging time.Introduction and Purpose
Crohn's disease(CD) is a chronic inflammatory disease that can affect any portion of the gastrointestinal tract. Endoscopy is commonly used to diagnose CD as the reference standard while magnetic resonance imaging has the advantage of being non-invasive and able to investigate small bowel involvement that cannot be reached by endoscopy. Previous studies have shown that fast imaging employing steady state acquisition(FIESTA) sequence was superior to single-shot fast spin echo(SSFSE) sequence in showing linear ulcers and pseudopolyps[1]. However, the scanning time of three-dimensional FIESTA(3D FIESTA)sequence is longer than that of two-dimensional SSFSE(2D SSFSE) sequence but provides higher resolution and better image quality. Deep learning reconstruction (DLR) is excellent at noise reduction without additional acquisition and post-processing time and has recently been introduced for clinical use. Our study aimed to explore the feasibility of 2D SSFSE with DLR (SSFSEDL) for evaluating bowel inflammation in CD using 3D FIESTA sequence as reference.Materials and Methods
Patients:Forty-seven patients with histological diagnosis of CD confirmed by endoscopy (36 male/11 female, age: 14–56 years) were prospectively recruited in this study. Imaging:All patients fasted for 6–8 hours prior to the scheduled exam time, and ingested 2000 mL of oral contrast agent (water with polyethylene glycol electrolytes powder dissolved) over 1 hour before magnetic resonance enterography (MRE) scan. All MRE scans were performed on a 3.0 T clinical MRI scanner (Signa Architect, GE Healthcare). Parameters of 3D FIESTA and 2D SSFSE sequences were shown in Table 1. 2D SSFSEDL and 2D SSFSE without DLR (SSFSEO) were automatically reconstructed with commercial DL-based reconstruction algorithm (AIRTM Recon DL). Assessment: Two radiologists made diagnosis in consensus and independently drew regions of interest on the bowel-segment of the suspected lesions to calculate signal-to-noise-ratio (SNR) and contrast to-noise-ratio (CNR). Representative MR images are shown in Figure 1. Statistical Tests: According to data normality and equality of variance, paired Wilcoxon signed-rank tests or paired t-test were performed to evaluate the statistical significance of differences in SNR and CNR between 2D SSFSEDL and SSFSEO, and between 2D SSFSEDL and 3D FIESTA. P value <0.05 was considered to be statistically significant.Results
SSFSEDL showed significantly higher SNR in jejunum (125.24±106.84 vs. 69.41±42.79, P=0.026), ileum (167.87±110.42 vs. 98.18±49.51, P=0.001) and terminal ileum (190.34±80.70 vs. 123.24±48.10, P<0.0001) than SSFSEO as well as in ileum (94.85±45.88, P=0.02) and terminal ileum (88.81±33.57, P<0.0001) than 3D FIESTA. SSFSEDL showed significantly higher CNR in jejunum (123.64±107.00 vs. 68.08±42.87, P=0.027), ileum (166.24±110.61 vs. 96.73±49.67, P=0.001) and terminal ileum (188.60±80.71 vs. 121.85±48.15, P<0.0001) than SSFSEO as well as ileum(93.29±45.87, P=0.02) and in terminal ileum (87.16±33.43, P<0.0001) than 3D FIESTA. There was no significant difference of SNR and CNR in jejunum between 2D SSFSEDL and 3D FIESTA (P = 0.477) (Figure 2).Discussion and conclusion
2D SSFSEDL showed overall better image quality, has shorter scanning time and consistent diagnosis performance on assessing bowel inflammation in CD with 3D FIESTA. The previous research showed that SSFSE has superior lesion detection rate and imaging ability on motion target to DWI. The SSFSE sequence alone might be sufficient in lesion detection[2]. With DLR SSFSE images, inter-observer agreement on the lesion detection rate elevated. The inline DLR SSFSE shortened scan time and increase patient compliance.Acknowledgements
No acknowledgement found.References
[1] Masselli G, Casciani E, Polettini E, Lanciotti S, Bertini L, Gualdi G. Assessment of Crohn's disease in the small bowel: Prospective comparison of magnetic resonance enteroclysis with conventional enteroclysis. Eur Radiol. 2006, 16(12):2817-27.
[2] Sohn B, Kim MJ, Koh H, Han KH, Lee MJ. Intestinal lesions in pediatric Crohn disease: comparative detectability among pulse sequences at MR enterography. Pediatr Radiol. 2014, 44(7):821-30.
Figures
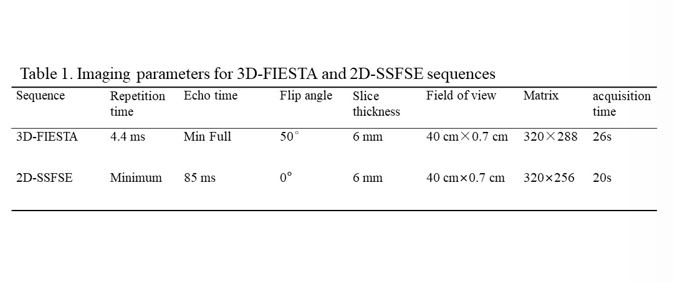
Table
1. Imaging parameters for 3D-FIESTA and 2D-SSFSE sequences
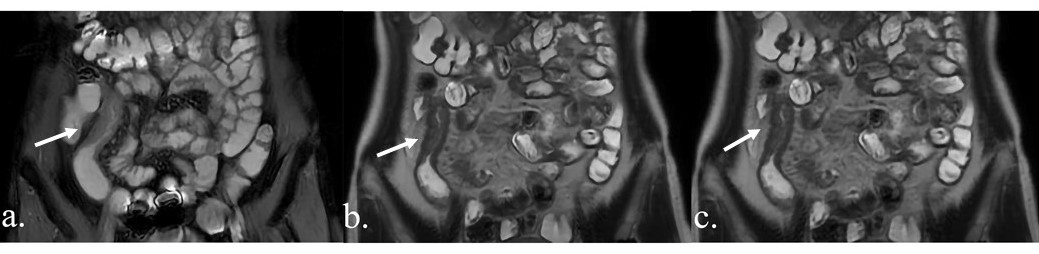
Figure
1: 3D-FIESTA (a), 2D-SSFSEDL (b), and 2D-SSFSEO (c) of a 36-year-old
female patient with active Inflammation in Crohn’s Disease. Uneven
thickening of the terminal ileum wall was more clearly displayed on both FIESTA
and SSFSEDL images.
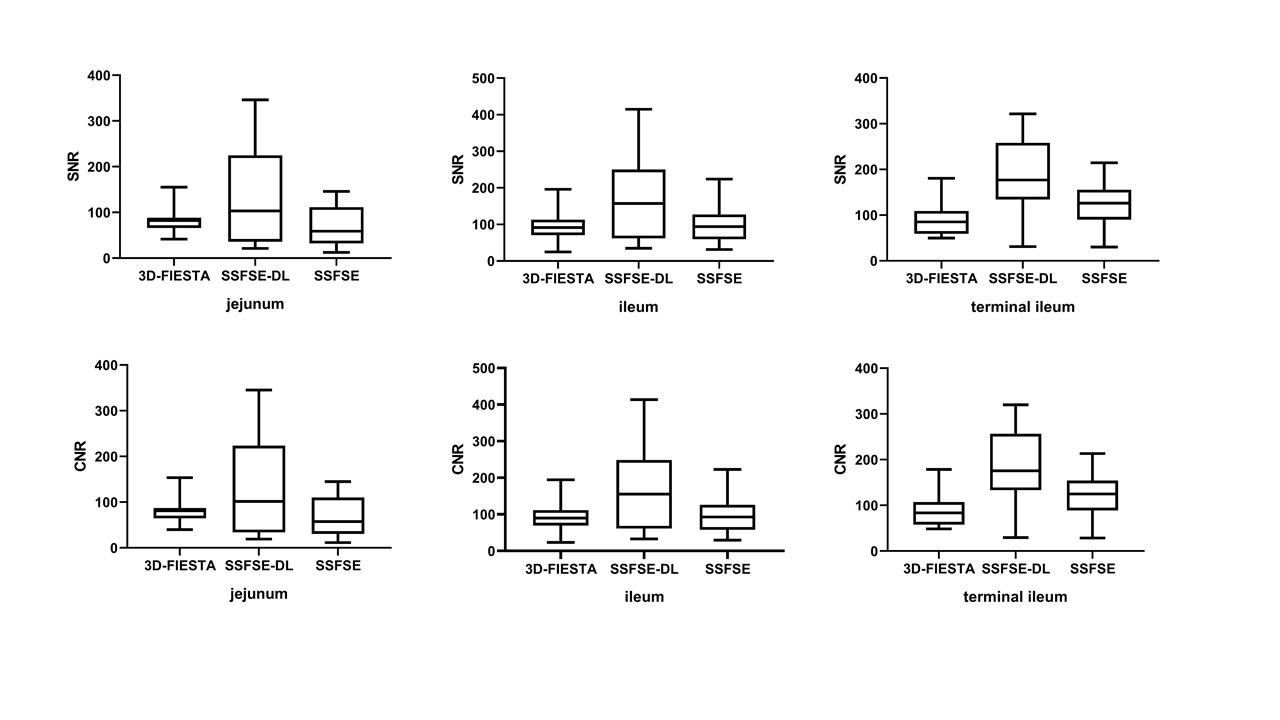
Figure 2 SNR and CNR for 3D-FIESTA, SSFSEDL
and SSFSEO.
DOI: https://doi.org/10.58530/2023/4121