4119
5T MRI of the pancreas in comparison to 3T: An initial study1Shanghai Institute of Medical Imaging, Shanghai, China, 2Department of Radiology, Zhongshan Hospital, Fudan University, Shanghai, China, 3Shenzhen United Imaging Research Institute of Innovative Medical Equipment, Shenzhen, China, 4MR Collaboration, Central Research Institute, United Imaging Healthcare, Shanghai, China
Synopsis
Keywords: High-Field MRI, Pancreas
Despite the growing clinical acceptability of magnetic resonance imaging (MRI) evaluation, continued efforts are required to increase the resolution and robustness of pancreatic imaging. The feasibility of pancreatic MRI at 5T was studied in this study, which used a brand-new 5T MR scanner. 5T pancreatic MRI exhibited greater signal-to-noise ratio (SNR) and sufficient image quality as compared to the 3T examination. Diffusion-weighted imaging (DWI) at 5T was sufficient for measuring the longitudinal pancreatic apparent diffusion coefficient (ADC). As a result, pancreatic MRI at 5T may be effective for diagnosing and managing pancreatic diseases.
Introduction
With exceptional soft tissue contrast, great spatial resolution, and no ionizing radiation, magnetic resonance imaging (MRI) has shown promise in the exploration of pancreatic disorders [1]. Many aspects influence the overall quality of pancreatic MRI, including signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), spatial resolution, and artifact level. Higher magnetic field strengths result in increased SNR, CNR, and resolution. The use of ultra-high-field whole-body MRI devices to examine their potential clinical uses is gaining popularity. However, increasing water-fat shift, susceptibility effects, and Larmor frequency all result in greater artifact levels at higher magnetic field strengths (>3T), especially for abdominal imaging. As a result, most ultra-high-field investigations have focused on brain and musculoskeletal imaging [2, 3]. Despite the growing clinical acceptability of MRI evaluation, continued efforts are required to increase the resolution and robustness of pancreatic imaging, as detecting tiny pancreatic lesions (less than 1 cm) remains difficult [4]. Furthermore, single-shot spin-echo echo-planar imaging (EPI) is the most often employed sequence for diffusion-weighted imaging (DWI) in pancreatic MRI. Traditional single-shot EPI-DWI sequences, on the other hand, are subject to susceptibility, which is notably noticeable in areas with strong magnetic susceptibility variations, such as the neighboring duodenum and jejunum [5]. Consequently, a more precise and efficient pancreatic imaging technology is needed. A whole-body 5T MRI scanner has recently been brought into research and clinical settings [6]. The goal of this work was to investigate the feasibility of imaging the pancreas at 5T and to compare the practical benefits of anatomical MRI and DWI with reduced field-of-view (FOV) at 5T to 3T.Methods
A cohort of 15 healthy subjects was recruited for this prospective study. MRI examinations were performed on both 3T (uMR 790, United Imaging Healthcare, Shanghai, China) and 5T (uMR Jupiter, United Imaging Healthcare, Shanghai, China) scanners. The MRI sequences included breath-hold T1-weighted volume interpolated gradient echo sequence with fat suppression (QUICK 3D) (For 3T, repetition time (TR)/echo time (TE) = 3.49/1.48 ms, flip angle (FA) = 15°; For 5T, TR/TE = 3.49/1.45 ms, FA = 20°; Other parameters were the same: FOV = 300×400 mm, Matrix = 408×544, Slice Thickness = 3 mm, 66 slices), T2-weighted fast spin-echo (FSE) (For 3T, TR = ~3472 ms (influenced by the respiratory cycle), TE = 98.34 ms; For 5T, TR, ~4520 ms (influenced by the respiratory cycle), TE = 87.66 ms; Other parameters were the same: FA = 100°, FOV = 120 × 280, and matrix = 226 × 528) and DWI with reduced FOV (For 3T, TR = ~4650 ms (influenced by the respiratory cycle), TE = 74.55 ms; For 5T, TR = ~5151 ms (influenced by the respiratory cycle), TE = 65.60 ms for 5T; Other parameters were the same: FA = 90°, FOV = 120 × 280, matrix = 246 × 576, and b-values = 0 and 800 s/mm2). Two experienced radiologists performed subjective image quality and artifacts analysis using a 4-point Likert scale independently. The signal-to-noise ratio (SNR) and apparent diffusion coefficient (ADC) values were assessed in the head, body, and tail of the pancreas. The degree of agreement between the two radiologists at qualitative analysis was assessed with the kappa statistic. A series of paired Wilcoxon tests were utilized to compare the subjective image quality, mean ADC value, and coefficient of variation (CV) of ADC between 3T and 5T measurements. P < 0.05 was regarded as statistically significant.Results
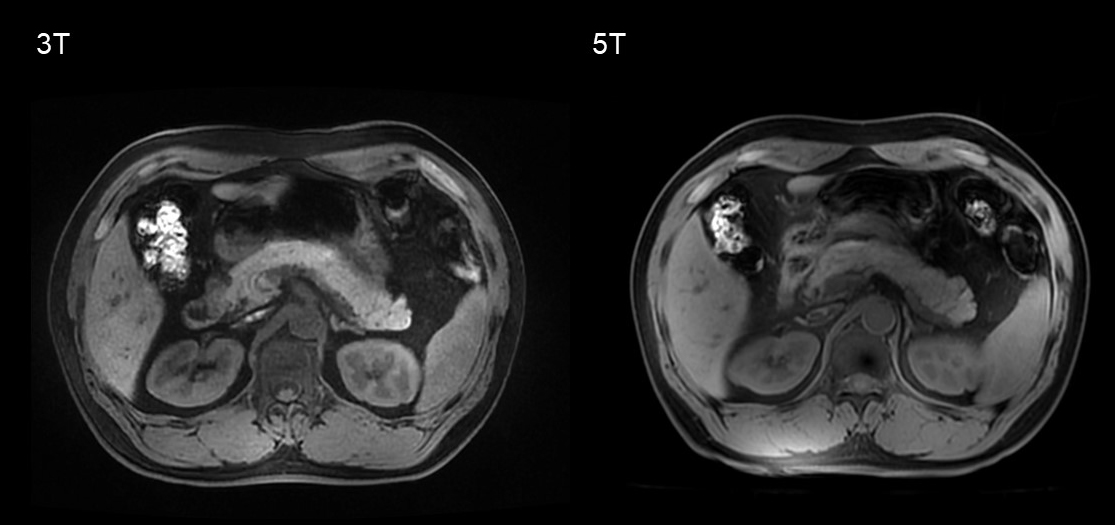
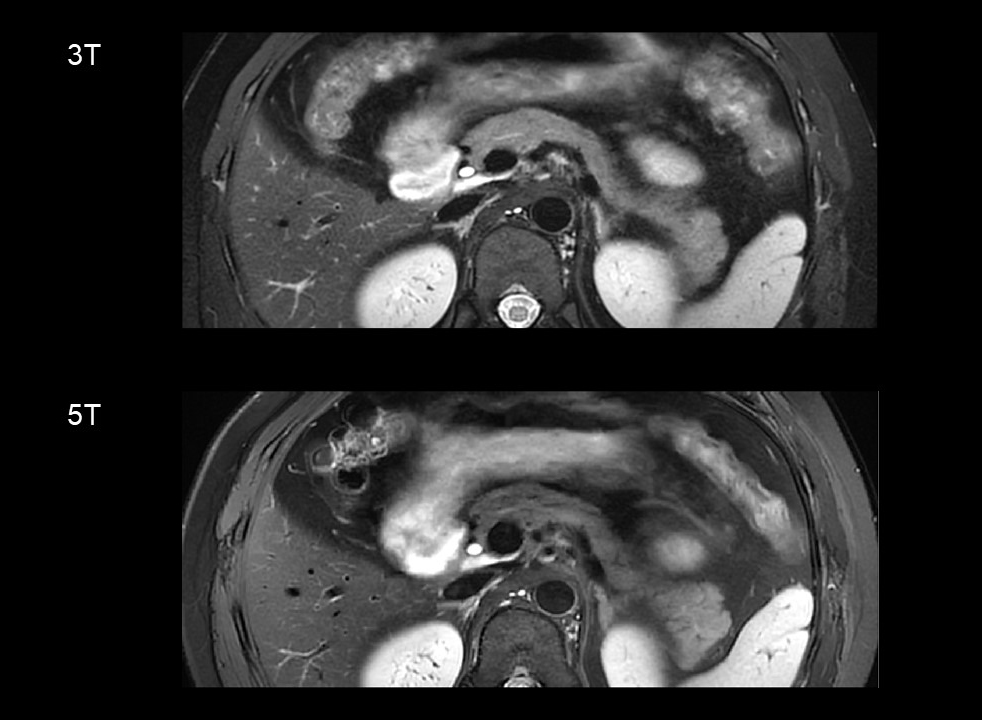
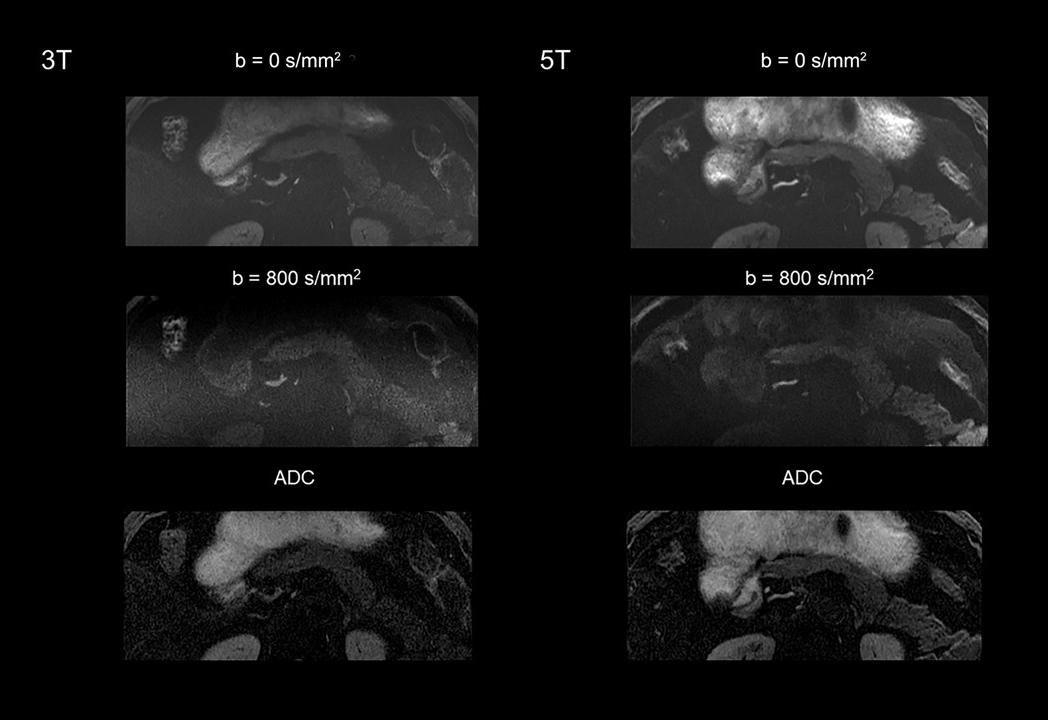
Figure 1-3 shows an example of 5T MRI and 3T MRI for each sequence. Interobserver agreement in image quality and artifacts was substantial to excellent for all sequences (κ > 0.7). Compared to the 3T examination, T1-weighted and DWI sequence at 5T showed significantly better image quality and comparable artifacts. For T2-weighted images, there was no significant difference in image quality ratings and the presence of artifacts between 3T and 5T. The mean ratios of SNR at 5 T to 3T of the T1-weighted images for the pancreatic head, body, and tail were 1.45, 1.35, and 1.48, respectively. For T2-weighted images, the corresponding ratios were 1.16, 1.33, and 1.39, respectively. For the DWI images (b = 800 s/mm2), the corresponding ratios were 1.29, 1.40, and 1.24, respectively. The SNRs of all the sequences were significantly higher at 5T than at 3T (P < 0.05 for all comparisons). For both 3T and 5T, mean ADC values on the pancreatic head were significantly higher than those of the tail (P = 0.016 for 3T, and P = 0.018 for 5T), while no significant difference was observed between the pancreatic head and body (P = 0.679 for 3T, and P = 0.445 for 5T). There was no significant difference in mean ADC values and CV of ADC between 3T and 5T (P > 0.05 for all comparisons).Discussion & Conclusion
In conclusion, this preliminary work demonstrated that 5T MRI was able to obtain pancreatic images with a better SNR and adequate image quality. DWI at 5T was sufficient for measuring longitudinal pancreatic ADC. As a result, pancreatic MRI at 5T may be effective for diagnosing and managing pancreatic diseases. More research on sequence optimization is needed to validate the current findings.Acknowledgements
No acknowledgement found.References
1. Kasban, H., M. El-Bendary, and D. Salama, A comparative study of medical imaging techniques. International Journal of Information Science and Intelligent System, 2015. 4(2): p. 37-58.
2. Verma, G. and P. Balchandani, Ultrahigh field MR neuroimaging. Topics in magnetic resonance imaging: TMRI, 2019. 28(3): p. 137.
3. Juras, V., et al., Magnetic resonance imaging of the musculoskeletal system at 7t: morphological imaging and beyond. Topics in Magnetic Resonance Imaging, 2019. 28(3): p. 125.
4. Saisho, H. and T. Yamaguchi, Diagnostic imaging for pancreatic cancer: computed tomography, magnetic resonance imaging, and positron emission tomography. Pancreas, 2004. 28(3): p. 273-278.
5. Thierfelder, K.M., et al., Parallel-transmit-accelerated spatially-selective excitation MRI for reduced-FOV diffusion-weighted-imaging of the pancreas. European journal of radiology, 2014. 83(10): p. 1709-1714.
6. Zhang, Y., et al., Preliminary Experience of 5.0 T Higher Field Abdominal Diffusion‐Weighted MRI: Agreement of Apparent Diffusion Coefficient With 3.0 T Imaging. Journal of Magnetic Resonance Imaging, 2022.
Figures