4118
Comparison of NATIVE-TrueFISP and 3D-SPACE in the magnetic resonance cholangiopancreatography of patients with ascites at 3T scanner
Lanbin Huang1, Jinglian Zhong2, Liping Liao1, Yingying Huang1, Zeping Liu3, Qingchun Li1, Qiceng Ruan1, Mingxia Tan1, Mengzhu Wang4, Shasha Liao5, Zehe Huang1, and Song Chen1
1Department of Radiology, The First People's Hospital of QinZhou, Qinzhou, China, 2Department of Radiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China, 3School of Biomedical Engineering, Guangzhou Medical University, Guangzhou, China, 4MR Scientific Marketing, Siemens Healthineers Ltd, Guangzhou, China, 5Department of Clinical Pharmacy, Maternity and Child Health care of Guangxi Zhuang Autonomous Region, Nanning, China
1Department of Radiology, The First People's Hospital of QinZhou, Qinzhou, China, 2Department of Radiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China, 3School of Biomedical Engineering, Guangzhou Medical University, Guangzhou, China, 4MR Scientific Marketing, Siemens Healthineers Ltd, Guangzhou, China, 5Department of Clinical Pharmacy, Maternity and Child Health care of Guangxi Zhuang Autonomous Region, Nanning, China
Synopsis
Keywords: Digestive, Biliary, MRCP
To compare the image quality of NATIVE-TrueFISP and 3D-SPACE in the MRCP of patients with ascites at 3T scanner. 5 patients with ascites and another 5 patients without underwent conventional upper abdominal MRI and MRCP with two kinds of sequences: NATIVE-TrueFISP and 3D-SPACE. The image quality of the two MRCP methods were independently assessed by two readers. Image quality of 3D-SPACE was superior to TrueFISP in patients without ascites while the TrueFISP sequence achieved better duct visualization in patients with ascites. Native TrueFISP can be used as an optional fast imaging sequence for MRCP of patients with ascites.Introduction and Purpose
The conventional three-dimensional variable flip-angle fast spin-echo (3D-SPACE) sequence is easily affected by peritoneal fluid, which leads to poor magnetic resonance cholangiopancreatography (MRCP) image quality. Thus, its clinically diagnostic usefulness in patients with ascites is compromised. Unenhanced NATIVE true fast imaging with steady-state precession (TrueFISP) technique is another frequently used sequence for MRCP. Whether TrueFISP can achieve optimal image quality of patients with ascites remains unknown. This study was designed to compare cholangiopancreatography image quality of NATIVE TrueFISP sequence and with that of 3D-SPACE sequence.Methods
5 patients with massive peritoneal fluid were classified as experimental group and another 5 patients without peritoneal fluid as control group. Participants of both groups underwent MR examinations on a 3T MR scanner (MAGNETOM Skyra, Simens Healthcare, Erlangen, Germany). All participants were studied after fasting for at least 8 h. The patients were placed in the supine position and a combination of body matrix and spine array coil were used. Afterwards, conventional coronal T2 weighted imaging and axial T2 weighted fluid attenuated inversion recovery imaging were performed. Then the MRCP images were acquired using respiratory-triggered Native-TrueFISP (FOV = 380mm×380mm, TR/TE = 2273ms/1.69ms, flip angle = 50°, slice thickness = 1.3mm, 56 slices, voxel size = 0.5mm × 0.5mm × 1.3mm, TI = 1600ms, GRAPPA (PE) = 2, and total acquisition time = 2 min 10 s) and 3D-SPACE sequences (FOV = 380mm ×380mm, TR/TE = 2400ms/703ms, flip angle = 120°. slice thickness = 1.3mm, 56 slices, voxel size = 0.5mm ×0.5mm × 1.3mm, GRAPPA (PE) =3, total acquisition time = 4 min 18 s). The maximum-intensity projection was performed on both series for further image analysis. The relative contrast ratio (CR) between the common bile duct and peribiliary tissue, overall image quality, suppression of background noise and visualization of pancreatic bile duct structure in both series were evaluated by two attending physicians on a five-point scale (Table 1).Results
All of the 10 patients successfully received MRCP. The CR and the quality scores of the major structures of the pancreaticobiliary system were shown in table 2 and table 3. The structure of the pancreaticobiliary ducts is visible in both groups. Image quality of 3D-SPACE was superior to TrueFISP in control group. In experimental group, however, the TrueFISP sequence achieved better duct visualization compared with 3D-SPACE.Discussion and Conclusion
MRCP is the most commonly used magnetic resonance water imaging technique to display bile duct and is mainly used for the diagnosis of obstructive bile duct disease [1]. The commonly used sequence for MRCP is the T2 weighted 3D-SPACE. However, the signal of space sequence is often reduced because of the dielectric effect which was caused by ascites [2]. Ascites makes the emitted RF pulse reflected or refracted in the ascites area and cannot be diffracted for propagation. In this way, there is a standing wave effect and penetration attenuated excitation, resulting in a reduction of the signal [3]. In addition, the large excitation and recombination flip angle of T2W TSE sequences make the local SAR values very high [4]. Therefore, in order to reduce the SAR value, the flip angle needs to be reduced, which further reduces the signal of the T2W images. In contrast, the Native-TrueFISP sequence can suppresses static tissue, blood and other liquid signal using a spatial selective inversion pulse, and highlight the non-inverted fluid entering into imaging volume during the TI period. The contrast of Native-TrueFISP, which mainly relies on the T2/T1 ratio, makes an extremely high contrast between fluid and tissue [5]. The Native -TrueFISP sequence also achieved a high bile duct signal regardless of the fluid. Compared with 3D-SPACE, it is not susceptible to the dielectric effect on peritoneal fluid. Therefore, Native TrueFISP can be used as an optional fast imaging sequence for MRCP of patients with ascites.Acknowledgements
We thank all the participants and the Scientific Cooperation department of Siemens healthineers for their support.References
[1]MacEneaney P,Mitchell MT,McDermott R. Update on magnetic resonance cholangiopancreatogrphy. Gastroenterology Clinics of North America.2002.31:731
[2]Heiland S. From A as in aliasing to Z as zipper: artifacts in MRI [J]. Clin Neuro radiol, 2008; 18: 25-36.
[3]Dietrich O, Reiser MF, Schoenberg SO. Artifacts in 3‐T MRI: physical background and reduction strategies. Eur J Radiol. 2008;65:29–35.
[4]Webb AG, Collins CM. Parallel transmit and receive technology in high-field magneticresonance neuroimaging [J]. Int J Imaging Syst Technol, 2010; 20: 2-13.
[5]Bieri,O.,Scheffler,K.Fundamentals of balanced steady state free precession MRI[J].Journal of magnetic resonance imaging: JMRI,2013,38(1):2-11.
Figures
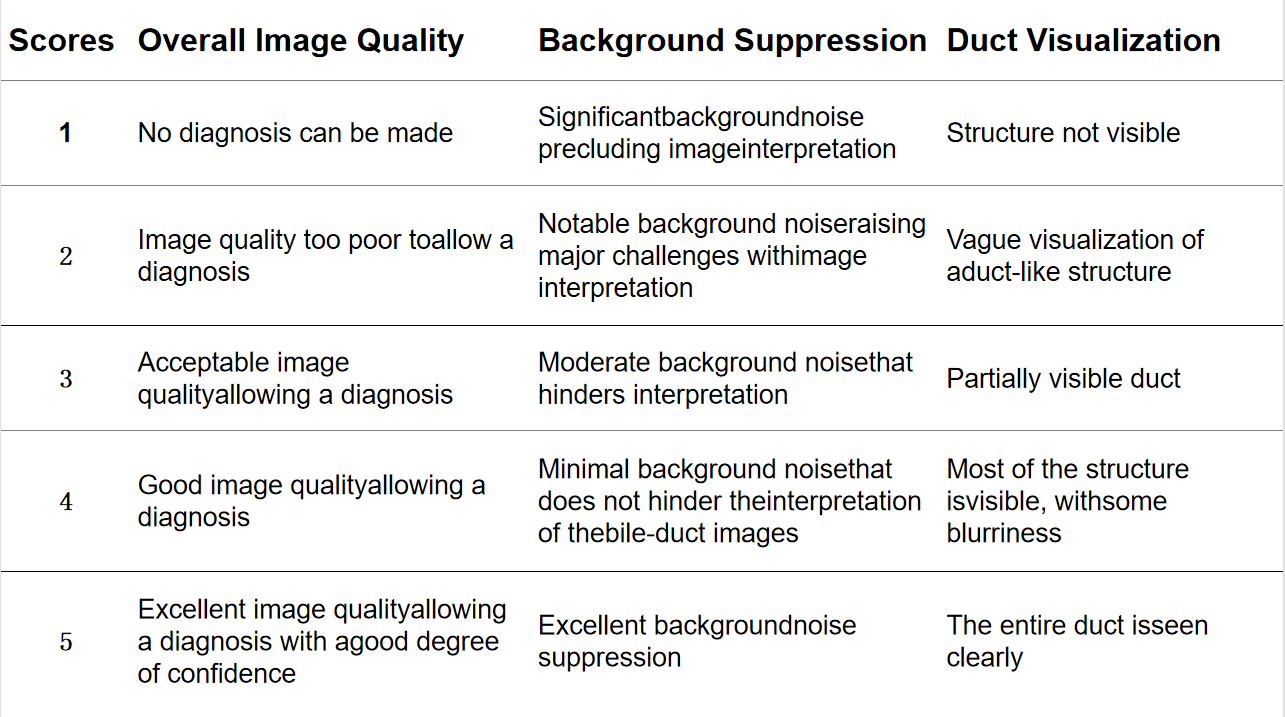
Table 1 Image quality scoring reference criteria
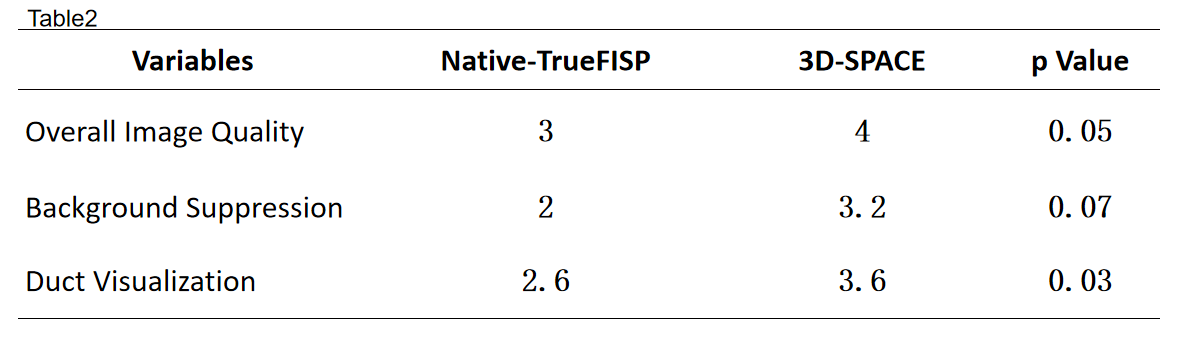
Table 2 Display rate and the quality score of MRCP in five patients with ascites
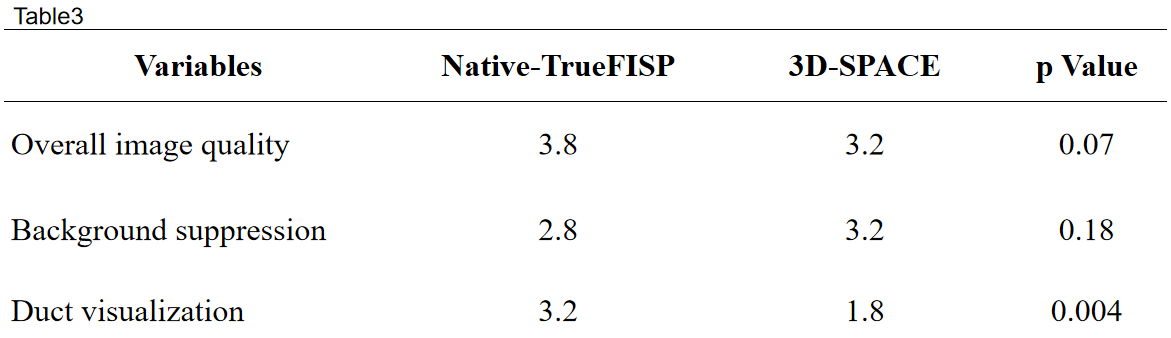
Table 3 Display rate and the quality score of pancreatic bile duct structure in 5 normal volunteers
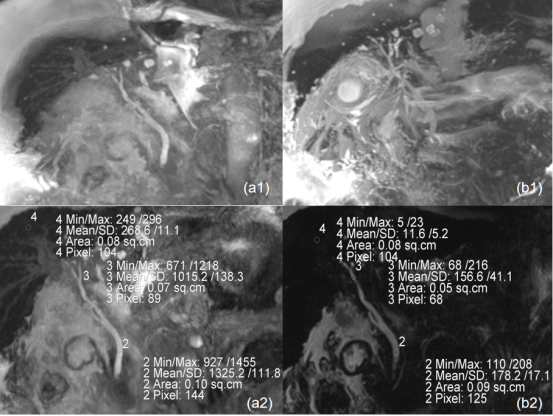
Figure 1 (a,b) MRCP images of a 67-year-old male patient with seroperitoneum on Native-TrueFISP and 3D-SPACE sequences,That the bile ducts and liver parenchyma are not affected by dielectric effects on the images of Native-TrueFISP (a2), whereas on the (b2) images of 3D-SPACE have reduced signal intensity.Representative section of the common bile duct (CBD) used for the quantitative evaluation of image quality: The regions of interest (ROIs) on the CBD and peri-biliary tissues . Note that the ROIs were drawn on the native images and not on the MIP reconstruction as shown here(a1,b1).
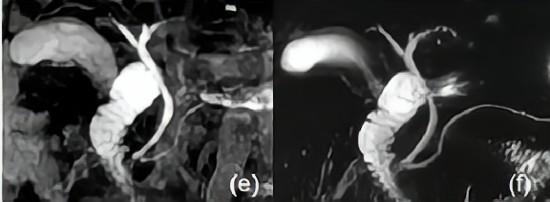
Figure 2 (e,f) MIP images of MRCP based on Native-TrueFISP sequence and 3D-SPACE sequence of a normal control. Where the Native-TrueFISP sequence (e) has less background suppression than the 3D-SPACE sequence (f).
DOI: https://doi.org/10.58530/2023/4118