4053
Axial diffusivity and kurtosis derived based on DWI reflect microstructure changes in patients with in stress urinary incontinence patients
Kun Ou1, Weiyn Vivian Liu2, and Kun Zhang1,3
1Department of Radiology, First Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, China, 2MR Research, GE Healthcare, Beijing, China, 3College of Integrated Traditional Chinese and Western Medicine, Hunan University of Chinese Medicine, ChangSha, China
1Department of Radiology, First Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, China, 2MR Research, GE Healthcare, Beijing, China, 3College of Integrated Traditional Chinese and Western Medicine, Hunan University of Chinese Medicine, ChangSha, China
Synopsis
Keywords: Muscle, Diffusion/other diffusion imaging techniques, Diffusion kurtosis imaging
Stress urinary incontinence (SUI) is the most common form of urinary incontinence. However, in patients with SUI, the pelvic floor muscles generally have no obvious radiographic abnormalities. This study applied diffusion-weighted imaging with different analysis models and found that patients with SUI had significantly lower FA and Da values based on gaussian-distributed water movement and higher values in the Ka based on non-gaussian-distributed water movement compared to the healthy volunteers. This study showed both DTI and DKI derived parameters can detect microstructure changes in the the pubic visceral muscle of the SUI patients.Introduction
The prevalence of urinary incontinence is as high as 28% and stress urinary incontinence (SUI) is the most common form1,2. SUI is caused by involuntary loss of urine during coughing or laughing in which bladder pressure exceeds the capacity of holding closed3. The periurethral, paraurethral, and pubic-urethral connective tissue may be damaged during pregnancy and labor. In addition, the pubic visceral muscle forms the medial portion of the levator ani muscle and is susceptible to injury during childbirth4,5. Magnetic Resonance Imaging (MRI) is commonly used to visualize pelvic floor anatomy and pelvic floor muscle defects. However, in patients with SUI, the pelvic floor muscles generally have no obvious structural abnormalities6. Therefore, more imaging studies attempted to detect microstructural changes in the pelvic floor muscles via diffusion weighted imaging. Previous studies in assessment of skeletal muscle injury using diffusion tensor imaging(DTI) have confirmed significant different DTI-derived parameters such as decreased FA and increased MD for injured pelvic floor muscles7,8.Diffusion kurtosis imaging(DKI) is an extension of diffusion weighted imaging and more sensitive to changes in tissue microarchitecture 9. Therefore, this study aimed to explore the feasibility of DKI in evaluation of the muscle function between women with and without SUI.Material and methods
51 healthy volunteers and 54 patients with SUI underwent pelvic floor examination using routine MRI and axial DTI imaging on a 3.0-T MR scanner (Signa HDxt, GE Healthcare). DKI postprocessing was performed and analyzed on Advanced Workstation 4.6 (GE Healthcare). Three diffusional kurtosis (DK) maps including mean kurtosis (MK), axial kurtosis (Ka), and radial kurtosis (Kr) and four diffusion tensor (DT) maps containing fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (Da), and radial diffusivity (Dr) were obtained. The regions of interest (ROIs) was circled in bilateral pubic visceral muscles for three times and average.Results
There was no significant difference of all parameter in DKI sequence between the left and right sides. Patients with SUI had significantly lower values in the FA, Da (P < 0.05, P < 0.05) as well as higher values in the Ka (P <0.05) compared with the healthy volunteers. (Table 1). In the healthy volunteers, the Da was significantly higher than Dr (P < 0.05). The Kr was significantly higher than Ka (P < 0.05).Discussion
We demonstrated diffusion-based models can reflect the function of bilateral pubic visceral muscles. Our study shows that patients with SUI had significantly lower values in the FA and Da, which is similar to previous studies.7,8 In the healthy volunteers, the Da was significantly higher than Dr. Da represents the diffusivity in the direction parallel to the length of the pubovisceral muscle fibers, and Dr represents the average diffusivity in all directions perpendicular to the length of the pubic visceral muscle fibers. Our result was consistent with the finding of the least restricted for water molecules along the longitudinal diffusion displacement of muscle fibers10. When muscle injuries, muscle fibrosis and fat accumulation disorganizes fiber bundles, leading to Da dropping. We also found patients with SUI had significantly higher values in the Ka than the healthy volunteers. In the healthy volunteers, the Kr was significantly higher than Ka. When K is greater than 0, a larger value indicates a larger deviation from the Gaussian distribution, and the K value is also positively correlated with the complexity of the internal microstructure 4,11. Ka refers to the kurtosis parallel to the length of the pelvic floor muscle fibers, and Kr refers to the average kurtosis of all directions perpendicular to the length of the pelvic floor muscle fibers. It is generally believed that the Kr value is larger than the Ka value, which may be related to the barrier of the endomysium, perimysium, cytoskeleton and capillary network, forming a more complex and heterogeneous microstructure in the vertical direction4. Similar to Da value, elevated Ka values in SUI patients may be due to edema, fat deposition, and fibrosis after muscle injury. Our results showed Ka and Da complement each other and both can reflect muscle injury.Conclusion
DKI sequence can detect changes in the microstructure of the pubic visceral muscle including lower Da and FA values and higher Ka values for SUI patients. It had potential in discovering functional alteration in injured muscle induced SUI.Acknowledgements
No acknowledgement found.References
- Falah-Hassani K, Reeves J, Shiri R, Hickling D, McLean L. The pathophysiology of stress urinary incontinence: a systematic review and meta-analysis. Int Urogynecol J. 2021;32(3):501-552.
- Minassian VA, Drutz HP, Al-Badr A. Urinary incontinence as a worldwide problem. Int J Gynaecol Obstet. 2003;82(3):327–38.
- D’Ancona C, Haylen B, OelkeM, Abranches-Monteiro L, Arnold E, Goldman H, et al. The international continence society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol Urodyn. 2019;38(2):433–77.
- Zhou H, Shang H, Li X, Tian M, Wei R. Measuring healthy female nulliparous pubovisceral muscle from diffusion kurtosis imaging. NMR Biomed. 2022;35(9):e4753.
- Abdool Z, Shek KL, Dietz HP. The effect of levator avulsion on hiatal dimension and function. Am J Obstet Gynecol. 2009;201(1):89.e1-89.e895.
- DeLancey JO, Morgan DM, Fenner DE, et al. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol. 2007;109:295-302.
- Heemskerk AM, Sinha TK, Wilson KJ, Ding Z, Damon BM. Repeatability of DTI-based skeletal muscle fiber tracking. NMR Biomed. 2010;23(3):294-303.
- Goh V, Tam E, Taylor NJ, et al. Diffusion tensor imaging of the anal canal at 3 tesla: feasibility and reproducibility of anisotropy measures. J Magn Reson Imaging. 2012;35(4):820-826.
- Jensen JH, Helpern JA. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010;23(7):698-710.
- Zijta FM, Froeling M, van der Paardt MP, et al. Feasibility of diffusion tensor imaging (DTI) with fibre tractography of the normal female pelvic floor. Eur Radiol. 2011;21(6):1243-1249.
- Lazar M, Jensen JH, Xuan L, et al. Estimation of the orientation distribution function from diffusional kurtosis imaging. Magn Reson Med. 2008; 60(4):774-781. doi:10.1002/mrm.21725
Figures
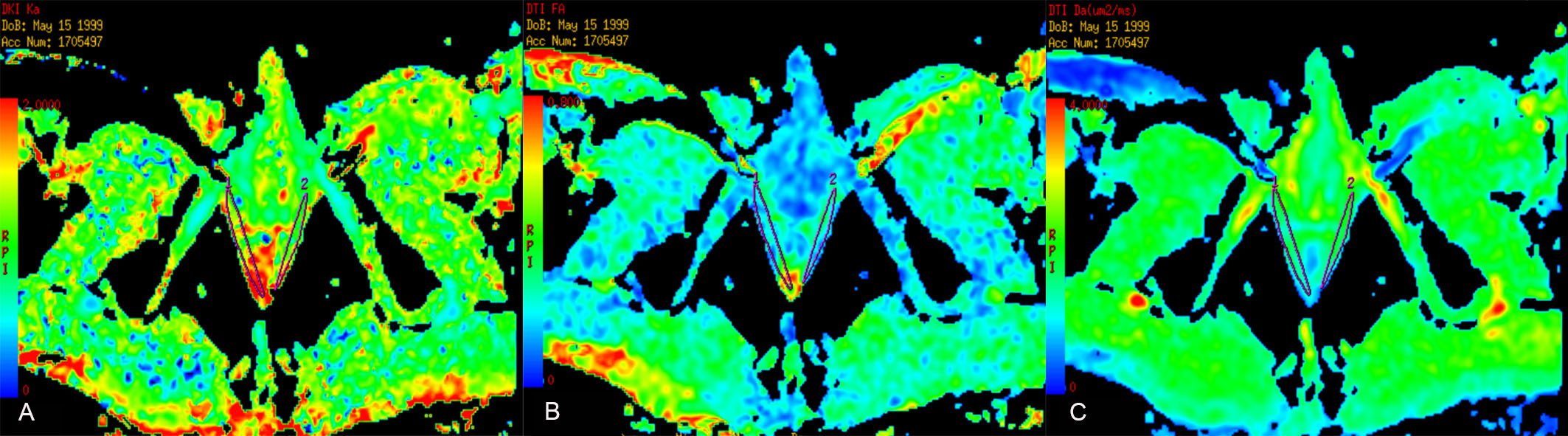
Figure 1 Representative regions of interest (ROIs) in
both pubovisceral muscles. (A) Axial kurtosis map; (B) Fractional
anisotropy map; (C) Axial diffusivity map
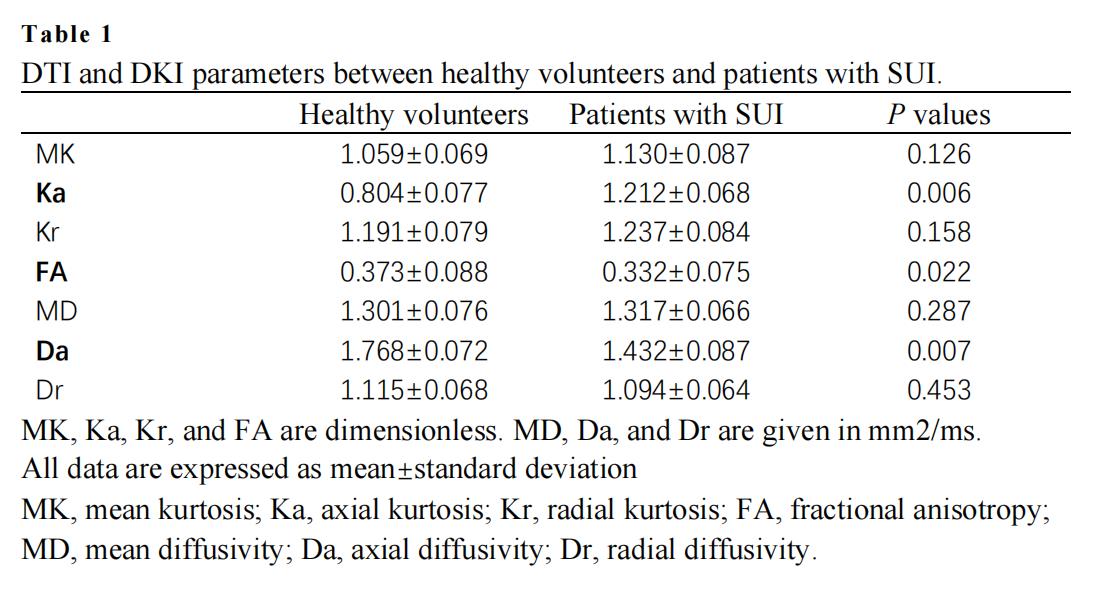
Table 1 DTI and DKI parameters between healthy volunteers
and patients with SUI.
DOI: https://doi.org/10.58530/2023/4053