4041
Deep Learning Based Reconstruction Improved Image Quality for rectum T2-weighted imaging1Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 2GE Healthcare, Shanghai, China, 3GE Healthcare, Beijing, China
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Image Reconstruction, rectum; magnetic resonance imaging; T2-weighted imaging
High-resolution MRI is of much significance in preoperatively staging rectal cancer. However, the motion artifact from intestinal peristalsis inevitably affects image quality then the accuracy of staging. Deep learning reconstruction (DLRecon) that uses artificial neural networks to extract patterns and makes predictions from large data sets, has been verified in related studies for improving image quality and reducing scanning time. In this study, rectum T2-weighted imaging (T2WI) reconstructed with DLRecon and conventional reconstruction were evaluated, and the results indicate that DLRecon could be employed for better image quality without extra scanning time in clinical practice.
Introduction
Rectal cancer accounts over 50% of colorectal cancers in Asia1. Nowadays, the diagnostic staging mainly depends on high resolution MRI, especially T2-weighted imaging (T2WI), to guide individual treatment. However, the relative long scanning time and thus introduced possible motion artifacts might decrease image quality then the staging accuracy.A vendor commercialized deep learning reconstruction method (AIRTM Recon DL, DLRecon), developed based on well trained convolutional neural networks (CNN) with curated database of over 4 million training iterations, has been recently proposed 2. This technique reconstructs MRI raw data in K space to achieve improved image quality with significantly reduced noise level, increased image sharpness and eliminated truncated artifacts3. Promising results have been reported in neural system4, cardiac imaging5 as well as abdominal organs of prostate3 and uterus6. With these promising findings, we assume DLRecon may also hold clinical potential in rectal MRI by improving the image quality. So far, no such studies have been implemented. Therefore, the main goal of this study was to first explore if DLRecon can improve the image quality for rectal T2WI.
Materials and Methods
SubjectsA total of 51 patients with primary rectal cancer were finally enrolled.
MRI acquisition
All patients underwent standard preoperative MRI examination on a 3.0T MR scanner (SIGNA Architect, GE Healthcare, USA) with 32-channels flexible coil employed. Routine and fast scan T2WI were acquired with 2min46s and 40s, respectively. Routine T2WI was reconstructed with DLRecon at three noise reduction levels (DLRecon-H: 75% noise reduction; DLRecon-M: 50% noise reduction; DLRecon-L: 25% noise reduction) and conventional reconstruction (cRecon). Fast scan T2WI was reconstructed with DLRecon-H and cRecon.
Data analysis
Signal-to-noise ratio (SNR) was used to quantitative analysis of the image quality. ROI-based mean values were measured by two experienced radiologists separately. Paired Samples Wilcoxon Signed Rank Test, Friedman Test and Student-Newman-Keuls Test were used for statistical analysis. P<0.05 was considered threshold of statistical significance.
Results
The DLRecon reconstructed routine T2WI with all three noise levels have significantly higher SNR of rectum than that of the corresponding images with cRecon (121.20±15.64, 71.00±20.77 and 57.80±16.16 for DLRecon-H, DLRecon-M and DLRecon-L respectively, vs. 40.24±10.77 for images with cRecon; all p<0.05). The SNRs of rectum were also significantly different among three noise reduction levels (higher level presented with higher SNR; p<0.05).For the fast scan T2WI, the rectum SNR of images with DLRecon-H (96.67±35.58) was significantly higher than that of corresponding images with cRecon (31.38±7.46) (P<0.05).
As shown in Figure 1, the T2WI clearly presented the details of the rectum lesion and surrounding structures. The rectum SNR of fast scan T2WI with DLRecon-H was higher than that of routine T2WI with cRecon (106.5 vs. 48.37) and comparable with that of routine T2WI with DLRecon-M (106.5 vs. 97.33). Both of two radiologists agree that the images from DLRecon have more distinct anatomical structures and details for further clinical staging.
Discussion and Conclusion
Rectum MRI can accurately evaluate the tumor location, tumor stage, extramural vascular invasion, and circumferential resection margin based on good image quality7. Motion artifacts including respiratory motion and intestinal peristalsis are inevitable factors affecting image quality. Improving image quality by traditional methods can greatly increase the scanning time, which is unacceptable for certain patients.A vendor commercialized DLRecon is a deep CNN denoising algorithm training from 4 million paired images with low and near-perfect image quality2. Pilot studies have shown that DLRecon images are sufficient to replace conventional scan images for clinical diagnosis with improved image quality and less scanning time 4-6.
In this study, we obtained images with better quality by DLRecon without increasing scanning time. Our results demonstrated DLRecon with all three noise reduction levels exhibiting significantly higher SNR while the high level has the highest values. The differences in images between each of the two DLRecon levels was also statistically significant. Moreover, DLRecon significantly improved the quality of fast scan T2WI with 40s acquisition time to the level that meets diagnostic needs, which is of practical meaningful for certain patients.
In conclusion, our results demonstrated that DLRecon method for the preoperative MRI scan of rectal cancer is feasible to improve image quality compared to standard imaging without extra scanning time and realize super-fast but sufficient scanning when needed. The point may be focus on preoperative T and N staging or restaging in further study based on DLRecon.
Acknowledgements
Thanks for the valuable technical support from Yong Zhang, Jiankun Dai and Guifeng Fu, GE Healthcare.References
1. Hammernik, K.; Klatzer, T.; Kobler, E.; et al. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med 2018, 79 (6), 3055-3071.
2. Lebel, R. M. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arXiv 2020, 2008 (06559).
3. Gassenmaier, S.; Afat, S.; Nickel, D.; et al. Deep learning-accelerated T2-weighted imaging of the prostate: Reduction of acquisition time and improvement of image quality. Eur J Radiol 2021, 137, 109600.
4. Kim, M.; Kim, H. S.; Kim, H. J.; et al. Thin-Slice Pituitary MRI with Deep Learning-based Reconstruction: Diagnostic Performance in a Postoperative Setting. Radiology 2021, 298 (1), 114-122.
5. Ogawa, R.; Kido, T.; Nakamura, M.; et al. Reconstruction of cardiovascular black-blood T2-weighted image by deep learning algorithm: A comparison with intensity filter. Acta Radiol Open 2021, 10 (9), 20584601211044779.
6. Tsuboyama, T.; Onishi, H.; Nakamoto, A; et al. Impact of Deep Learning Reconstruction Combined With a Sharpening Filter on Single-Shot Fast Spin-Echo T2-Weighted Magnetic Resonance Imaging of the Uterus. Invest Radiol 2022, 57 (6), 379-386.
(7) Wang, P. P.; Deng, C. L.; Wu, B. Magnetic resonance imaging-based artificial intelligence model in rectal cancer. World J Gastroenterol 2021, 27 (18), 2122-2130.
Figures
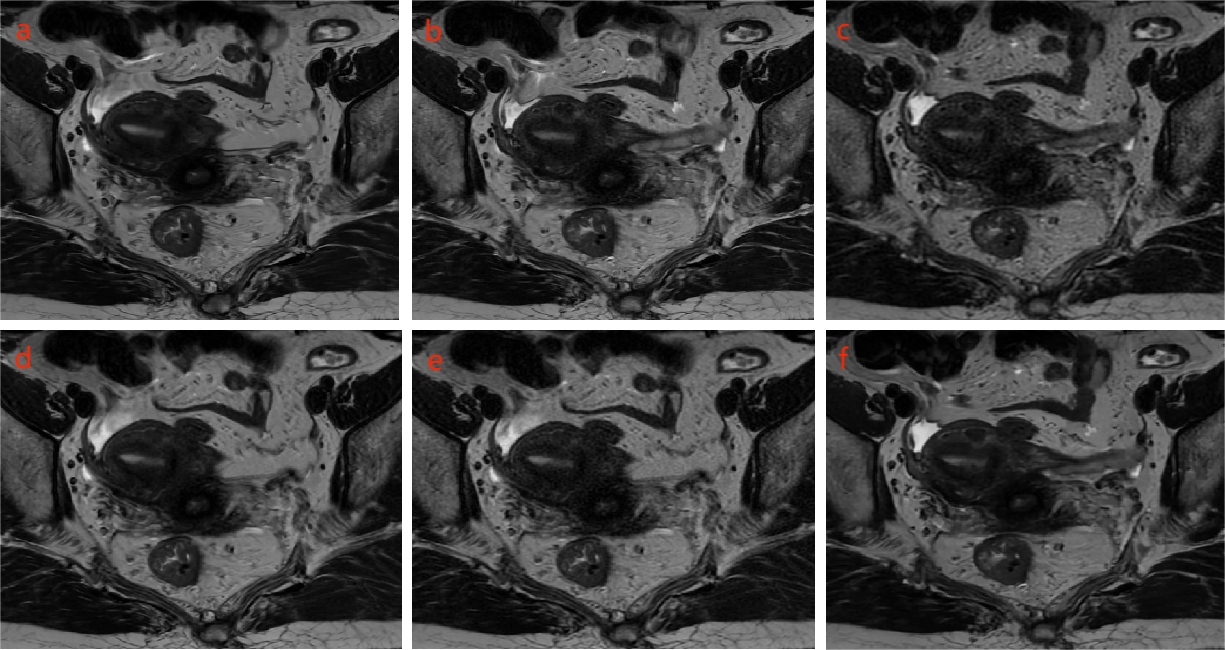
Figure 1. T2WI images with DLRecon and cRecon of the same patient. (a) DLRecon-H image, rectum SNR=146.44. (b) DLRecon-M image, rectum SNR=97.33; (c) DLRecon-L image, rectum SNR=73.70; (d) cRecon image corresponding to (a-c), rectum SNR=48.37. (e) Image from fast scan T2WI with cRecon, rectum SNR=27.86; (f) Image from fast scan T2WI with DLRecon-H, rectum SNR=106.65. DLRecon, deep learning reconstruction; cRecon, conventional reconstruction; SNR, signal-to-noise ratio; DLRecon-H, 75% noise reduction; DLRecon-M, 50% noise reduction; DLRecon-L, 25% noise reduction.