4025
Uncertainties in baseline cerebral oxidative metabolism mapping by gas-free and dual-calibrated fMRI: a simulation-based comparison1Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Rotman Research Institute, Baycrest Hospital, Toronto, ON, Canada, 3Institute of Biomedical Engineering, University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: fMRI, Metabolism
Calibrated BOLD fMRI is becoming a method of choice in assessing baseline cerebral oxidative metabolism (CMRO2), with gas-free calibrated fMRI being an non-invasive alternative to the more established gas-calibrated fMRI methods. However, the relative repeatabilities of these two approaches are unknown, each depending on a unique set of input measurements. This study uses analytical simulations to investigate the sensitivity of baseline OEF and CMRO2 estimates to the measured inputs of each method. Our results suggest that gas-free calibrated fMRI is substantially less sensitive to input variations than gas-calibrated fMRI, demonstrating the potential for simulation-informed methodological selection.Introduction
The assessment of quantitative cerebral oxidative metabolism (CMRO2) using MRI plays a valuable role in studying brain health1. Calibrated functional MRI (fMRI), specifically dual-calibrated fMRI, uses two different gas manipulations2 to enable mapping of baseline oxygen extraction function (OEF) and cerebral metabolic rate of oxygen (CMRO2)3. Gas-free calibrated fMRI, on the other hand, requires less set-up and is less demanding on the participants4, and is therefore better suited to certain patient populations. These two techniques each embodies a different set of input measurements, and to date, these two techniques have never been compared in terms of their sensitivity of resting metabolism measurements to variability in the input parameters. In this study, we use analytical simulation to assess the sensitivity of baseline OEF and CMRO2 estimates to variability in input parameters in each approach.Method
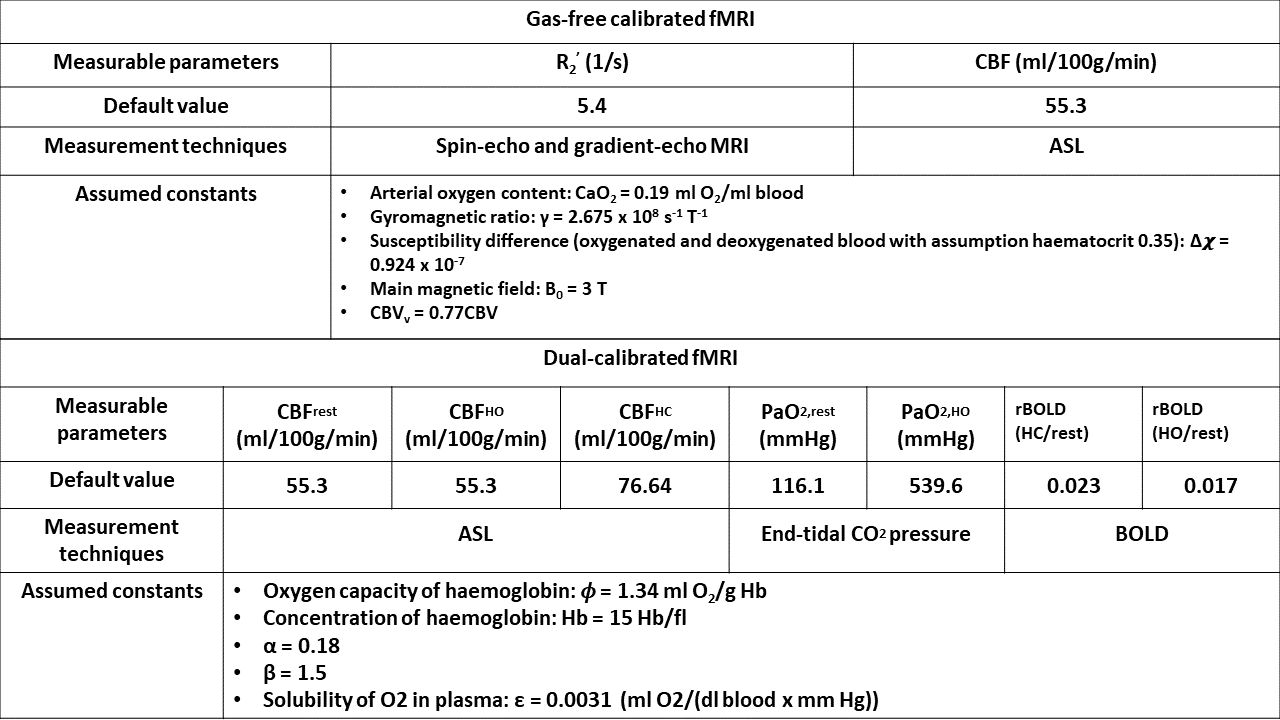
We performed an analytical simulation based on the parameters listed in Figure 1. The dual-calibrated fMRI model is defined by Eq. 1-6.$$rBOLD = \frac{\Delta\ BOLD}{BOLD}\;\;(1)$$
$$M=\frac{\frac{\Delta\ BOLD}{BOLD}}{1-(\frac{CBF}{CBF_{0}})^\alpha (\frac{[dHb]}{[dHb]_{0}})^\beta}\;\;(2)$$
$$\frac{[dHb]}{[dHb]_{0}}=\frac{((1-(\frac{1}{\phi [Hb]})(CaO_{2}-(CaO_{2}|_{0}\times OEF_{0}))}{1-\frac{CaO_{2}|_{0}}{\phi [Hb]}\times(1-OEF_{0})}+(\frac{CBF_{0}}{CBF}-1))\;\;(3)$$
$$CBV=\frac{0.0723CBF+1.144}{100}\;\;(4)\;\;(4)$$
$$CaO_{2}=\phi \times [Hb] \times SaO_{2} + PaO_{2} \times \epsilon \;\;(5)$$
$$SaO_{2}=\frac{1}{\frac{}{(PaO_{2})^3+150PaO_{2}}+1} \;\;(6)$$
rBOLD: fractional BOLD signal change to gas manipulations, where ∆BOLD is the difference of BOLD signal in two states (gas-challenge minus resting-state); ‘0’ indicates “resting”; [dHb]: dHb concentration; [Hb]: Hb concentration; M: maximum achievable BOLD signal amplitude; φ: O2 capacity of hemoglobin; α and β: constants used to model cerebral blood volume and transverse relaxation influence of dHb; PaO2: arterial oxygen tension; ϵ: solubility of O2 in blood.
Dual-calibrated fMRI relies on the calibration factor M, obtained by applying Eq. 2 to hypercapnic data, and OEF, obtained by applying Eq. 3 to hyperoxic data4. CaO2 was calculated by applying Eq. 5 and Eq. 6. In gas-free calibrated fMRI, OEF is given by Eq. 75, partially-deoxygenated cerebral blood volume (CBVv) is defined as 77%6 of total CBV, which based on Eq. 47.
$$OEF=\frac{R_{2}'}{\frac{4}{3}\times\pi \times \gamma \times \Delta \times \chi \times B_{0}\times CBV_{v}}\;\;(7)$$
$$CMRO_{2}=CaO_{2} \times OEF \times CBF\;\;(8)$$
R2’: reversible part of transverse relaxation rate; CBF: cerebral blood flow; γ: proton gyromagnetic ratio; and ∆χ: susceptibility difference between oxygenated and deoxygenated blood. CMRO2 for both approaches was calculated by eq. 88.
Baseline parameters are set based on a typical OEF (~0.4) suggested to be globally uniform by the previous research2. For each simulation, ±10% random variability was added to each of the measurable parameters while all other parameters were kept at default.
Results
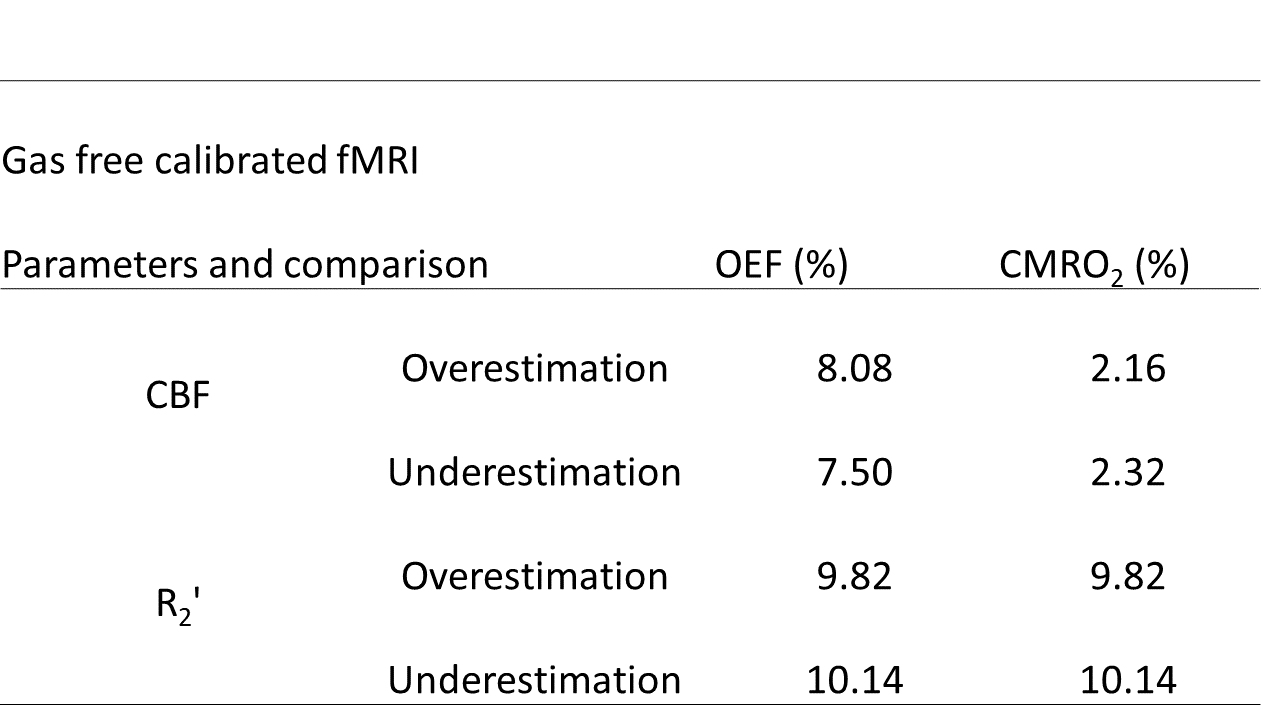
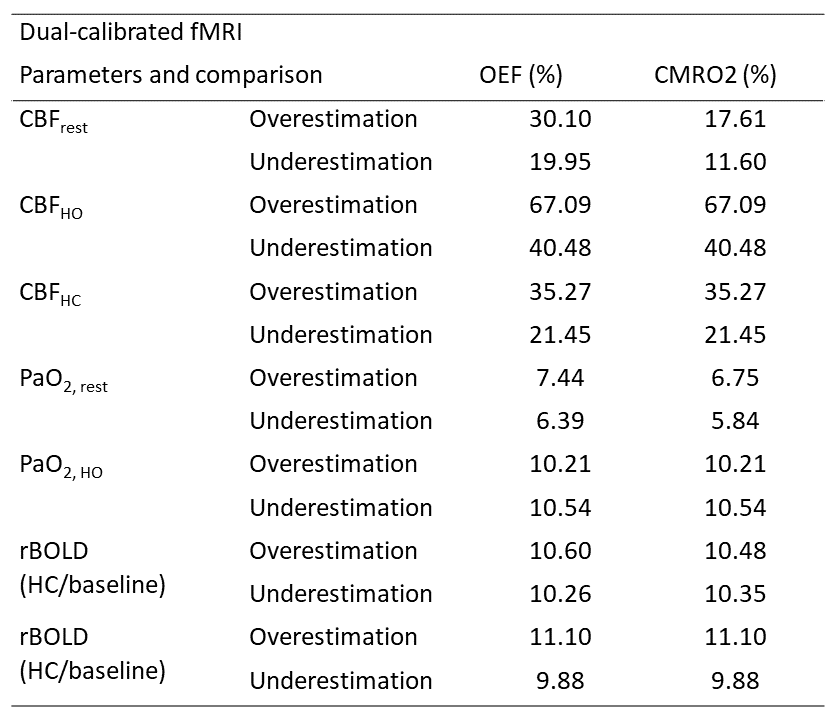
Figure 2 summarizes the simulated error range for OEF and CMRO2 given 10% variability in each measurable parameter for gas-free calibrated fMRI. OEF and CMRO2 estimation biases linearly dependent on R2’ measurement error and non-linearly dependent on CBF measurement error. However, CBF measurement errors have less impact on CMRO2 uncertainty.Similarly, Figure 3 summarizes the error ranges for dual-calibrated fMRI. Most of the measurable parameters in dual-calibrated fMRI exert a non-linear influence on the resultant estimation error in CMRO2 and OEF. Moreover, dual-calibrated fMRI is relatively insensitive to variability in PaO2,rest and PaO2,HO and extremely sensitive to errors in CBF measurements, especially in the hyperoxia state.
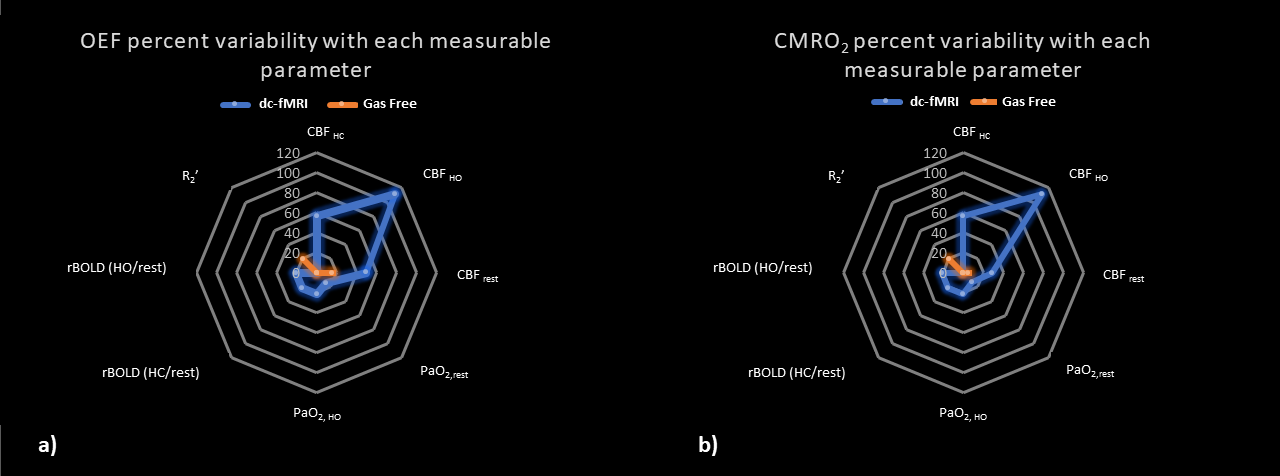
The sensitivity of OEF and CMRO2 estimates to 10% variation in each of the input parameters is illustrated by radar plots in Fig. 4a and 4b, respectively. In general, gas-free calibrated fMRI has better precision performance than dual-calibrated fMRI. For dual-calibrated fMRI, the hyperoxic CBF is the largest driver of OEF and CMRO2 estimation variability.
Discussion
The simulation results show that measurement of baseline OEF and CMRO2 by gas-free calibrated and dual-calibrated fMRI have different sensitivities to the same degree of variability in their measurable inputs. These variabilities can be as high as 110%, like parameter as CBFHO on both baseline OEF and CMRO2 measurements with dual-calibrated fMRI. Our results show that gas-free calibrated fMRI measurements of CMRO2 and OEF are associated with far lower variability than the dual-calibrated fMRI, potentially because the gas-free model is more linearly dependent on the inputs. However, the gas-free calibrated model heavily depends on using R2’ to estimate venous deoxygenated hemoglobin concentration (dHb) variation. However, dHb estimation purely through R2’ may not be correct in the in-vivo brain because of such confounds as partial-volume effects of cerebrospinal fluid (CSF)9 and ferritin deposition10. For example, previous gas-free calibrated studies report higher averaged R2’ than assumed in this simulation, which could lead to overestimating OEF11,12. Thus, the low sensitivity of gas-free calibrated fMRI does not necessarily translate into higher accuracy.Conclusion
In this study, we use simulations to compare the intrinsic uncertainties of gas-free calibrated and dual-calibrated fMRI for estimating CMRO2 and OEF, for a given variability to each of their measurable input parameters. We show that gas-free calibrated fMRI is substantially less sensitive to measurement variability. Limitations of our approach include: (1) we do not incorporate realistic variability in the input measurements (which will depend on the choice of technique, subject motion, field strength, scanner platform, etc); (2) we do not account for measurement error due to fundamental limitations in the models. Future research to analyze the natural variability of each measurement and how they may influence the choice between different approaches for cerebral metabolism measurements.Acknowledgements
The authors acknowledge funding support from the Canadian Institutes of Health Research (CIHR) and the Natural Sciences and Engineering Research Council of Canada (NSERC).References
1. Pike, G. B. Quantitative functional MRI: concepts, issues and future challenges. Neuroimage 62, 1234–1240 (2012).
2. Qin, Q., Grgac, K. & Van Zijl, P. C. M. Determination of whole-brain oxygen extraction fractions by fast measurement of blood T2 in the jugular vein. Magn. Reson. Med. 65, 471–479 (2011).
3. Chen, J. J., Uthayakumar, B. & Hyder, F. Mapping oxidative metabolism in the human brain with calibrated fMRI in health and disease. J. Cereb. Blood Flow Metab. 42, 1139–1162 (2022).
4. Gauthier, C. J. & Hoge, R. D. A generalized procedure for calibrated MRI incorporating hyperoxia and hypercapnia. Hum. Brain Mapp. 34, 1053–1069 (2013).
5. Hirsch, N. M. et al. Technical considerations on the validity of blood oxygenation level-dependent-based MR assessment of vascular deoxygenation. NMR Biomed. 27, 853–862 (2014).
6. An, H. & Lin, W. Cerebral venous and arterial blood volumes can be estimated separately in humans using magnetic resonance imaging. Magn. Reson. Med. 48, 583–588 (2002).
7. Zhang, J. et al. Cerebral metabolic rate of oxygen (CMRO2 ) mapping with hyperventilation challenge using quantitative susceptibility mapping (QSM). Magn. Reson. Med. 77, 1762–1773 (2017).
8. Göttler, J. et al. Flow-metabolism uncoupling in patients with asymptomatic unilateral carotid artery stenosis assessed by multi-modal magnetic resonance imaging. J. Cereb. Blood Flow Metab. 39, 2132–2143 (2019).
9. Simon, A. B., Dubowitz, D. J., Blockley, N. P. & Buxton, R. B. A novel Bayesian approach to accounting for uncertainty in fMRI-derived estimates of cerebral oxygen metabolism fluctuations. Neuroimage 129, 198–213 (2016).
10. Blockley, N. P., Griffeth, V. E. M., Simon, A. B. & Buxton, R. B. A review of calibrated blood oxygenation level-dependent (BOLD) methods for the measurement of task-induced changes in brain oxygen metabolism. NMR Biomed. 26, 987–1003 (2013).
11. Hirsch, N. M. et al. Technical considerations on the validity of blood oxygenation level-dependent-based MR assessment of vascular deoxygenation. NMR Biomed. 27, 853–862 (2014).
12. Göttler, J. et al. Flow-metabolism uncoupling in patients with asymptomatic unilateral carotid artery stenosis assessed by multi-modal magnetic resonance imaging. J. Cereb. Blood Flow Metab. 39, 2132–2143 (2019).
Figures