4012
The diagnostic value of multi-parameter CMR for early detection of light-chain amyloidosis from hypertension cardiomyopathy patients
Fang Wang1, Lili Yang1, Yanbin Yang1, Xiaowei Ruan1, Rui Wang1, and Xiuzheng Yue2
1Peoples hospital of ningxia hui autonomous region, Yinchuan, China, 2Philips Healthcare, Beijing, China, Beijing, China
1Peoples hospital of ningxia hui autonomous region, Yinchuan, China, 2Philips Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Cardiomyopathy, Cardiomyopathy, CMR, light chain amyloidosis, hypertension cardiomyopathy
The value of cardiac magnetic resonance imaging in diagnosing light chain amyloidosis has been confirmed, and its characteristic LGE manifestations are an important means to identify myocardial amyloidosis. However, early-stage light-chain amyloidosis patients always have the same symptoms as hypertensive cardiomyopathy in clinical practices. This study aimed to investigate the combined diagnostic efficacy of T1mapping, ECV, and myocardial strain techniques in early myocardial amyloidosis by comparing with healthy controls and patients with hypertensive cardiomyopathy that also caused uniform myocardial thickening.Introduction
The value of cardiac magnetic resonance imaging in diagnosing light chain amyloidosis has been confirmed, and its characteristic LGE manifestations are an important means to identify myocardial amyloidosis. However, its clinical application is limited for patients with contraindications to using contrast agents. At the same time, because a single LGE sign is not highly sensitive in diagnosing patients with early myocardial involvement, it is prone to misdiagnosis and misdiagnosis. This study aimed to investigate the combined diagnostic efficacy of T1mapping, ECV, and myocardial strain techniques in early myocardial amyloidosis by comparing with healthy controls and patients with hypertensive cardiomyopathy that also caused uniform myocardial thickening.Methods
Thirty-eight AL CA patients, fourteen HHM patients, and seventeen HA people were prospectively recruited. All subjects underwent LGE imaging, Cine images, and T1 mapping on a 3T scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) equipped with a 16-element phased-array torso-cardiac coil. All subjects have consented to participate in this study. The LV LGE pattern was recorded as none, patchy or global. LV strain, native T1, and ECV were measured semi-automatically using dedicated CMR software. According to their clinical and biochemical markers, all patients were classified as Mayo I/II and Mayo IIIa/IIIb. Cardiac structure, function, ECV mapping, and myocardial deformation were measured semi-automatically using dedicated CMR software (cvi42, version 5.3, Circle Cardiovascular Imaging, Calgary, Canada). Correlations between continuous variables, such as T1mapping, GLS, etc., or categorical variables, such as Mayo stage, were assessed using Pearson's correlation or Spearman's p-correlation. A P value < 0.05 was statistically significant.Results
For patients with Mayo stage I/II AL CA, the absolute value of global longitudinal strain (GLS) (11.2±3.3 vs. 9.7±3.1, P<0.05), the absolute value of global circumferential strain (GCS) (19.0 ±3.6 vs. 14.4±4.4, P<0.001) higher than that of HHD patients. In particular, the T1 (1334.9±49.9ms vs. 1269.9±38.4ms, P<0.0001) and ECV values (37.8±5.7% vs. 31.2±3.5%, P<0.0001) of the native were higher than those of the HHD patients. The detailed characteristics and CMR parameters of Health control, HHD, and AL CA patients are shown in Tabel 1 and Table 2.Examples of short axis-and four-chamber LGE images, strain parameters, native T1, and ECV values from a healthy control subject, an HHD patient, and AL CA patients with different Mayo stages are shown in FIGURE 1.Discussion
In this study, we found that GCS, GLS, and T1 values combined with ECV can effectively improve the detection rate of Mayo I/II AL CA patients from HHD patients. Both LGE and T1 mapping can assess myocardial fibrosis, but T1 mapping is more sensitive. It can identify early myocardial fiber replacement in Mayo I/II AL CA patients. The results of this study show that the T1 mapping value combined with ECV can be used for the differential diagnosis of Mayo staging. At the same time, it was confirmed that the T1mapping value and ECV value of hypertensive patients were mostly in the normal range, while the left ventricular long axis and circumferential strain rate decreased more significantly This may be related to the compensatory hypertrophy of the myocardium in patients with hypertension and the early hypertrophy of myocardial cell contractility, which can be used for the identification of early myocardial amyloidosis and hypertensive cardiomyopathy.Conclusion
Native-T1, ECV value, and longitudinal strain could detect early CA patients from HHD patients. They have important clinical implications as they have the potential to be an alternative to early and appropriate diagnosis of cardiac involvement, with timely initiation of targeted therapy.Acknowledgements
NoneReferences
1. Palladini, G. et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: Impact on survival outcomes. J. Clin. Oncol. 30(36), 4541–4549 (2012).Jung, H. N. et al. Comparison of tissue tracking assessment by cardiovascular magnetic resonance for cardiac amyloidosis and hypertrophic cardiomyopathy. Acta Radiol. 61, 284185119883714 (2019).Figures
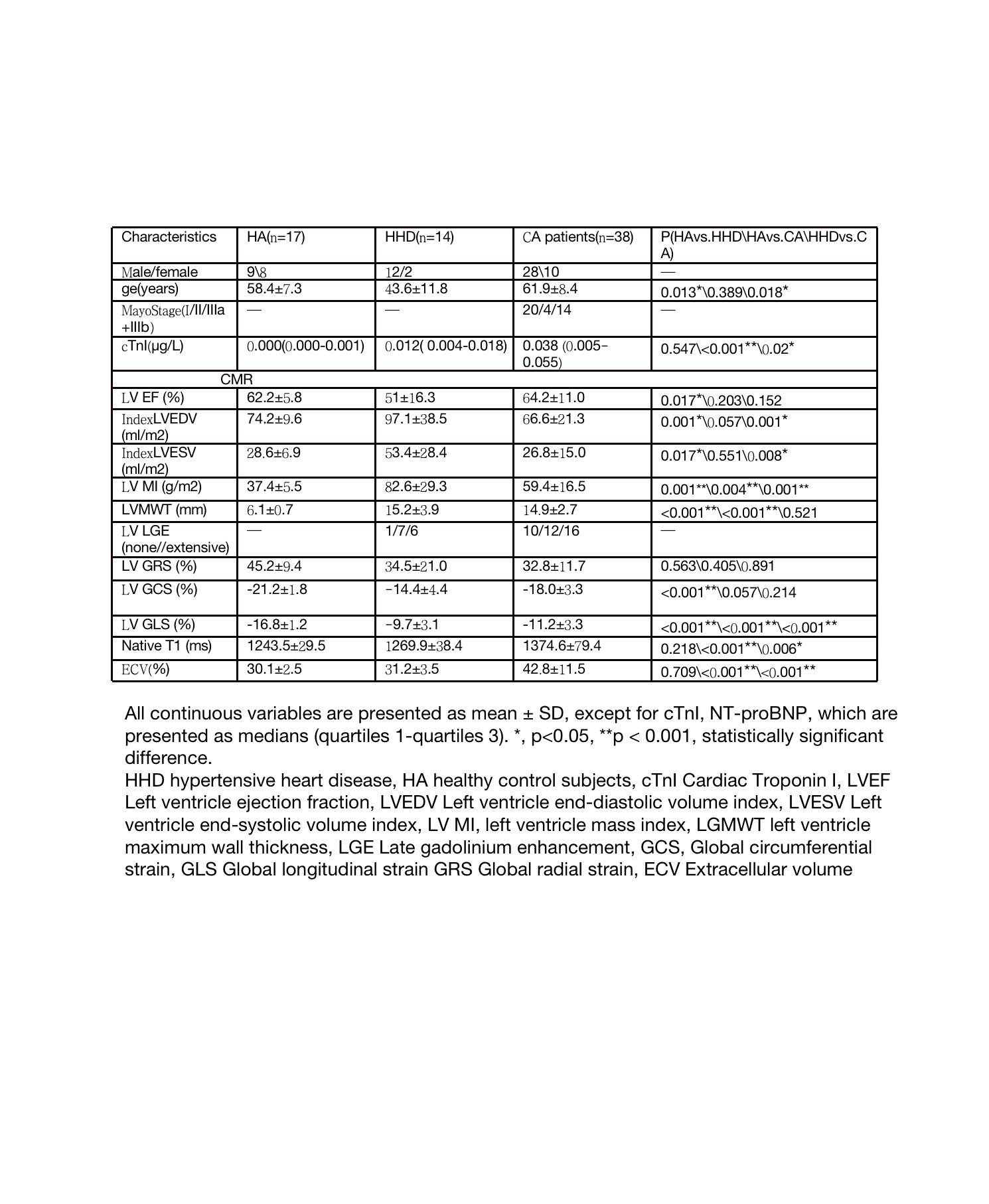
Table 1 Baseline characteristics of the healthy control, HHD patients, and CA AL patients
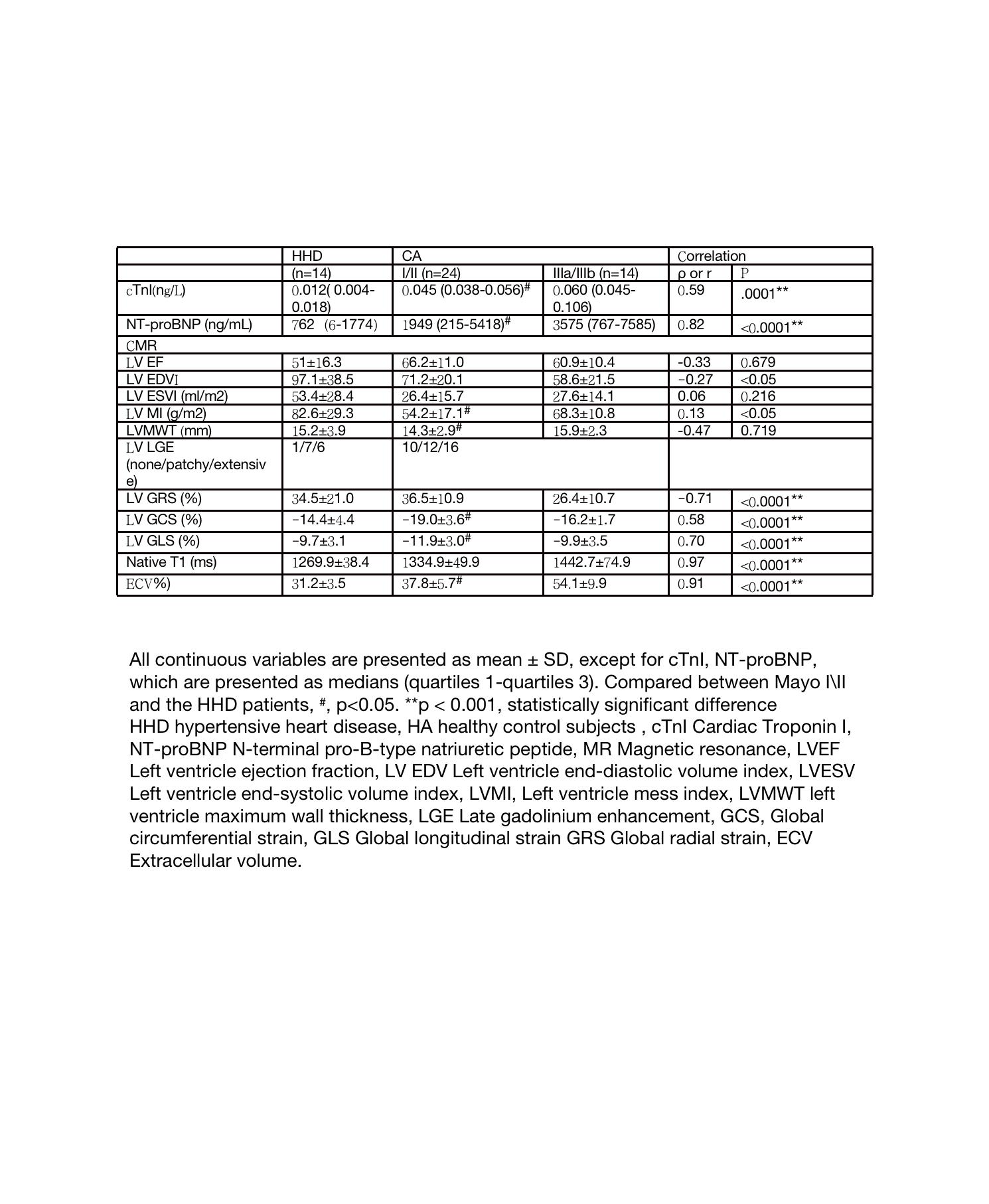
Table2 Clinical and CMR parameters correlation with hypertensive heart disease patient and clinical stage in AL amyloidosis patients
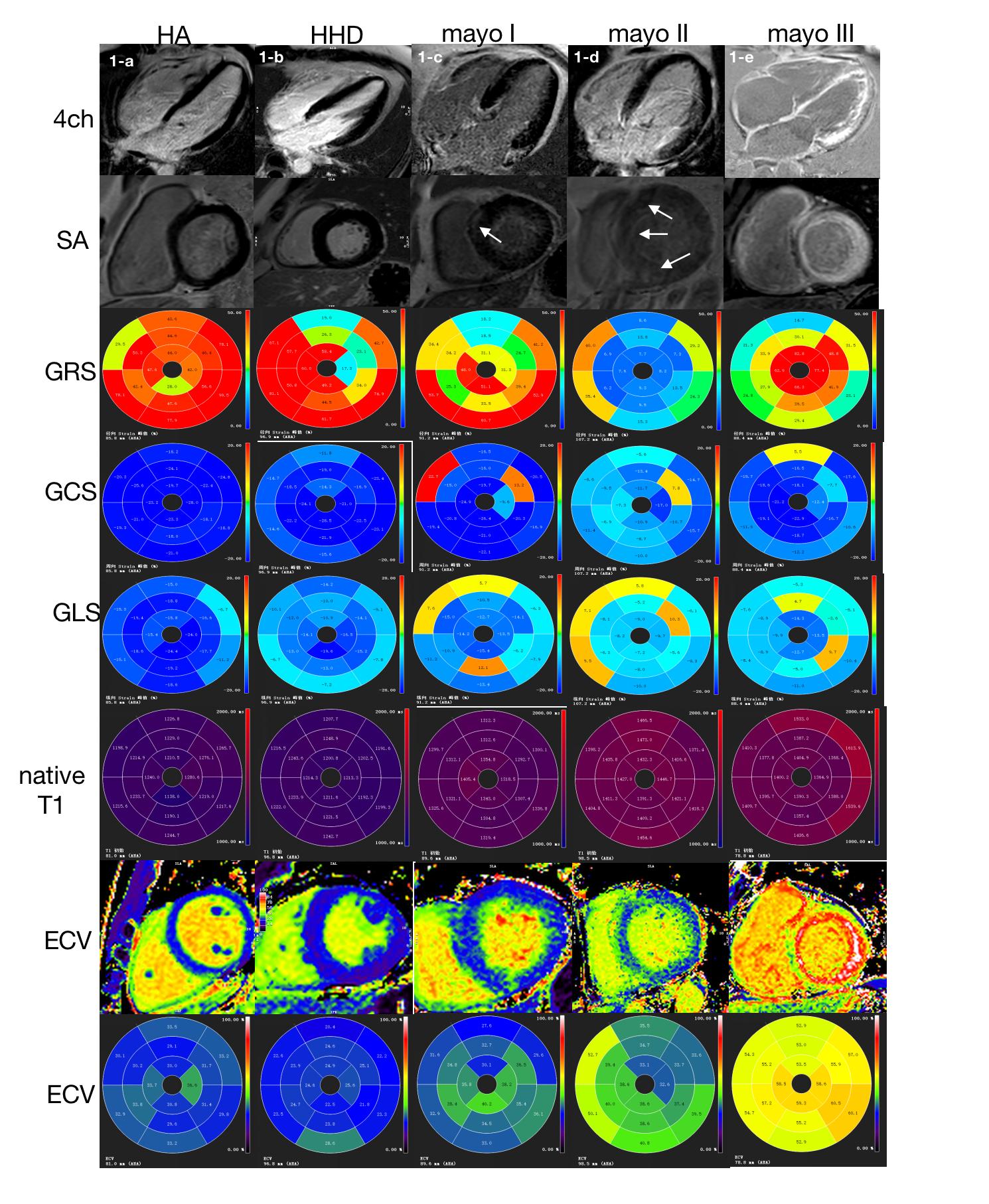
Fig.1 Four-chamber and SA LGE images, LV strain values, ECV pseudo-color images, Native T1 and ECV bull’s eye plots of AL amyloid patients and hypertensive heart disease and healthy control subjects.
DOI: https://doi.org/10.58530/2023/4012