4001
Whole-heart simultaneous CINE T2mapping and coronary MR angiography
Kazuo Kodaira1, Masami Yoneyama2, Michinobu Nagao3, Mana Kato1, Takumi Ogawa1, Yutaka Hamatani1, Isao Shiina1, Yasuhiro Goto1, and Shuji Sakai3
1Department of Radiological Services, Tokyo Women's Medical University, Tokyo, Japan, 2Philips Japan, Tokyo, Japan, 3Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan
1Department of Radiological Services, Tokyo Women's Medical University, Tokyo, Japan, 2Philips Japan, Tokyo, Japan, 3Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan
Synopsis
Keywords: Myocardium, Quantitative Susceptibility mapping
T2mapping is generally obtained only in diastole. However, because myocardial edema can affect both diastole and systole, acquisition of T2mapping of different cardiac phases is desirable. In addition, CMRA is also necessary in post-MI. However, scanning all these sequences prolongs exam time and increases patient stress. To overcome this limitation, we report a new T2mapping technique that enables quantitative systolic and diastolic T2mapping and CMRA acquisition in one scan by using dynamic trigger delay. In this study, we demonstrate the feasibility of this approach in healthy volunteer examination.Introduction
Quantitative myocardial-T2mapping is useful in diagnosis of heart diseases such as diffuse myocardial-edema1-3. Since current procedure is basically acquired during diastolic-phase, T2mapping has district information only. However, it is clinically known that myocardial-edema thereafter myocardial-infarction (MI) can affect both the diastolic and systolic function4. Thus, acquisition of T2mapping in different cardiac-phases (diastolic and systolic, at least), would be clinically desired to further accurately assess the diffuse myocardial pathologies. 3D isotropic whole-heart diastolic and systolic myocardial T2mapping that has recently been introduced could provide diastolic and systolic myocardial T2mapping within clinically acceptable scan time5. However, to obtain both diastolic and systolic T2mapping, two separate scans were required, which lead to image datasets misalignment due to possible motion between the scans. We hypothesized that diastolic and systolic can be acquired simultaneously by acquiring T2maps with variable trigger delay time in one single scan. On the other hand, the framework of previously introduced 3D isotropic whole-heart diastolic and systolic myocardial T2mapping sequence was based on navigator-gated, fat-suppressed, T2-prepared 3D turbo-field-echo sequence, which is identical to typical whole-heart coronary-MRA (CMRA) sequence7. Hence, we also hypothesized that T2mapping and CMRA may be acquired simultaneously with this sequence by adjusting the exact trigger-delay (TD) at mid-diastole, optimal timing for coronary arteries. In this study, we propose a new whole-heart T2mapping and CMRA technique (3D-WH-CINE-T2mapping) that simultaneously acquires diastolic and systolic data like CINE-imaging by using dynamic-TD (DynTD), and also simultaneously acquires CMRA.Methods
A schematic overview of the sequence for 3D-WH-CINE-T2mapping is shown in Figure 1. T2mapping was performed using a T2-prepared segmented RF-spoiled gradient echo (T1 turbo-field-echo: T1TFE) sequence, similar to whole-heart CMRA sequence at 3T. Recently, a unique T1ρ-mapping approach using interleaved spin-lock prepared steady-state-free-precession pulse sequence has been proposed to achieve single breath-hold T1ρ-Mapping of heart6, which employs different spin-lock pulses alternately before each TFE-shots. We followed the same concept and replaced the spin-lock pulses by T2prep pulses. Furthermore, we applied 3D non-selective excitation pulses which was previously introduced as effective in CMRA on 3.0T7,8 and compressed-sensing-technique (Compressed-SENSE, C-SENSE) 9,10 to shorten scan time. For generating the T2map, four images with different T2-preparation times (TE=0, 27, 53 and 80ms) were acquired with interleaved acquisition at the respective heartbeats. T2-weighted image was obtained with navigator respiratory triggering. The repetition-time (TFE shot interval) was set to 2 heartbeats. In addition, to obtain different cardiac-phases, we applied DynTD technique. DynTD is combined with the dynamic scan procedure with variable TD among different dynamic scans, but the scan-parameters (including TR/TE/number of slices, etc.) of each dynamic scan are exactly same. TD is only increasing with the number of dynamic scans and TD-increments (ms/dyn) can be determined arbitrarily. Consequently, DynTD can acquire several different time-phase images in one scan. Systolic-timing was observed using CINE-image, and its timing was set as trigger-delay time. Also, the interval between systole and diastole was set to TD-increments. In this way, systolic and diastolic phases were targeted and acquired. Besides, to obtain CMRA, the resting time of coronary arteries was observed on CINE-image, and the time was set to shot-duration time. To minimize motion-induced misalignment, the across T2prep-TE images were registrated using fast-elastic-image-registration (FEIR)11 which can mitigate such variations of in-plane heart-shape by registering the source images before creation of the parametric-map12. The scan-parameters were optimized and 6 healthy volunteers were scanned (5-males and 1-female; age-range: 27~45) on a clinical 3.0T system (Ingenia, Philips Healthcare). T2 relaxation times were measured from the obtained T2mapping using 16-segment model13. Imaging-parameters for 3D-WH-CINE-T2mapping were; 3D non-selective T1TFE, Coronal acquisition, FOV=340×340mm, voxel-size=2.2×2.2×2.2mm, TR/TE=1.9/0.94ms, flip-angle=12, TFE-factor=52, TFE shot interval=2 heartbeats, C-SENSE factor=10, and acquisition time=5 to 8minutes (depend on the heart-rate and body-habitus).Results
Figure 2,3 shows representative source T2-prepared images of 3D-WH-CINE-T2mapping and short-axis (SA), two-chamber (2CH), and four-chamber (4CH) MPR images in diastole and systole. These images showed sufficient SNR and there were no obvious artifacts in the heart. Figure 4 shows the comparison between 2D multi-echo gradient spin-echo (mGraSE) and 3D-WH-CINE-T2mapping in SA (base). The measured T2 relaxation times from all volunteers were comparable to the literature findings14. Figure 5 shows representative source image (prepTE:53ms) of 3D-WH-CINE-T2mapping and CPR images of coronary artery.Discussion & Conclusion
We demonstrated the feasibility of 3D-WH-CINE-T2mapping to simultaneously acquire diastolic and systolic T2mapping and CMRA in one scan within clinically acceptable scan time. It could make simultaneous acquisition of diastolic and systolic T2 relaxation time more convenient and may provide more detailed diagnosis of the myocardial effects of myocardial edema. In addition, diagnosis of T2mapping with full LV coverage is desirable for accurate evaluation of myocardial area-at-risk after ischemic event4. Moreover, coronary artery diagnosis is clinical desiable for post-MI assessment. Because the proposed technique can acquire both of these images in clinically acceptable time, it may reduce the burden on the patient with post-MI. Although lower spatial resolution of current sequence is poor for diagnosing coronary artery yet, it can be improved with advanced deep-learning based AI-reconstruction. More systematic investigations are needed to study its clinical robustness and quantification precision in comparison to the conventional techniques.Acknowledgements
No acknowledgements found.References
1. Giri S, et al. T2 quantification for improved detection of myocardial edema. J Cardiovasc Magn Reson. 2009 Dec 30;11:56. 2. Sprinkart AM, et al. Gradient Spin Echo (GraSE) imaging for fast myocardial T2 mapping. J Cardiovasc Magn Reson 2015;17:12. 3. Fernández-Jiménez R, et al. Fast T2 gradient-spin-echo (T2-GraSE) mapping for myocardial edema quantification: first in vivo validation in a porcine model of ischemia/reperfusion. J Cardiovasc Magn Reson 2015;17:92. 4. Constantin-Cristian Topriceanu. et al. T2 and T2* mapping and weighted imaging in cardiac MRI. Magn Reson Imaging 2022 Nov 93:15-32 5. Masami yoneyama, et al. Rapid free-breathing 3D isotropic whole-heart diastolic and systolic myocardial T2mapping. Proc. ISMRM:2020.2061. 6. Van Oorschot JW, et al. Single Breath-Hold T1ρ-Mapping of the Heart for Endogenous Assessment of Myocardial Fibrosis. Invest Radiol. 2016 Aug;51(8):505-12. 7. Kodaira K, et al. Acceleration of whole-heart coronary MR angiography using 3D non-selective bSSFP with Compressed SENSE. Proc. ISMRM:2019.2063. 8. Shiina I, et al. Whole heart coronary MRA using non-selective balanced SSFP sequence at 3.0T: comparison of image quality. Proc. ISMRM:2019.2073. 9. Geerts-Ossevoort L, et al. Compressed SENSE Speed done right. Every time. The Netherlands: Philips Healthcare; 2018 Jan. Report No: 4522 991 31821. https://www.philips.de/content/dam/b2bhc/de/resourcecatalog/landingpages/ingeniaelition/White_Paper_Compressed_SENSE-opt.pdf 10. Sartoretti E, et al. Reduction of procedure times in routine clinical practice with Compressed SENSE magnetic resonance imaging technique. PLoS One. 2019 Apr 12;14(4):e0214887. doi: 10.1371/journal.pone.0214887. eCollection 2019. 11. Zhang S, et al. Cardiac magnetic resonance T1 and extracellular volume mapping with motion correction and co-registration based on fast elastic image registration. MAGMA. 2018 Feb;31(1):115-129. 12. Takumi ogawa, et al. Minimizing motion artifacts in myocardial quantitative mapping by combined use of motion-sensitive CINE imaging and FEIR. Proc. ISMRM:2021. 13. Manuel D Cerqueira, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002 Jan 29;105(4):539-42. doi: 10.1161/hc0402.102975. 14. Florian von Knobelsdorff-Brenkenhoff, et al. Myocardial T1 and T2 mapping at 3 T: reference values, influencing factors and implications. J Cardiovasc Magn Reson 2013;15(1):53.Figures
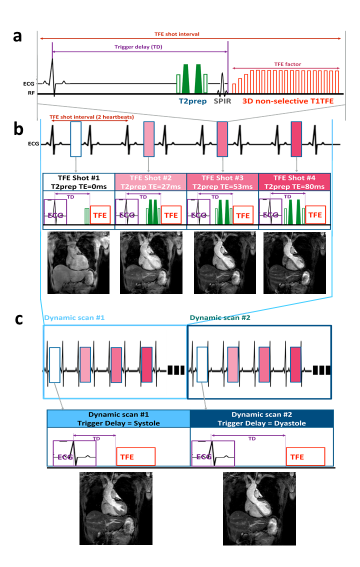
Figure 1: Scheme of the sequence for 3D whole heart CINE T2mapping.
T2map was
performed using T2prepared segmented turbo field echo
(TFE) sequence. 3D non-selective excitation pulses were applied to shorten
TR/TE which leads to increase TFE factor per 1 heartbeat (a). The numbers indicate 4 images
with different T2-preparation times (b).
Each
image was simultaneously obtained systole and diastole using dynamic trigger delay combines with dynamic scan procedure.
Dynamic scan #1 and #2 TDs were optionally
set to match systole and diastole timings obtained by observing CINE image (c).
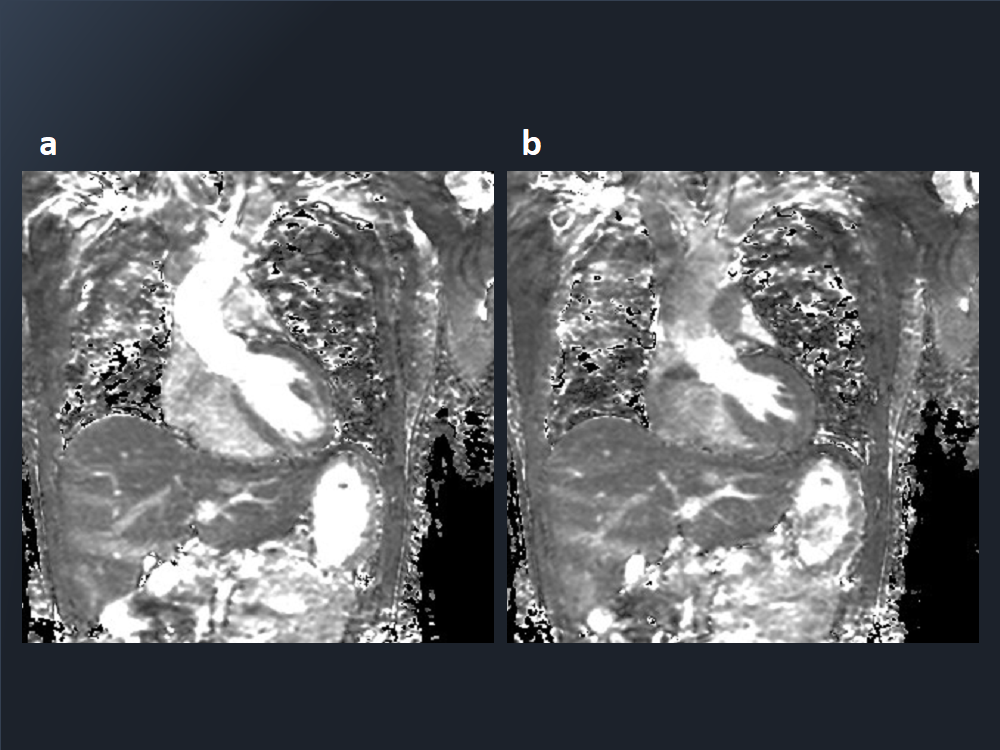
Figure 2: Representative source images
of myocardial 3D whole heart myocardial CINE T2mapping in diastole (a) and
systole (b).
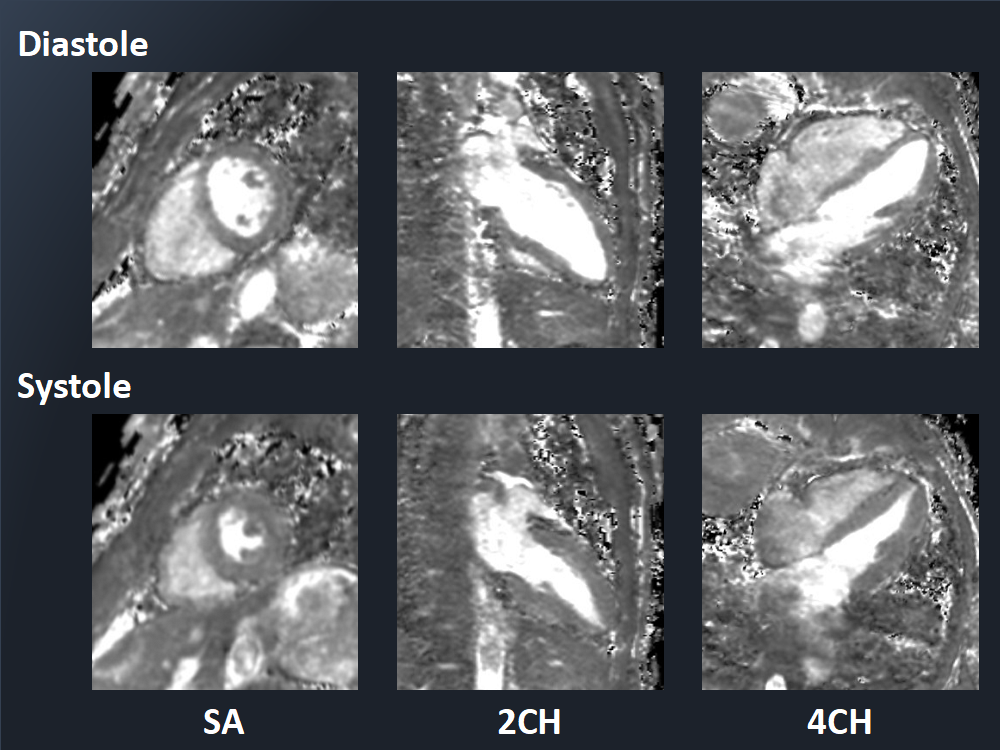
Figure 3: Representative short-axis
(SA), two-chamber (2CH), and four-chamber (4CH) MPR images of 3D whole heart
myocardial CINE T2mapping in diastole and systole.
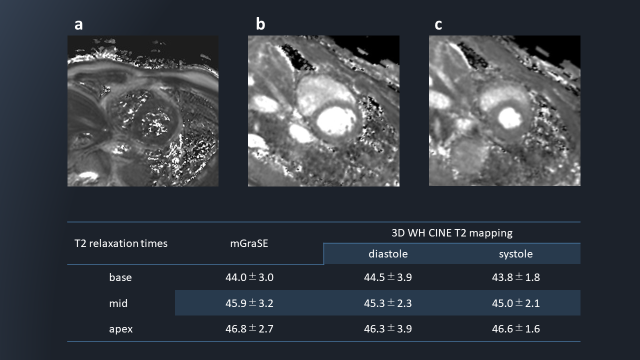
Figure 4: Comparison of short-axis
(SA) myocardial T2map with mGraSE at diastole (a) and SA MPR image of 3D whole heart myocardial CINE
T2mapping at diastole (b) and systole (c). The table shows the average T2
relaxation time for all volunteers in each sequence.
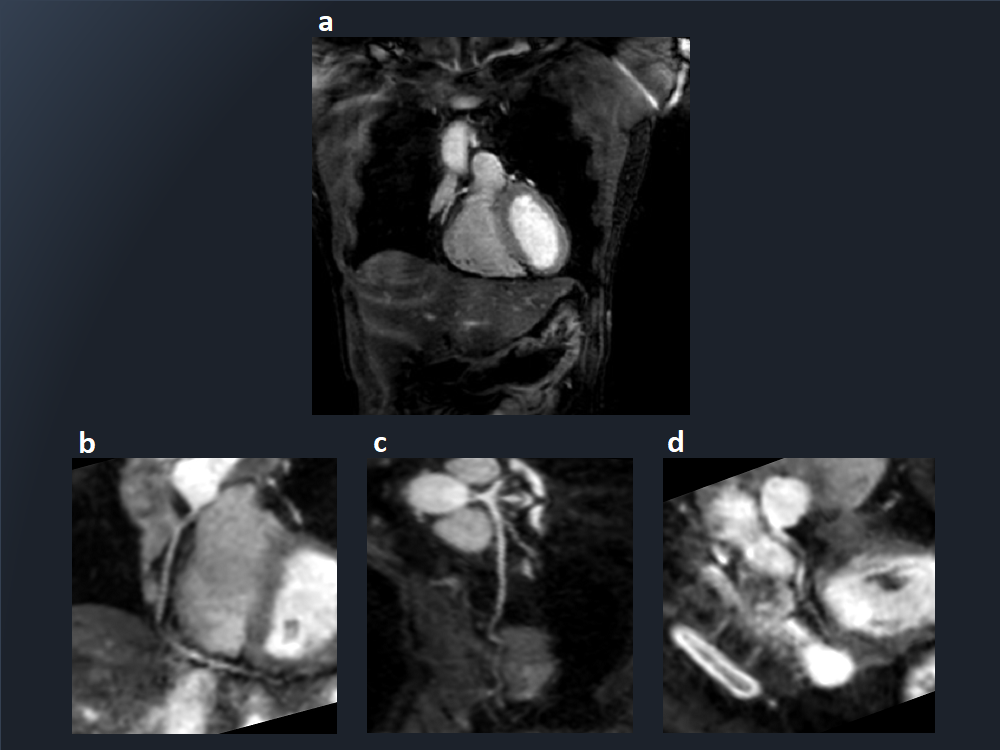
Figure 5: Representative
source image (prepTE:53ms) of 3D whole heart myocardial CINE T2mapping
(a) and RCA (b), LAD (c) and LCX (d) CPR images of coronary artery.
DOI: https://doi.org/10.58530/2023/4001