3988
Amide Proton Transfer MRI for Treatment Response of Locally Advanced Rectal Cancer Following Neoadjuvant Chemotherapy and Radiation Therapy1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Techonology, Wuhan, China, 2Philips Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Digestive, Cancer
We conducted this prospective study to determine whether APTw imaging is precise in evaluating treatment response of LARC after NCRT, by comparing the accuracy of evaluation using APTw imaging to that of T2-weighted imaging and DWI, which is value for the selection of organ preservation candidates.Introduction
For patients with locally advanced rectal cancer (LARC), neoadjuvant chemotherapy and radiation therapy (NCRT) is considered the standard treatment. NCRT has been shown to improve local control, inducing tumor downstaging in approximately 50% of patients, and results in pathologic complete response in 15%–38% of cases. This can allow for a sphincter-preserving surgery to be performed or may even offer a nonsurgical treatment approach in some patients. While precise evaluation of treatment response is the premise of the selection of the following treatment strategies. Since morphological details are insufficient and diffusion-weighted MR imaging appears to be controversial for better evaluating treatment response of LARC after NCRT, a new imaging biomarker to evaluate treatment response more accurately is desirable. Amide proton transfer-weighted (APTw) imaging is a molecular MRI technique that generates image contrast based predominantly on the amide protons in mobile cellular proteins and peptides that are endogenous in tissue, which have already shown potential application in diseases of central nervous system. Recently, several exploratory APT-related researches on rectal cancer are reported, while there has been no report on the diagnostic performance of APTw imaging in evaluating treatment response of LARC after NCRT. We thus conducted this prospective study to determine whether APTw imaging is precise in evaluating treatment response of LARC after NCRT. We compared the accuracy of evaluation by APTw imaging to that of T2-weighted imaging and DWI for the selection of organ preservation candidates.Methods
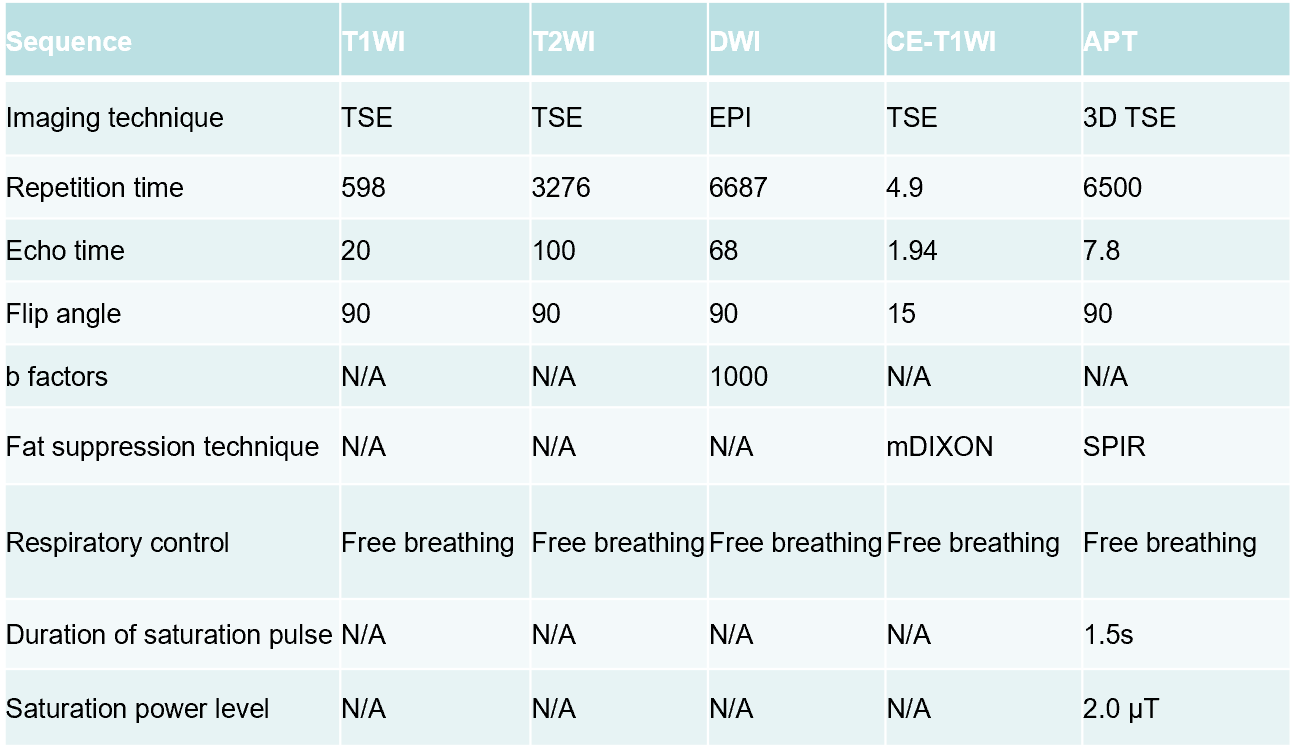
Patients with histological diagnostic rectal cancer and clinical T3-4 or N+ were recruited into this institutional review board-approved study. All participants were scanned at 3.0T (Ingenia, Philips Healthcare, Best, the Netherlands) using standard rectal protocols (T1WI, T2WI, DWI, contrast-enhanced) and APTw-imaging (acquired with 3D turbo-spin-echo sequence) at baseline and post-NRCT, imaging parameters listed in Table 1.NCRT was followed by total mesorectal excision surgery. The post-NCRT/preoperative MRI evaluation included yT stage, EMVI, and MRF. Readers evaluated yT stage on high-resolution T2-weighted imaging combined with high b value (b = 1000 sec/mm2) DWI. Two readers manually drew regions of interest (ROIs) on the APT maps by using a free and open software (3D slicer 5.0.3, NA-MIC, NAC, BIRN, NCIGT and the Slicer Community), and the ROIs should properly cover the rectal walls where the initial lesions were located with reference to the baseline T2-weighted images. APT parameters, including 10th percentile, mean, median, 90th percentile, SD, skewness and kurtosis, were extracted for histogram analysis from the ROIs.Two radiologists independently analyzed the MR data.Inter-observer agreement on APT values was analyzed using intraclass correlation coefficient (ICC) and k statistics. The grade of tumor response (TRG) to NCRT, classified into four categories, was extracted from hospital information system. To explore the feasibility of APT parameters in evaluating treatment response of LARC after NCRT, APT parameters of TRG0 tumors were compared with those of TRG123 tumors by using the independent sample t test or Mann-Whitney U test. The diagnostic performance of significant APT parameters for differentiating TRG0 from TRG123 tumors was assessed by using receiver operating characteristic (ROC) analysis with the area under the curve (AUC) to identify the optimal APT threshold by maximizing the sensitivity plus specificity. The significance of the threshold was re-evaluated by using chi square test. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of both T2DWI and the optimal thresholds of significant APT parameters were calculated. The ROC analysis was conducted for assessing the diagnostic performance of T2DWI too. The AUCs were compared by using the DeLong method.Results
A total of 34 patients were included.The mean APT were significantly lower in TRG0 tumors than in TRG1-3 tumors ( P=0.043), whereas APT 90th percentile, SD, kurtosis, and skewness showed no significant difference. The AUC of the APT mean in predicting TRG0 tumors was 0.73(95% CI: 0.60, 0.79), which was significantly higher than that of the T2DWI in predicting TRG0 tumors(0.66 95% CI: 0.55, 0.71).Discussion
Rectal cancer is usually very proliferative and possesses high considerable potential in long-distance metastases, which likely lead to an abundant pool of mobile cellular proteins and peptides. Post-NCRT, there are fibrosis, mucin and residual tumor in rectal wall of previous lesion. APTw imaging is a molecular MRI technique that generates image contrast based predominantly on the amide protons in mobile cellular proteins and peptides that are endogenous in tissue. Several exploratory APT-related researches on rectal cancer reported the relationship between APT value and pathological features. By comparing the accuracy of evaluation by APTw imaging to that of T2-weighted imaging and DWI ,we confirm the potential that APTw imaging is precise in evaluating treatment response of LARC after NCRT.Conclusion
We speculate that APT value may be a useful biomarker in evaluating treatment response of LARC after NCRT, which could have a potential impact on the clinical therapeutic strategies for patients, and this needs to be validated in a further study with larger sample size.Acknowledgements
No acknowledgement found.References
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Rectal Cancer version 2.2017.https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed December 15, 2017.
2. Kim SH, Lee JY, Lee JM, Han JK, Choi BI. Apparent diffusion coefficient for evaluating tumor response to neoadjuvant chemoradiation therapy for locally advanced rectal cancer. Eur. Radiol. 2011; 21: 987–95.
3. Zhou J, Payen JF, Wilson DA, Traystman RJ, van Zijl PCM. Using the amide proton signals of intracellular proteins and peptides to detect pH effects in MRI. Nat Med 2003; doi: 10.1038/nm907.
4. Nishie A, Takayama Y, Asayama Y, Ishigami K, Ushijima Y, Okamoto D, Fujita N, Tsurumaru D, Togao O, Sagiyama K, Manabe T, Oki E, Kubo Y, Hida T, Hirahashi-Fujiwara M, Keupp J, Honda H. Amide proton transfer imaging can predict tumor grade in rectal cancer2018;51:96-103.
5. Nishie A, Asayama Y, Ishigami K, Ushijima Y, Takayama Y, Okamoto D, Fujita N, Tsurumaru D, Togao O, Sagiyama K, Manabe T, Oki E, Kubo Y, Hida T, Hirahashi-Fujiwara M, Keupp J, Honda H. Amide proton transfer imaging to predict tumor response to neoadjuvant chemotherapy in locally advanced rectal cancer. Journal of Gastroenterology and Hepatology 2019;34 :140–146.
6. He YL, Li Y, Lin CY, et al. Three-dimensional turbo-spin-echo amide proton transfer-weighted MRI for cervical cancer: a preliminary study. J Magn Reson Imaging 2019; doi: 10.1002/jmri.26710
7. Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386.
8. Yang, Y.; Huang, X.; Sun, J.; Gao, P.; Song, Y.; Chen, X.; Zhao, J.; Wang, Z. Prognostic value of perineural invasion in colorectal cancer: A meta-analysis. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2015, 19, 1113–1122.
Figures