3976
MR Elastography Distinguishes Between Adrenal Adenomas and Malignomas by Increased Stiffness1Department of Radiology, Charité - Universitaetsmedizin Berlin, Germany, Berlin, Germany, 2Department of Surgery, Charité - Universitaetsmedizin Berlin, Germany, Berlin, Germany
Synopsis
Keywords: Endocrine, Elastography, Adrenal Gland, Multifrequency magnetic resonance elastography, Adrenal stiffness, Shear wave speed, Viscoelasticity
The ability to distinguish a benign from a malignant adrenal mass based on magnetic resonance imaging relaxation times is severely limited. For the first time at all, this study adrenal gland stiffness was investigated by using magnetic resonance elastography in healthy controls and participants with adrenal adenoma and malignoma. In healthy controls MRE was highly reproducible. Adrenal adenoma and malignoma are stiffer than healthy controls and both could be distinguished by an excellent diagnostic performance (AUC 0.8–1.0). MRE is promising non-invasive biomarker for clinically difficult differentiation of a malignancy and could prevent surgical overtreatment in the future.
Introduction
The adrenal gland as an endocrine gland is involved in the biosynthesis and secretion of steroid hormones and catecholamines(1, 2). Adrenal masses are occasionally discovered during routine examinations, commonly known as incidentalomas. Adrenal malignomas are rare tumors with a variable prognosis. The major challenge during clinical routine magnetic resonance imaging (MRI) examinations is the differentiation between benign and malignant adrenal tumors. Postoperative histopathology, with an invasive biopsy, remains the ultimate tool for differentiation between benign and malign tumors(2). An invasive biopsy can only be performed if an adrenal metastasis is suspected. In adrenal carcinoma a preoperative biopsy is forbidden, as it can lead to tumor spillage. High-resolution MR elastography (MRE) has been able to detect abdominal tumors based on changes in viscoelasticity(3-7). The hypothesis of this study is that adrenal adenoma and malignoma are stiffer than healthy adrenal glands, which could be detected by MRE. The purpose of this study is i) to establish multifrequency MRE for characterization of viscoelasticity of healthy adrenal glands and ii) to detect changes in benign and malignant adrenal tumors by altered stiffness.Methods
This prospective study includes 15 healthy volunteers (CTR) and 23 participants with adrenal masses suspicious for malignoma and clinical indication for adrenal resection. All adrenal masses were operatively resected and analyzed histopathologically. All subjects were examined by multifrequency MRE with tomoelastography postprocessing at 3 T with a 12-channel phased-array surface coil. Two posterior and two anterior actors were used to induct mechanic vibrations at harmonic frequencies of 30, 40, 50 and 60 Hz providing shear wave speed (SWS) in m/s as a surrogate for soft tissue stiffness(8, 9).Reproducibility was imparted in a subgroup of eleven healthy volunteers by performing two consecutive examinations with identical set-up and analysis of the intraclass correlation coefficient (ICC). Differences between CTR, adenoma and malignoma were calculated by Mann-Whitney test. Cutoffs and ROC-AUC analysis were computed to test diagnostic performances of MRE for detection of tumors.
Results
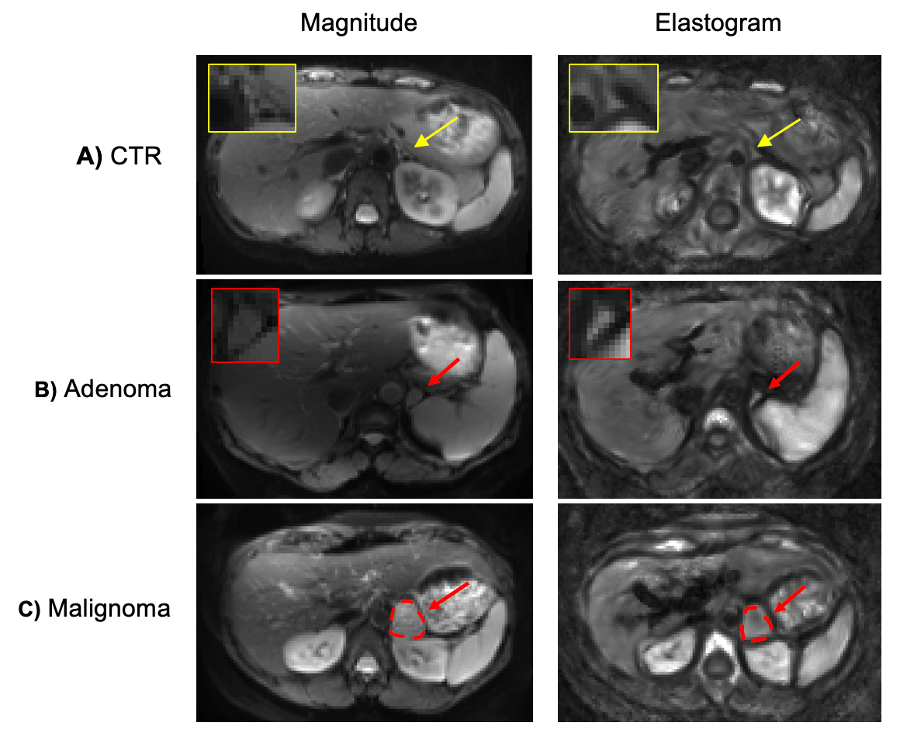
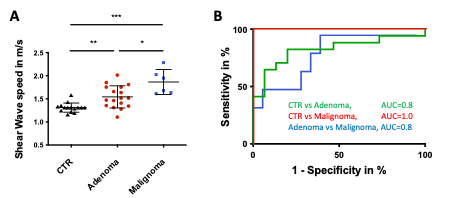
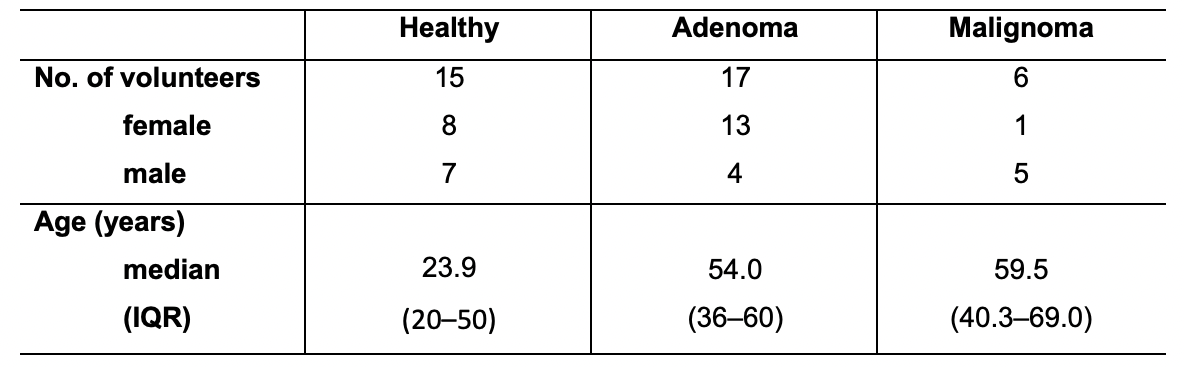
Multifrequency MRE was feasible in all subjects (100 % success rate). Of all adrenal masses, 17 adenomas and 6 malignomas were identified. The malignant cohort includes two adrenocortical carcinomas, two adrenal metastasis, and two high-risk pheochromocytomas. Study subject characteristics are displayed in table 1. Examples of CTR, adrenal adenoma, and malignoma are given in figure 1. An excellent reproducibility was calculated by an ICC of 0.84, see Bland-Altmann plot in figure 2. Compared to CTR (median SWS [interquartile range]; 1.31 [1.25–1.33] m/s) adenoma (1.52 [1.35–1.75] m/s) and malignoma (1.82 [1.63–2.09] m/s) showed a higher SWS with excellent AUCs of 0.8 and 1.0 with best cutoffs of 1.34 ms (sensitivity/specificity, 82 % / 80 %) and 1.59 m/s (100 % / 100 %) were calculated. Adenoma and malignoma were distinguished by a very good AUC of 0.8 with best cutoffs of 1.9 ms (sensitivity/specificity, 50 % / 94 %), see figure 3.Discussion
To the best of our knowledge, this is the first study that analyzed tissue stiffness in adrenal glands measured by in-vivo MRE. The detail resolution in the SWS maps generated by multifrequency MRE was high enough to reveal the adrenal gland with embedded tumors to the naked eye. The proposed MRE technique was highly reproducible and provided an excellent diagnostic accuracy for detection of adrenal adenoma and malignoma (AUC 0.8–1.0).Overactive adrenal glands are associated with increased metabolism and cell hypertrophy, reflected macroscopically by increased stiffness. Stiffness changes might be attributed to remodeling of extracellular matrix through cancer-associated fibroblasts in tumors(10). Currently, adrenal masses are subject to extensive endocrinological tests and histopathological examinations to determine functional disorders(2). However, these tests and standard imaging methods could not provide a sufficient determination of malignant adrenal lesions, which results in surgical overtreatment of benign masses(11).
In literature, only one study based on ultrasound elastography showed that benign tumors in the adrenal gland are stiffer than unaffected adrenal glands(14). In accordance with our results, the authors confirmed that diseased adrenal glands are stiffer than healthy adrenal glands. However, ultrasound elastography suffers from a low maximum penetration depth of 6 cm which limits its widespread clinical use for tumor detection in the adrenal gland.
The major limitation of our study was the relatively small sample size, which is due to the low prevalence of adrenal malignoma.
Conclusion
Multifrequency MRE provides non-invasive high-resolution elastograms for quantification of small organs as the adrenal glands and enables an excellent differentiation between healthy adrenal glands, benign and malignant tumors by detection of stiffness changes. MRE has a great potential as a novel biomarker for the, so far, challenging differentiation of a malignant adrenal mass by non-invasive imaging. In the future, MRE could reduce surgical overtreatment and support therapeutic decisions.Acknowledgements
No acknowledgement found.References
1. Avisse C, Marcus C, Patey M, Ladam-Marcus V, Delattre JF, Flament JB. Surgical anatomy and embryology of the adrenal glands. Surg Clin North Am. 2000;80(1):403-15.
2. Torti JF, Correa R. Adrenal Cancer. StatPearls. Treasure Island (FL)2022.
3. Shahryari M, Tzschatzsch H, Guo J, Marticorena Garcia SR, Boning G, Fehrenbach U, et al. Tomoelastography Distinguishes Noninvasively between Benign and Malignant Liver Lesions. Cancer Res. 2019;79(22):5704-10.
4. Zhu L, Guo J, Jin Z, Xue H, Dai M, Zhang W, et al. Distinguishing pancreatic cancer and autoimmune pancreatitis with in vivo tomoelastography. Eur Radiol. 2021;31(5):3366-74.
5. Marticorena Garcia SR, Zhu L, Gultekin E, Schmuck R, Burkhardt C, Bahra M, et al. Tomoelastography for Measurement of Tumor Volume Related to Tissue Stiffness in Pancreatic Ductal Adenocarcinomas. Invest Radiol. 2020;55(12):769-74.
6. Meyer T, Marticorena Garcia S, Tzschatzsch H, Herthum H, Shahryari M, Stencel L, et al. Comparison of inversion methods in MR elastography: An open-access pipeline for processing multifrequency shear-wave data and demonstration in a phantom, human kidneys, and brain. Magn Reson Med. 2022;88(4):1840-50.
7. Gultekin E, Wetz C, Braun J, Geisel D, Furth C, Hamm B, et al. Added Value of Tomoelastography for Characterization of Pancreatic Neuroendocrine Tumor Aggressiveness Based on Stiffness. Cancers (Basel). 2021;13(20).
8. Marticorena Garcia SR, Grossmann M, Lang ST, Tzschatzsch H, Dittmann F, Hamm B, et al. Tomoelastography of the native kidney: Regional variation and physiological effects on in vivo renal stiffness. Magn Reson Med. 2018;79(4):2126-34.
9. Tzschatzsch H, Guo J, Dittmann F, Hirsch S, Barnhill E, Johrens K, et al. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal. 2016;30:1-10.
10. Najafi M, Farhood B, Mortezaee K. Extracellular matrix (ECM) stiffness and degradation as cancer drivers. J Cell Biochem. 2019;120(3):2782-90.
11. Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1-G34.
12. Dittmann F, Tzschatzsch H, Hirsch S, Barnhill E, Braun J, Sack I, et al. Tomoelastography of the abdomen: Tissue mechanical properties of the liver, spleen, kidney, and pancreas from single MR elastography scans at different hydration states. Magn Reson Med. 2017;78(3):976-83.
13. Streitberger KJ, Guo J, Tzschatzsch H, Hirsch S, Fischer T, Braun J, et al. High-resolution mechanical imaging of the kidney. J Biomech. 2014;47(3):639-44.
14. Slapa RZ, Kasperlik-Zaluska AA, Migda B, Jakubowski WS. Shear wave elastography of adrenal masses is feasible and may help to differentiate between solid and cystic lesions - an initial report. Endokrynol Pol. 2014;65(2):119-24.
Figures