3974
Abnormal functional connectivity of the hippocampus and amygdala in plateau Tibetan with type 2 diabetes mellitus1Department of Radiology, Hospital of Chengdu Office of People’s Government of Tibetan Autonomous Region (Hospital. C.T.), Chengdu, Sichuan, China, 2Huaxi MR Research Center (HMRRC), Functional and Molecular Imaging Key Laboratory of Sichuan Province, Department of Radiology, West China Hospital, Sichuan University, Chengdu, Sichuan, China, 3Psychoradiology Research Unit of the Chinese Academy of Medical Sciences, West China Hospital of Sichuan University, Chengdu, Sichuan, China, 4Department of Endocrinology and Metabolism, Hospital of Chengdu Office of People’s Government of Tibetan Autonomous Region (Hospital. C.T.), Chengdu, Sichuan, China
Synopsis
Keywords: Endocrine, Diabetes
We performed a seed-based rsFC study to explore the hippocampus and the amygdala FC patterns in plateau Tibetan patients with T2DM. We found that, compared to plateau Tibetan HC, T2DM showed both increased rsFC between the right hippocampus and left DLPFC and left SFG, and between the left amygdala and right OFC as well as right DLPFC.Moreover, these rsFC abnormalities were significantly correlated with age, RBC and changes of visuospatial memory function in plateau Tibetan patients with T2DM. These findings of altered FC may provide important insights into the neural basis of diabetes-related cognitive decline in plateau Tibetan.Background
Type 2 diabetes mellitus (T2DM) accounts for 90-95% of diabetic patients, affects approximately 450 million adults worldwide, and increases the risk for cognitive decline and dementia[1]. It is reported that China has the largest number of patients with diabetes and spending the second highest amount on diabetes and its complications worldwide in 2013, among them the Tibetan population has the second highest incidence[2]. Several lines of evidence from structural and functional neuroimaging studies have reinforced the crucial role of the hippocampus and the amygdala in the pathophysiology of T2DM[3]. However, the mechanism how type 2 diabetes affects brain function in the hippocampus and amygdala in Tibetan plateau patients has not been fully elucidated. Thus, we hypothesized that there is a wide range of functional connectivity (FC) abnormalities between the hippocampus, amygdala and the whole brain in plateau Tibetan T2DM and that these abnormalities are correlated with cognitive function deficits.Materials and Methods
We recruited 87 plateau Tibetan T2DM patients and 63 plateau Tibetan healthy control subjects (HCs). We assessed their demographic and clinical data (weight, height, blood pressure, body mass index (BMI), plasma glucose, blood lipidand complete blood count (CBC)) and cognitive performance (living quality, anxiety and depressive symptoms, general cognitive function, processing speed, logical memory and visuospatial memory). All participants were scanned using a 3.0 T MRI scanner (Philips Achieva) with an 8-channel phased-head coil to acquire resting-state functional MR images and T1-weighted anatomical images.The preprocessing of resting-state functional images was performed using the pipeline of DPARSF. Seed-based FC analysis was used to map the FC pattern for the hippocampus and amygdala. We compared the differences in FC pattern of hippocampus and amygdala between plateau Tibetan T2DM patients and healthy controls using a multivariate analysis of covariance (MANCOVA) with age, sex and head motion as covariates. The significance threshold was set to p < 0.005 at the voxel level and the family-wise error (FWE) correction (p < 0.05) at the cluster level. Then, partial correlation analyses were conducted to investigate the association of hippocampus and amygdala FC abnormalities with biometric and neuropsychological measures.
Results
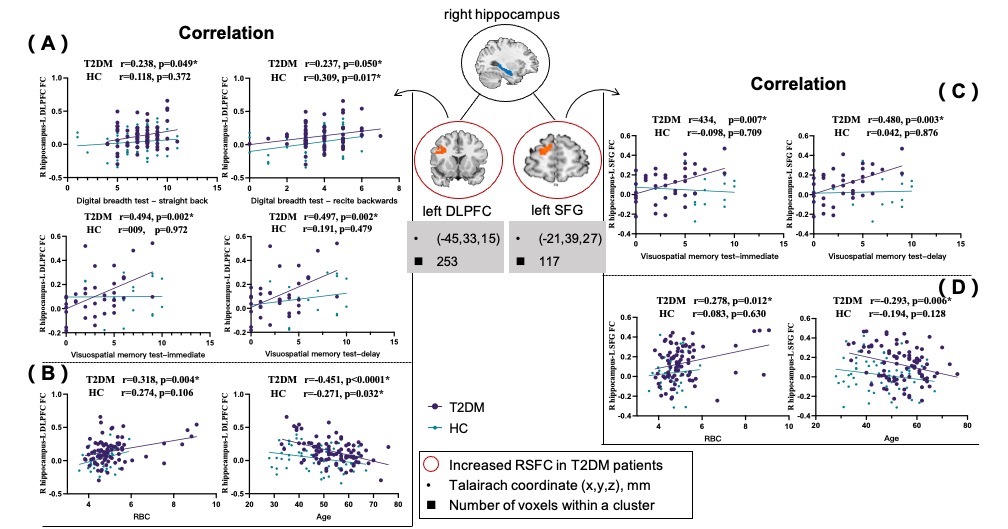
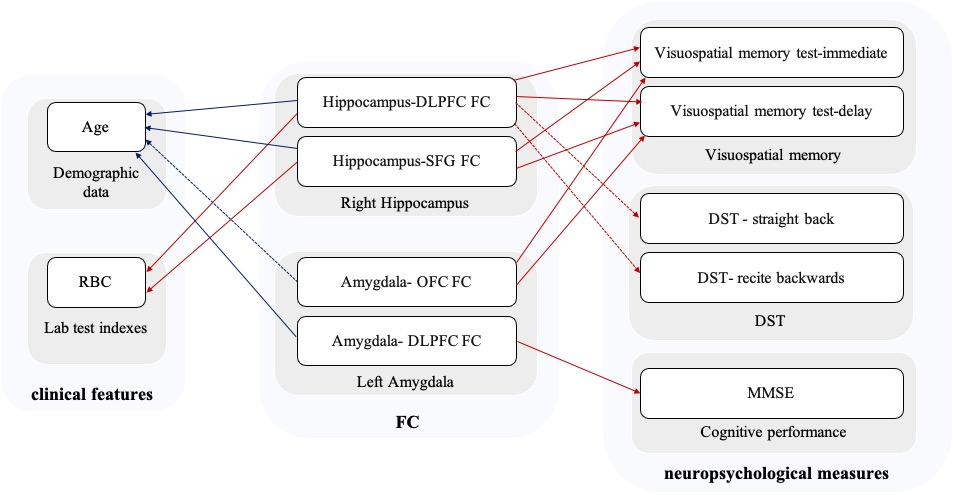
Compared to plateau Tibetan HC, T2DM showed both increase connectivity between the right hippocampus and left dorsal lateral prefrontal cortex (DLPFC), left superior frontal gyrus (SFG), and between the left amygdala and right orbitofrontal cortex (OFC), right DLPFC (Figure 1).The functional connectivity between the right hippocampus and left DLPFC, left SFG was positively correlated with red blood corpuscle (RBC) and negatively correlated with age in the T2DM group. Several neuropsychological measures were positively correlated with the functional connectivity between the right hippocampus and left DLPFC, left SFG, including the visuospatial memory test-immediate, visuospatial memory test-delay in the T2DM group (Fig2, 4).
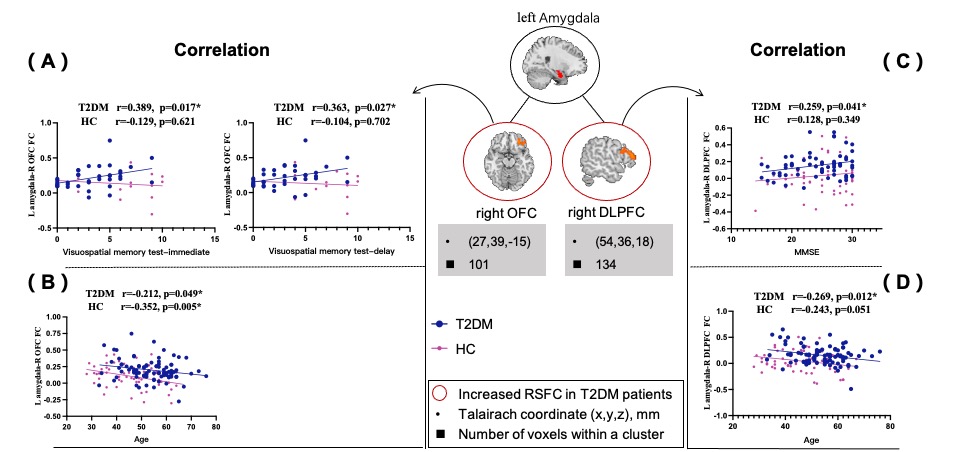
In the T2DM group, the functional connectivity between the left amygdala and right OFC, right DLPFC was negatively correlated with age. About neuropsychological measures, the functional connectivity between the left amygdala and right OFC was positively correlated with visuospatial memory test-immediate, visuospatial memory test-delay. The functional connectivity between left amygdala and right DLPFC was positively correlated with MMSE in the T2DM group (Fig3,4).
Discussion and Conclusion
To our knowledge, this is the first study to explore impairments in functional connectivity in plateau Tibetan T2DM using seed-based rsFC approach. First, we found that compared with plateau Tibetan HC, plateau Tibetan patients with T2DM showed both increased hippocampus and amygdala functional connectivity in left DLPFC and left SFG and right OFC. The differences in hippocampal FC were more pronounced in the younger population and gradually mitigated as age increased, while the age-dependent difference in the amygdala FC was not as obvious as that of the hippocampus. Second, we observed that increased FC between the right hippocampus and left DLPFC, left SFG was associated with increased RBC in plateau Tibetan patients with T2DM. The RBC was affected by the elevation[4], as the patients with T2DM in our study long lived on the plateau, we speculated that the increased hippocampal functional connectivity in diabetes patients may be affected by both disease and plateau environment. This finding is specific to the plateau T2DM patients, as most previous studies found decreased functional connectivity in the general T2DM population. Third, notably, abnormal functional connectivity of hippocampus and amygdala was associated with memory function impairments in T2DM. These findings of altered FC may provide important insights into the neural basis of diabetes-related cognitive decline in plateau Tibetan.Acknowledgements
This study was supported by the Science and technology project of Sichuan Province (Fund No. 2021YJ0161), the Medical Research project of Sichuan Province (Fund No. Q20042), the Science and technology Project of Tibet Autonomous Region: The central government guides local projects (Fund No. XZ202102YD0032C).References
1. Wood, A.G., et al., Brain Activation during Memory Encoding in Type 2 Diabetes Mellitus: A Discordant Twin Pair Study. J Diabetes Res, 2016. 2016: p. 3978428.
2. Wang, L., et al., Prevalence and Treatment of Diabetes in China, 2013-2018. JAMA, 2021. 326(24): p. 2498-2506.
3. Zhang, W., et al., Hippocampal subfields atrophy contribute more to cognitive impairment in middle-aged patients with type 2 diabetes rather than microvascular lesions. Acta Diabetologica, 2021. 58(8): p. 1023-1033.
4. Euser AG., et al., Gestational Diabetes Prevalence at Moderate and High Altitude. High Alt Med Biol. 2018 Dec;19(4):367-372.
Figures
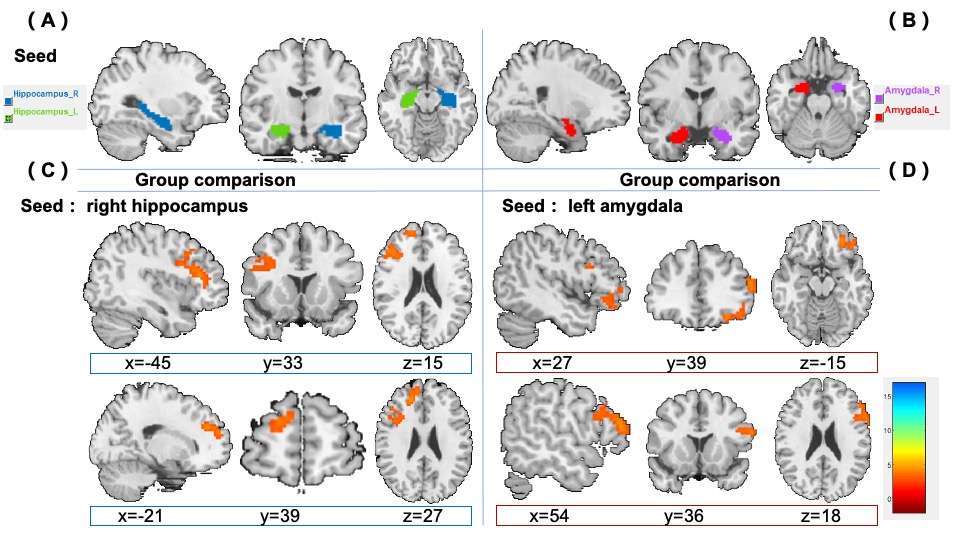
Figure 1. Significant differences were observed in the right hippocampus and left amygdala functional connectivity between the plateau Tibetan T2DM and plateau Tibetan HC groups. Thresholds were set using FWE correction at a p value of <0.05 (voxel p < 0.001, cluster size > 100). (A). the seed of right hippocampus, (B) the seed of left amygdala, (C). the right hippocampus and left DLPFC, left SFG showed a significant increase in the plateau Tibetan T2DM group, (D) the left amygdala and right OFC, right DLPFC showed a significant increase in the plateau Tibetan T2DM group.