3969
Readout-segmented EPI using 2D spatially-selective RF excitation pulses for DWI with reduced FOV
Wei Liu1, Thomas Benkert1, and Elisabeth Weiland1
1MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
1MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Pulse Sequence Design, Diffusion/other diffusion imaging techniques
In this work, we propose to further minimize the distortion and T2* blurring in DWI by the combination of readout-segmented EPI and 2D spatially-selective RF excitation. We demonstrate its application to DWI of the temporal lobe and the uterus. The experimental results based on volunteer scans show substantial distortion reduction in the proposed method, compared to the conventional 2DRF based single-shot EPI with reduced FOV.INTRODUCTION
Diffusion weighted imaging (DWI) has become a valuable and clinically well-established complement to traditional techniques due to its high sensitivity to detect and characterize lesions. Single-shot echo-planar imaging (ss-EPI) is widely used in DWI because of its short acquisition time. However, it is also well known that ss-EPI is sensitive to susceptibility artifacts and suffers from T2*-related blurring, limiting the clinical applications. A shorter echo train will increase the bandwidth of the sequence in the phase-encoding direction, which reduces distortions and enables higher spatial resolutions. To achieve this, 2D spatially-selective radiofrequency excitation pulses (2DRF) have been introduced for ss-EPI to enable the acquisition of small FOVs in phase-encoding direction while avoiding infolding artifacts from outside the FOV1-2. An alternative approach is based on multi-shot acquisitions, which also reduces the echo spacing and the echo-train duration, resulting in reduced distortion and T2*-related blurring. Readout-segmented EPI (rs-EPI) with 2D navigation3 is a multi-shot EPI technique that is increasingly used in clinical routine for acquiring high-resolution diffusion weighted (DW) images for various applications. In this study, we propose to further improve the distortion and T2* blurring by combining rs-EPI and 2DRF excitation and demonstrate its application to DWI of the temporal lobe and the uterus.METHODS
Data acquisition for temporal lobe imaging was performed on a 3 Tesla scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) equipped with a 20-channel head-neck coil. Coronal DW images from a healthy volunteer were acquired with rFOV-ss-EPI (ZOOMitPRO, Siemens Healthcare, Erlangen, Germany) and the proposed rFOV-rs-EPI research application. Imaging parameters were as follows: FOV = 200x80 mm2, 30 slices with 2 mm slice thickness without slice gap, diffusion mode = 4-scan trace, no in-plane acceleration. In rFOV-ss-EPI, matrix size = 134x52, TE/TR = 69/5500 ms, echo spacing = 0.95 ms, b = 0 s/mm2 with 2 averages, b = 1000 s/mm2 with 8 averages, total scan time = 3:14 min; in rFOV-rs-EPI, matrix size = 160x64, TE/TR = 69/5000 ms, segment number = 5, and echo spacing = 0.54 ms, b = 0 s/mm2 with 1 average, b = 1000 s/mm2 with 2 averages, total scan time = 3:57 min.Data acquisition for uterus imaging was performed on a 3 Tesla scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) equipped with a 32-channel spine coil and an 18-channel body coil. Axial DW images from a healthy volunteer were acquired with rFOV-ss-EPI and the proposed rFOV-rs-EPI research application. Imaging parameters were as follows: FOV = 200x102 mm2, 22 slices with 3 mm slice thickness without slice gap, diffusion mode = 4-scan trace, no in-plane acceleration. In rFOV-ss-EPI, matrix size = 122x62, TE/TR = 74/4000 ms, echo spacing = 0.96 ms, b = 50 s/mm2 with 2 averages, b = 800 s/mm2 with 11 averages, total scan time = 3:38 min; in rFOV-rs-EPI, matrix size = 118x60, TE/TR = 55/4800 ms, segment number = 5, and echo spacing = 0.34 ms, b = 50 s/mm2 with 1 average, b = 800 s/mm2 with 2 averages. To achieve a comparable scan time of 4:07 min, readout partial Fourier 7/8 was additionally employed.
RESULTS
Figs 1A and 1B show rFOV-ss-EPI and rFOV-rs-EPI images of the temporal lobe. The two acquisitions demonstrate comparable anatomical details. As expected, distortions can be further reduced in rFOV-rs-EPI while achieving higher resolution and reduced blurring. As can be seen, higher acquisition matrix and less averages in rFOV-rs-EPI result in a slight SNR drop, compared to the rFOV-ss-EPI.Figs 2A and 2B show rFOV-ss-EPI and rFOV-rs-EPI images of the uterus. Again, the two acquisitions demonstrate comparable anatomical details. The distortions can be well reduced in rFOV-rs-EPI. Due to the use of readout partial Fourier in rFOV-rs-EPI, a slight reduction in sharpness can be seen.
DISCUSSION AND CONCLUSION
We have demonstrated that 2DRF excitation scheme can be applied to rs-EPI DWI to further improve distortions and T2*-related blurring compared with conventional rFOV-ss-EPI DWI. While this work focused on the acquisition side and no dedicated reconstruction techniques were applied, the proposed method can also be combined with in-plane GRAPPA to reduce the echo train length for further reduced distortions or deep learning-based reconstruction schemes to reduce scan times and increase SNR. Altogether, the proposed rFOV-rs-EPI technique has the potential to enable improved diagnosis especially in applications which are prone to susceptibility-related artifacts such as prostate DWI in the presence of rectal gas, inner ear DWI and pancreas DWI.Acknowledgements
No acknowledgement found.References
1. Rieseberg S, Frahm J, Finsterbusch J. Two-dimensional spatially-selective RF excitation pulses in echo-planar imaging. Magn Reson Med 2002; 47:1186-1193.
2. Finsterbusch J. Improving the performance of diffusion-weighted inner-field-of-view EPI based on 2D-selective RF excitations by tilting the excitation plane. J. Magn. Reson. Imaging 2012; 35:984-992.
3. Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator based reacquisition. Magn Reson Med 2009; 62(2):468-475.
Figures
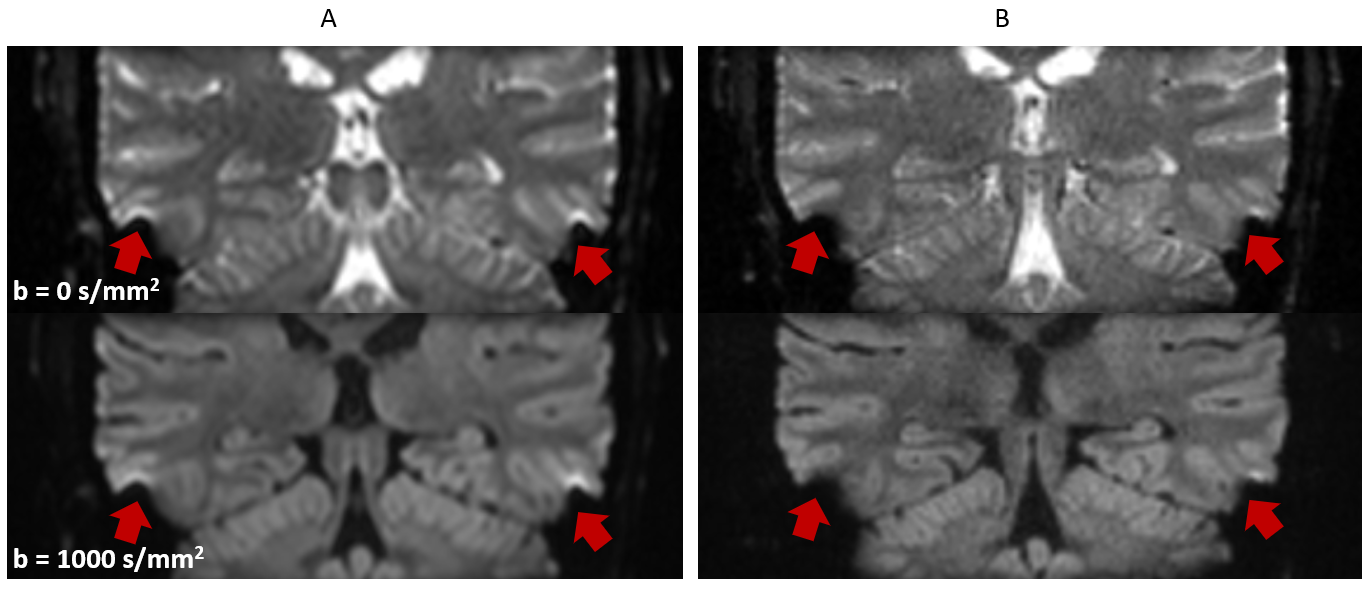
Figure 1. Representative results applying rFOV-ss-EPI (A)
and rFOV-rs-EPI (B) in the temporal lobe. Compared with rFOV-ss-EPI, susceptibility-related
artifacts from air-filled cavities which lead to distortions and signal pile-up,
are further reduced when using the proposed rFOV-rs-EPI (red arrows).
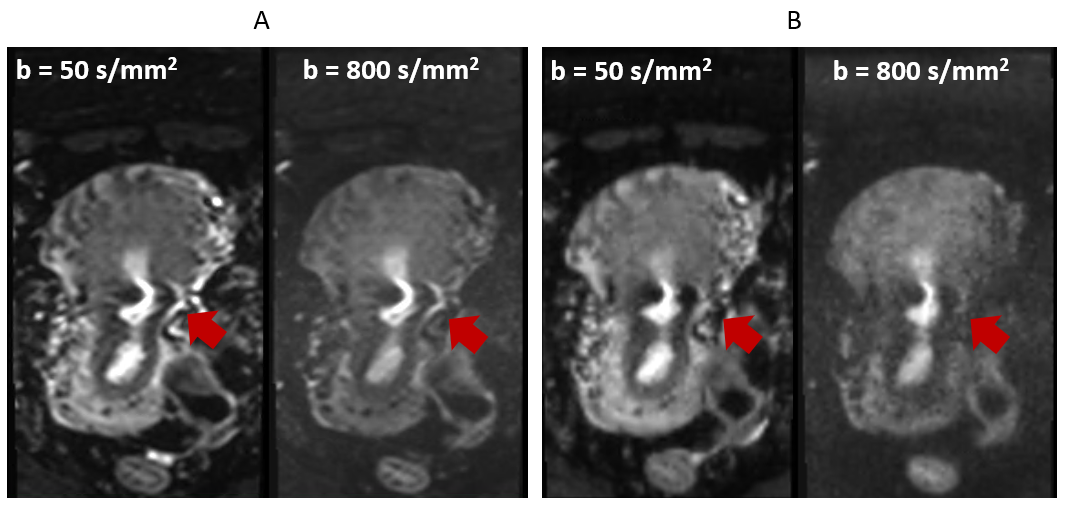
Figure 2. Representative results applying rFOV-ss-EPI (A) and rFOV-rs-EPI (B) in the uterus. Compared with rFOV-ss-EPI, susceptibility-related
artifacts can be further reduced when using the proposed rFOV-rs-EPI (red
arrows).
DOI: https://doi.org/10.58530/2023/3969