3878
Investigation of deep learning reconstruction in MR imaging of pancreatic space occupying lesions1Department of Radiology, West China Hospital, Sichuan University, Chengdu, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Image Reconstruction
At present, the resolution of magnetic resonance image is still limited to the detection of pancreatic space occupying lesions. In this work, quantitative and qualitative analysis of pancreatic images of T1WI and DWI with built-in DL Recon was carried out. The results showed that the images obtained by the sequence with built-in DL Recon were better than the original images in terms of SNR, CNR and subjective scores. It is confirmed that deep learning reconstruction can improve image resolution and has potential in the detection of space occupying lesions in pancreas.Background and Aim
Magnetic resonance imaging (MRI) plays an important role in the diagnosis of space occupying lesions of the pancreas. However, the detection and characterization of small lesions is often limited by the image spatial resolutions, which places conflicting requirements with scan time and signal to noise ratio (SNR). Deep learning reconstruction (DL Recon) utilizes convolutional network to reduce noises while preserving the image details, and has been applied in several anatomies (1-6). This study aimed to investigate the use of DL recon in the pancreas, especially the space occupying lesions.Methods
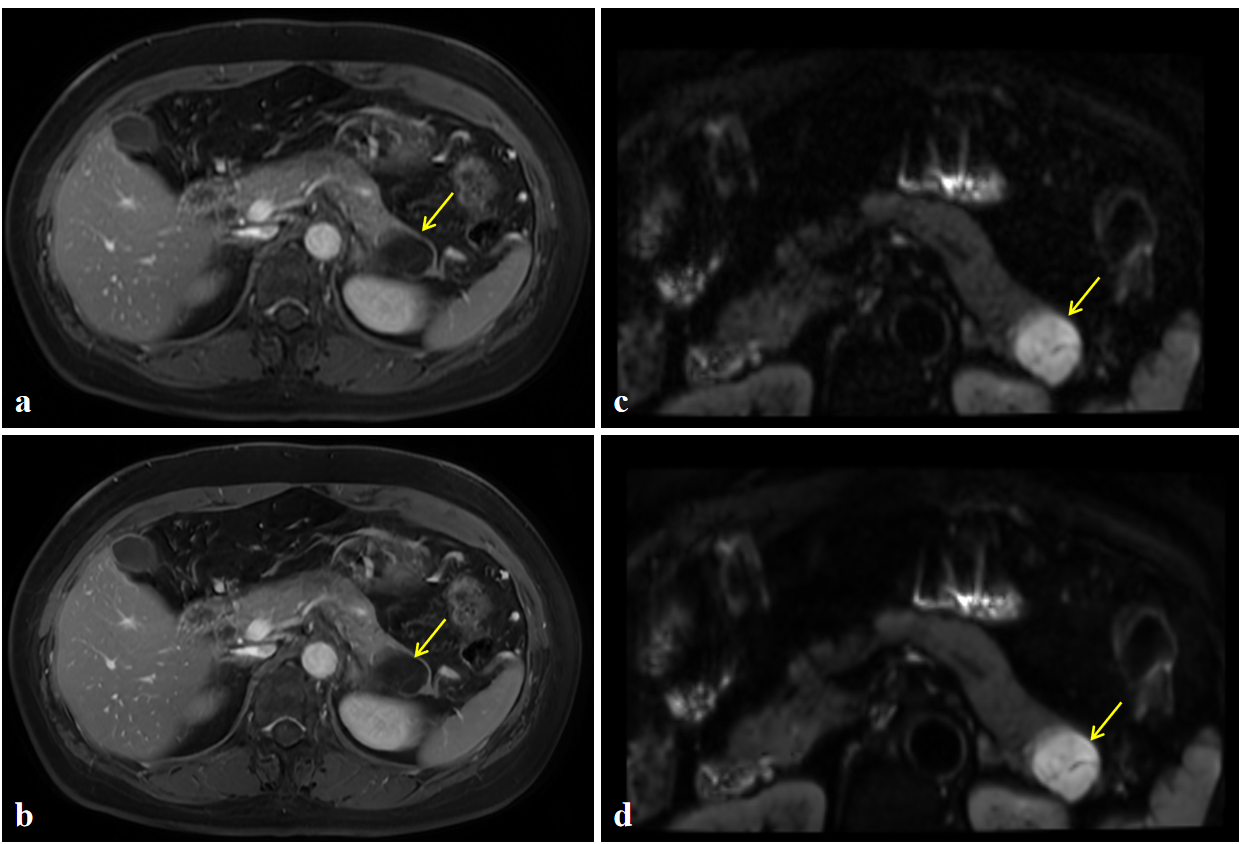
Local ethic approval was granted for this study and consent forms were obtained from each participant. A total of 21 patients with space occupying pancreatic lesions were enrolled in this study from July 2022 to October 2022. All examinations were performed on a 3 T MRI scanner (SIGNATM Architect 3 T, GE Healthcare, Milwaukee, USA). A 30-channel AIRTM Anterior Array Coil (GE Healthcare, USA) was used. 2D axial (Ax) fast spin echo (FSE) T1 weighted image (T1WI) with contrast enhancement (+C) and field-of-view optimized and constrained undistorted single-shot (FOCUS) DWI were performed with both DL Recon and conventional reconstruction. The sequence parameters were as follows: 2D Ax FSE T1WI +C (TR = 120 ms, TE = 1.7 ms, flig angle = 80°, FOV = 300 × 300 mm, matrix = 320 × 192, slice thickness = 7.0 mm, spacing = 2.0 mm, resolution = 1.2 × 2.1 × 7.0 mm, NEX = 1, scanning time = 16s). Ax FOCUS DWI (TR = 6000 ms, TE = 69.1 ms, flig angle = 90°, FOV = 300 × 300 mm, matrix = 140 × 70, slice thickness = 3.6 mm, spacing = 1.0 mm, resolution = 1.7 × 1.7 × 3.6 mm, scanning time = 3min 18s, b value = 50 and 800 s/mm2, NEX = 1 and 8).Deep learning reconstruction images and conventional reconstruction images were subjectively and objectively evaluated. In the subjective evaluation, two radiologists with more than 5 years of imaging diagnosis experience used the "five-point method" to score the image uniformity, pancreatic edge sharpness, lesion quality and overall image quality. When there was a difference in scoring, two radiologists reached consensus after discussion. In the objective evaluation, a radiologist with more than 10 years of imaging diagnosis experience used the following formula to measure the signal-to-noise ratio (SNR) and the contrast noise ratio (CNR) of pancreas and lesions by delineating the region of interest (ROI) in DL Recon 2D Ax FSE T1WI +C and its original images, DL Recon Ax FOCUS DWI and its original images.The measured values included the signal intensity (SI) and standard deviation (SD) for each region of interest.$$SNR=\frac{SI_{interested\space tissue}}{SD_{noise}}$$ $$CNR=\frac{|SI_{interested\space tissue}-SI_{contrast\space tissue}|}{SD_{noise}}$$ The locations of ROI in the T1WI images were the head of pancreas, the body of pancreas, the tail of pancreas, the lesion, the muscle, and the image background. The locations of ROI in the DWI images were respectively the head of the pancreas, the body of the pancreas, the tail of the pancreas, the lesion, the spine, and the aorta (since there was no air background in the DWI images, the aorta was selected as the image background for the measurement). It should be noted that after measuring the ROI signals at the head, tail and body of the pancreas, the average values of the three were taken as the signals of the whole pancreas, and then SNR and CNR were calculated.
SPSS (version 27.0, IBM, Armonk, NY, USA) software was used for statistical analysis. The subjective and objective difference between DL recon and original groups were evaluated with Wilcoxon signed-rank test and paired t-test. P < 0.05 indicates that the difference is statistically significant.
Results
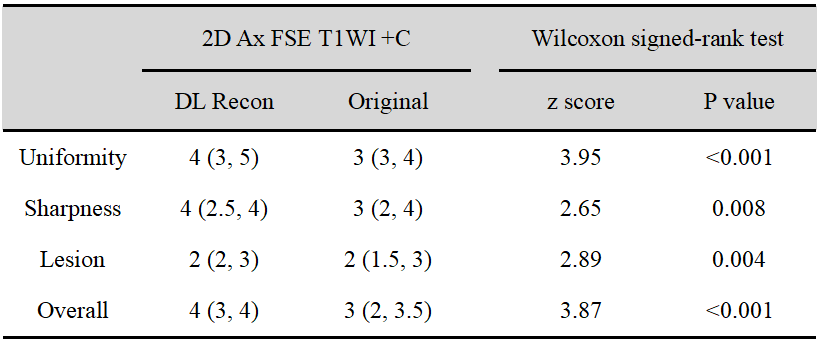
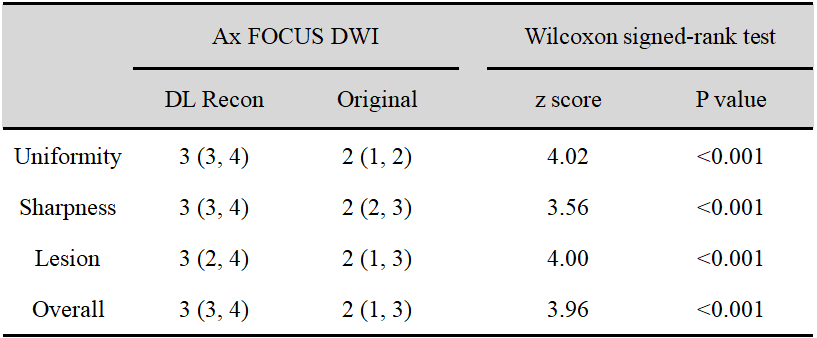
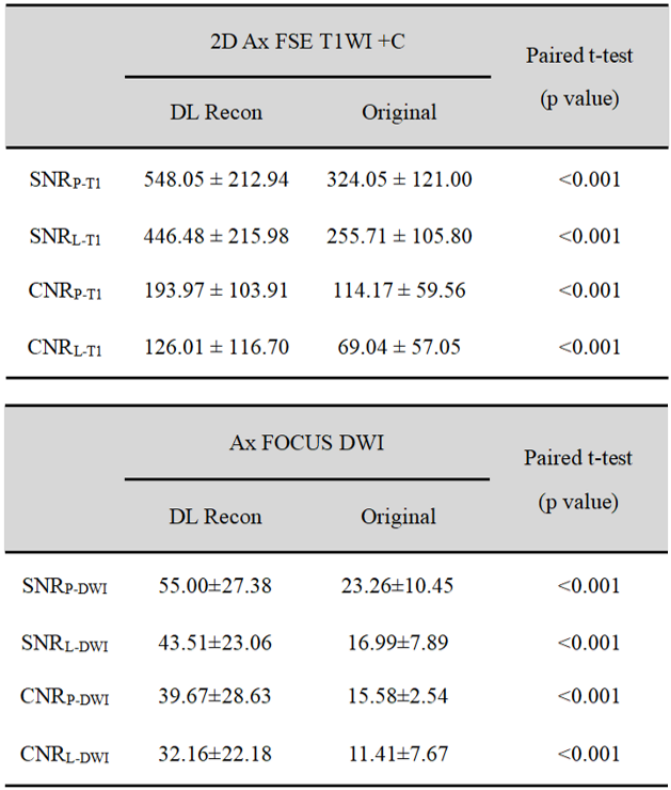
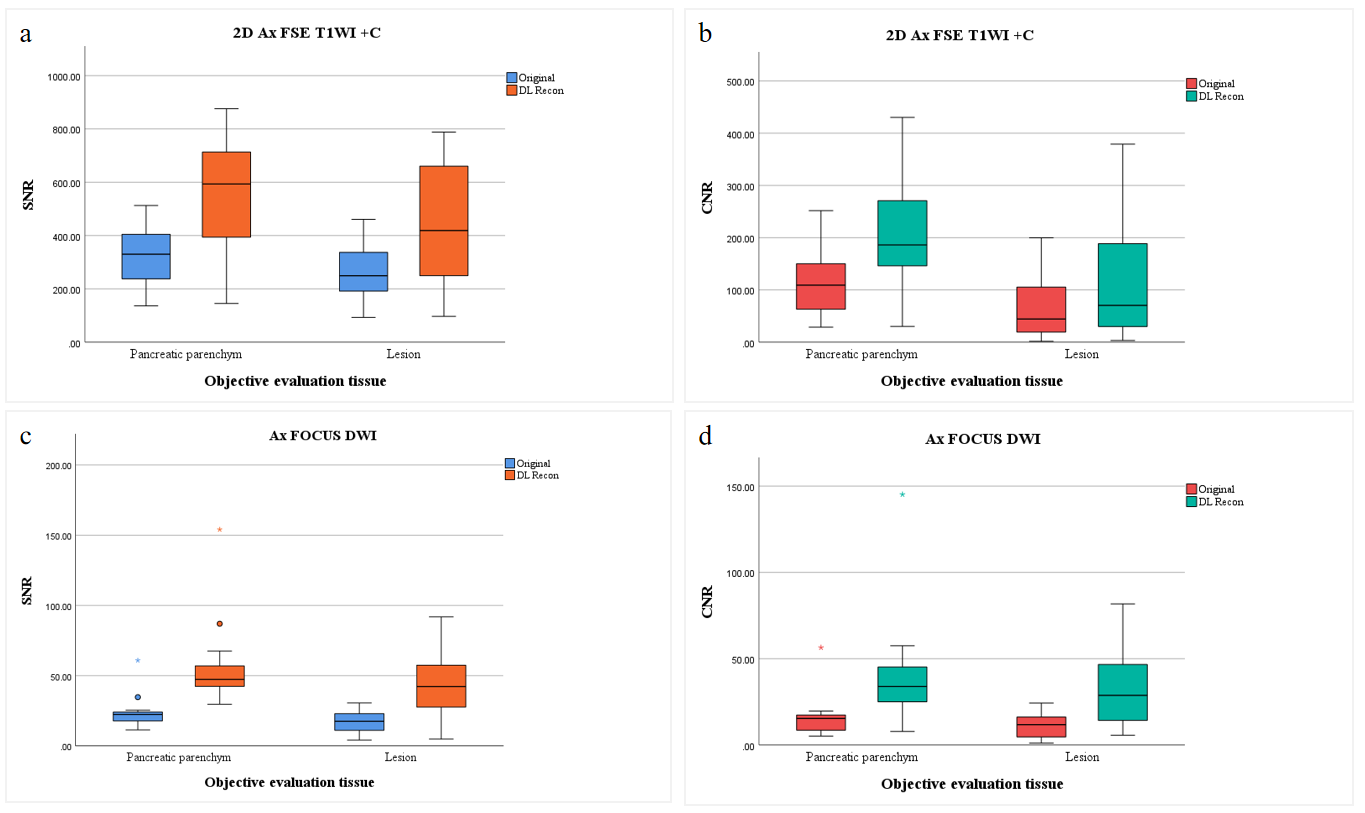
A typical set of DL reconstruction and conventional reconstruction images are shown in Figure 1.The subjective evaluation results of DL Recon 2D Ax FSE T1WI +C and DL Recon Ax FOCUS DWI were significantly better than their original images (The results are shown in Figure 2 and Figure 3).The objective evaluation results of DL Recon 2D Ax FSE T1WI +C with its original image and DL Recon Ax FOCUS DWI with its original images were shown in the Figure 4 and Figure 5. According to the figures, in the two DL Recon sequences, both the pancreatic parenchyma and the lesion tissue, the SNR and CNR obtained by calculation were better than the original images, and the difference between the groups was statistically significant (P < 0.001).
Conclusions
Deep learning reconstruction can reduce the noises in MR images, which may be translated into spatial resolution and/or scan time. In this work, we have demonstrated the feasibility and advantage of incorporating DL reconstruction (AIR Recon DL) in pancreatic imaging using both qualitative scoring and quantitative measures. Deep learning reconstruction may have potential in clinical routine pancreatic imaging.Acknowledgements
No acknowledgement found.References
1. Harrington KA, Shukla-Dave A, Paudyal R, Do RKG. MRI of the Pancreas. J Magn Reson Imaging. 2021; 53(2): 347-359.
2. van Huijgevoort NCM, Del Chiaro M, Wolfgang CL, van Hooft JE, Besselink MG. Diagnosis and management of pancreatic cystic neoplasms: current evidence and guidelines. Nat Rev Gastroenterol Hepatol. 2019; 16(11): 676-689.
3. Siddiqui N, Vendrami CL, Chatterjee A, Miller FH. Advanced MR Imaging Techniques for Pancreas Imaging. Magn Reson Imaging Clin N Am. 2018; 26(3): 323-344.
4. Fukukura Y, Shindo T, Hakamada H, et al. Diffusion-weighted MR imaging of the pancreas: optimizing b-value for visualization of pancreatic adenocarcinoma. Eur Radiol. 2016; 26(10): 3419-3427.
5. Barral M, Taouli B, Guiu B, et al. Diffusion-weighted MR imaging of the pancreas: current status and recommendations. Radiology. 2015; 274(1): 45-63.
6. Matsuyama T, Ohno Y, Yamamoto K, et al. Comparison of utility of deep learning reconstruction on 3D MRCPs obtained with three different k-space data acquisitions in patients with IPMN. Eur Radiol. 2022; 32(10): 6658-6667.
Figures