3837
Exploration of age-related hemodynamic and mechanical changes in the human thoracic aorta using an atlas based approach
Elodie Piot1, Nicolas Duchateau1, Marine Menut2, Benyebka Bou-Said2, Patrick Clarysse1, Philippe Douek1,3, Karl Kunze4, Rene Botnar5, Sara Boccalini6, Claudia Prieto5, and Monica Sigovan1
1CREATIS, Lyon, France, 2INSA de Lyon, Lyon, France, 3Departement of Radiology, HCL, Lyon, France, 4Siemens Helthineers, London, United Kingdom, 5School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 6Department of Radiology, HCL, Lyon, France
1CREATIS, Lyon, France, 2INSA de Lyon, Lyon, France, 3Departement of Radiology, HCL, Lyon, France, 4Siemens Helthineers, London, United Kingdom, 5School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 6Department of Radiology, HCL, Lyon, France
Synopsis
Keywords: Data Processing, Blood vessels
Understanding the hemodynamic involvement in a vascular pathology requires inter-subject comparisons that are not straightforward due to variability in terms of aorta morphology. Hemodynamic atlases can facilitate detection of intra-group characteristics. We propose here a workflow to create a hemodynamic atlas using 4D Flow MRI. In addition, we propose to investigate the aorta wall stiffness using non-rigid image registration and inverse mechanical modeling. This type of analysis is expected to improve pathophysiological understanding of vascular disease, by enabling the investigation of potential correlations between hemodynamic and wall mechanical properties at each point of the aorta.INTRODUCTION
4D Flow MRI offers valuable hemodynamic information in individual subjects. Yet, understanding the hemodynamic involvement in a vascular pathology requires inter-subject comparisons that are not straightforward due to variability in terms of aorta morphology. Hemodynamic atlases can facilitate these comparisons and facilitate detection of intra-group characteristics. We propose here a workflow to create a hemodynamic atlas using 4D Flow MRI. We then explore age related differences in aorta hemodynamics using the proposed workflow.METHODS
15 male subjects without any known cardiovascular pathology were included as follows: 8 in the younger group (mean age = 28 ± 3 years) and 7 in the older group (mean age = 55 ± 6 years). Imaging was performed on a 1.5T system (Siemens Avanto) and included a retrospectively cardiac gated 4D Flow MRI Cartesian acquisition and a 3D T2-prep simultaneous bright-blood and black-blood phase sensitive inversion recovery sequence (BOOST) 1. The 4D Flow acquisition was performed with TE=2.7 ms, TR=43 ms, FA=8◦, VENC=120-180 cm/s, 2.3x2.3x2.8 mm voxel. An acceleration factor of 7.6 was used in combination with compressed-sensing reconstruction for an approximate acquisition time of 6 minutes. 4D Flow data was analyzed using a Matlab-based toolbox; briefly, time averaged phase contrast angiography (PCMRA) was semi-automatically segmented and then meshed. Several hemodynamic parameters were then computed using a finite element method2. The BOOST sequence was performed in a coronal orientation using: TE=1.4 ms, TR=313 ms, TI = 150 ms, FA=90◦, VENC=120-180 cm/s, 1.4 mm isotropic voxel; and 2D-image based navigation to track and correct for respiratory motion. The acquisition was performed twice for each volunteer, once in diastole and once in systole. The resulting bright-blood non-contrast angiography volumes were registered using a non-rigid image registration algorithm (Elastix) to obtain the displacement field from diastole to systole. Subsequently, the displacement of the aorta was obtained by interpolating the displacement field on the previously obtained segmentation from PCMRA. The aorta wall was estimated as a constant 2 mm thickness at the interface of the lumen. Finally, Lagrangian strain maps of the aorta wall were estimated by the derivation of the displacement fields. Atlas creation: State-of-the-art atlas estimation software (Deformetrica, v.4.3.0) was used to estimate a reference shape for each subgroup and to define anatomical correspondences between each subject and this reference. Then, hemodynamic parameters, both volumetric (velocity, vorticity and helicity) and surface defined parameters (wall shear stress (WSS) and oscillatory shear index (OSI) for example) and Lagrangian strain maps for each subject were transported to this reference using the aforementioned anatomical correspondences. Finally, representative patterns were estimated for each subgroup by averaging the mechanical data of each subject aligned to the reference.RESULTS
Examples of the computed biomechanical atlases are displayed in the figure. Morphologically, the aorta presented overall larger diameters and higher curvature of the aortic arch in the older group, while curvature of the ascending aorta was slightly lower. In the same region of increased curvature, flow disturbance appeared to be stronger, as demonstrated by increased regurgitant flow, OSI, and eccentricity. Flow eccentricity and area of increased OSI were also higher in the elder group in the ascending aorta. Oppositely, strain was higher for the younger group compare to the older one, indicating lower stiffness.DISCUSSION
We present here initial results of an atlas-based method to investigate age-related changes in aorta shape, hemodynamics, and stiffness. In terms of the hemodynamic changes with age, our results are in agreement with the recent study of Callaghan et al.3. While the aforementioned study was performed in a large population, the actual assessment of the hemodynamic parameters was done only at specific locations along the aorta. In addition, the mechanical assessment of the aorta wall obtained is also in agreement with current knowledge that arterial walls stiffen with increasing age. Our proposed approach appears promising and should be investigated in a larger cohort. The atlas-based analysis allows much finer assessment of both shape and biomechanical differences, up to each element of the reference aortic mesh. This type of analysis is expected to improve pathophysiological understanding of pathologies4, by enabling the investigation of potential correlations between hemodynamic and wall mechanical properties at each point of the aorta.Acknowledgements
Funding: ANR-18-CE19-0025-01, Institut Universitaire de France.References
1. Ginami G., Neji R., Phinikaridou A., et al (2018) MRM 79 :1460-1472
2. Sotelo J, Urbina J, Valverde I, et al (2016) IEEE Trans Med Imaging 35:1475–1487.
3. Callaghan FM, Bannon P, Barin E, et al (2019) J Magn Reson Imaging 49:90–100.
4. van Ooij P, Potters WV, Nederveen AJ, et al (2014) Magn Reson Med
Figures
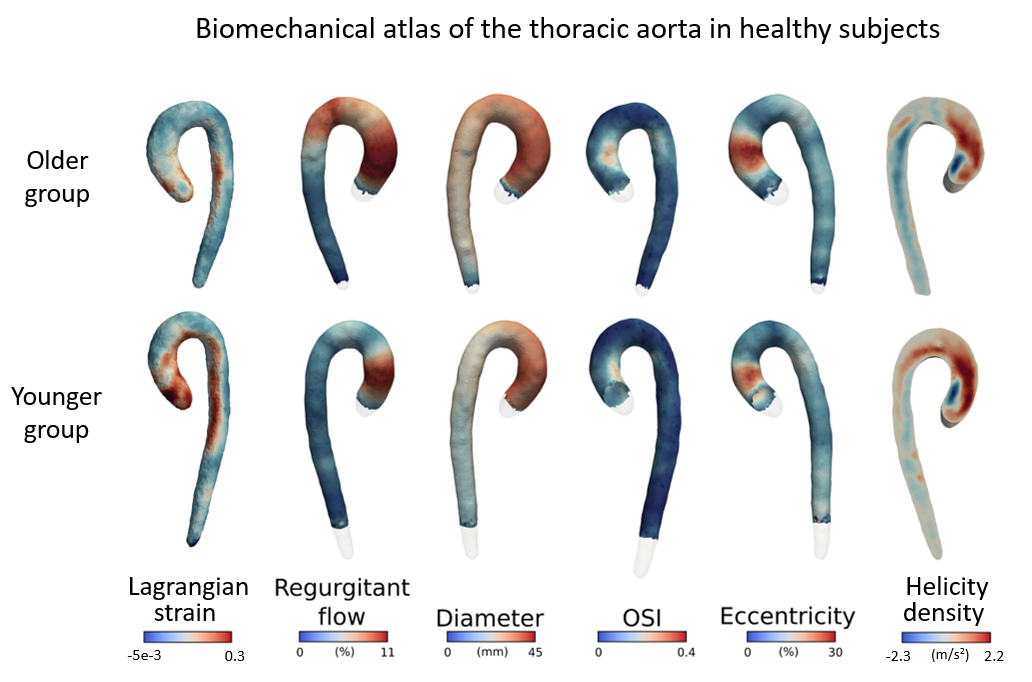
Results of the atlas construction in the older group (top row) and the
younger group (bottom row). Lagrangian strain maps and hemodynamic parameters
are presented as average values per group. On average, the older group
presented a larger aortic diameter, stronger flow disturbance and stiffer aorta
wall.
DOI: https://doi.org/10.58530/2023/3837