3831
Hemodynamics of common iliac arteries is associated with the risk of abdominal aortic aneurysm: assessment using 4D flow MRI1West China Hospital, Sichuan University, Chengdu, China, 2Clinical Science, Philips Healthcare, Chengdu, China, Chengdu, China
Synopsis
Keywords: Flow, Cardiovascular, Abdominal aortic aneurysm
Studies have confirmed the interaction between iliac arteries and abdominal aortic aneurysms. Four-dimensional (4D) flow MRI can reveal the hemodynamic changes of common iliac arteries in abdominal aortic aneurysm and health controls. In this study, we tried to explain the relationship between the changes of iliac artery hemodynamics and the asymmetry of the left and right iliac artery blood flow and the occurrence and development of abdominal aortic aneurysms in patients.Introduction
Abdominal aortic aneurysm (AAA) is defined as a local dilation of the abdominal aorta that exceeds 50% of the normal diameter, or a dilation in size that is greater than 30mm.With the aggravation of population aging, the incidence of AAA is increasing, and the incidence of AAA in China has tripled in the past decade. Therefore, it is important to understand the underlying mechanisms that contribute to the weakening of AAA growth and structure in order to diagnose lesion progression and design appropriate patient-specific interventions. One under-investigated area of AAA research is how changes in iliac arteries flow alter infrarenal aortic hemodynamics and aneurysm expansion, which results in approximately one in five AAA cases with aneurysms of the common iliac artery (CIA)(1). AAA can induce most emerging-blood flow in healthy segments of the arterial system far downstream of the emerging-hair. In the same way, abnormal blood flow in the iliac artery may lead to the appearance of abdominal aortic aneurysms, or even further accelerate the expansion of abdominal aortic aneurysms(2). Iliac stenosis may have upstream effects on AAA progression, which has been demonstrated in animal models(3). There are few hemodynamic studies on iliac arteries in abdominal aortic aneurysm(4), but researchers trying to figure out the relationship between CIA and AAA formation have focused more on CIA geometric parameters and strategies to overcome surgical difficulties. Therefore, the aim of this study was to investigate the hemodynamics of iliac arteries in healthy volunteers and AAA patients using 4D flow MRI. Through this study, we can not only obtain the general morphological characteristics of the iliac artery vessels, but also pay more attention to the hemodynamic characteristics of the iliac artery, trying to explore the relationship between the abnormal blood flow of the iliac artery and the occurrence of auxiliary aneurysm.Methods
Between December 2021 and May 2022, 8 volunteers (58.79±13.23 years) and 8 AAA patients (66.53±10.34 years) were included. All the subjects underwent MRI on a 3.0T MR scanner using a 32-channel phased array body coil (Ingenia Elition, Philips Healthcare). 4D flow MRI was conducted with a flip angle of 10° and an echo time/repetition time (TE/TR) of 4.1/8.0 msec. The temporal resolution was 30.2 msec. Respiratory gating was not used in 4D flow MRI acquisition when considering the examination time. Three-directional velocity-encoding sensitivity (VENC) was set to 80-150 cm/second. All images were analyzed using Circle Cardiovascular Imaging 42 (CVI, Canada). Hemodynamic parameters, including total flow volume, peak velocity and WSS of left and right common iliac artery were recorded. The normality of the data was tested using the Kolmogorov‒Smirnov test, and the homogeneity of the variance was tested using the Levene method. Data were expressed as mean ± standard deviation (SD) if normally distributed and as median (interquartile range) in case of skewed distribution. Two-tailed unpaired Student’s t-test was used to compare volunteers with AAA and P<0.05 was considered statistically significant. Two-tailed paired Student’s t-test was used to compare the hemodynamic parameters of left and right iliac arteries.Results
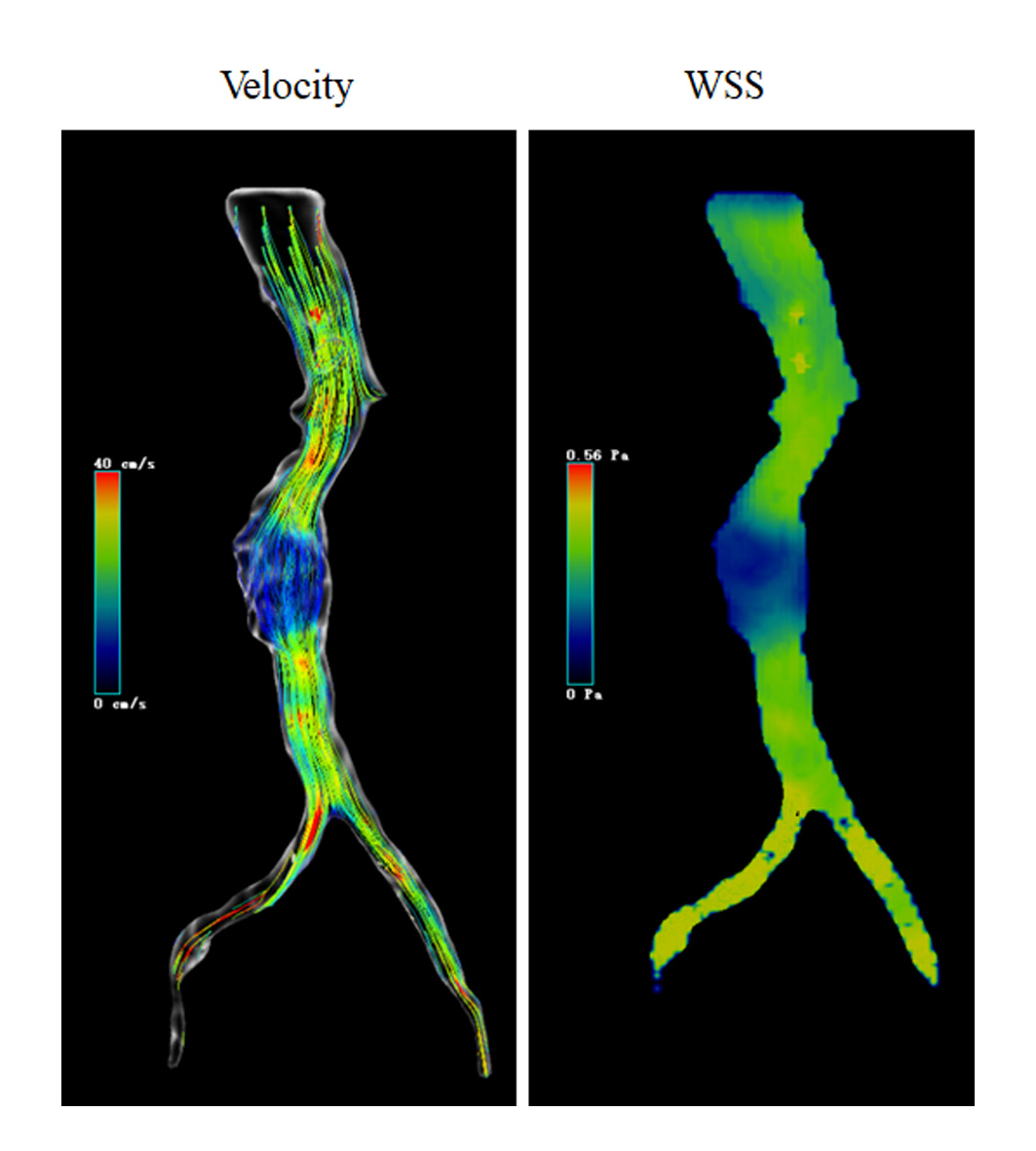
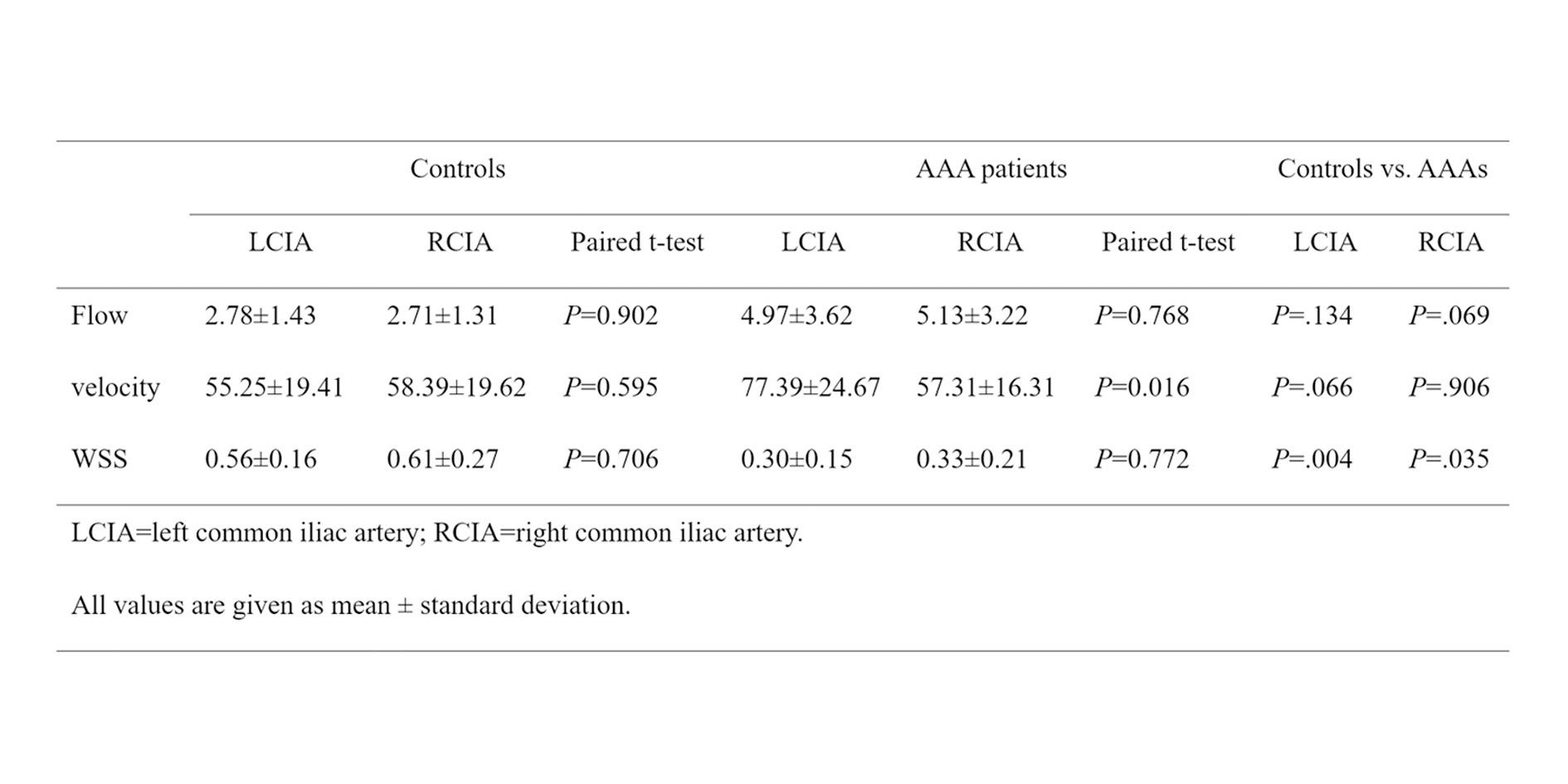
There was no significant difference in flow volume between controls and AAA both in LCIA and RCIA (Table 1). However, the WSS decreased in AAA patients both in LCIA (0.56±0.16 vs. 0.30±0.15, P=0.004, Table 1) and RCIA (0.61±0.27 vs. 0.33±0.21, P=0.035, Table 1). The WSS visualization was shown in Figure 1. In healthy volunteers, there was good consistency of hemodynamic parameters between the left and right iliac artery. However, peak velocity between left and right common iliac arteries is significantly different in AAA (77.39±24.67 vs. 57.31±16.31, P=0.016, Table 1).Discussion
In this study, 4D flow MRI were used to evaluate the iliac arteries dynamics changes between healthy controls and AAA patients. In patients with abdominal aortic aneurysms, the WSS of the iliac arteries was significantly reduced. At the same time, there were more misalignment of peak velocity between the left and right common iliac arteries. Most studies believe that low WSS has the highest correlation with AAA rupture, which indicates that low WSS is not only related to the generation of thrombosis, but also may directly cause rupture due to irreversible vascular injury(5). There were many reasons for the occurrence of abdominal aortic aneurysms. This study only confirmed that abdominal aortic aneurysms were associated with decreased WSS of iliac arteries and inconsistent blood flow parameters of left and right iliac arteries. However, this association was not equal to the exact causal relationship, and large samples and long-term follow-up investigation were needed to confirm it.Conclusion
In this study, 4D flow MRI were used to evaluate the iliac arteries dynamics changes between healthy controls and AAA patients. Meanwhile, the changes of blood flow in the iliac artery, the relationship between the hemodynamic asymmetry of the left and right iliac arteries and aneurysms were further analyzed. In AAA patients, the WSS of both left and right iliac arteries was decreased, and the hemodynamic parameters between the left and right iliac arteries are asymmetrical. These changes are of great value for predicting the development of abdominal aortic aneurysms and even for predicting the occurrence and development of iliac aneurysms.Acknowledgements
None.References
1. Armon MP, Wenham PW, Whitaker SC, Gregson RH, Hopkinson BR. Common iliac artery aneurysms in patients with abdominal aortic aneurysms. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 1998; 15:255-257.
2. Drewe CJ, Parker LP, Kelsey LJ, Norman PE, Powell JT, Doyle BJ. Haemodynamics and stresses in abdominal aortic aneurysms: A fluid-structure interaction study into the effect of proximal neck and iliac bifurcation angle. Journal of biomechanics. 2017; 60:150-156.
3. Sangha GS, Busch A, Acuna A, et al. Effects of Iliac Stenosis on Abdominal Aortic Aneurysm Formation in Mice and Humans. Journal of vascular research. 2019; 56:217-229.
4. Coulston J, Baigent A, Selvachandran H, Jones S, Torella F, Fisher R. The impact of endovascular aneurysm repair on aortoiliac tortuosity and its use as a predictor of iliac limb complications. Journal of vascular surgery. 2014; 60:585-589.
5. Boyd AJ, Kuhn DC, Lozowy RJ, Kulbisky GP. Low wall shear stress predominates at sites of abdominal aortic aneurysm rupture. Journal of vascular surgery. 2016; 63:1613-1619.
Figures