3822
Flow Displacement and Wall Shear Stress in Individuals with Mild-to-Moderate Aortic Dilation and Tricuspid Aortic Valves
1Department of Health, Medicine and Caring Sciences (HMV), Linköping University, Linköping, Sweden, 2Center for Medical Image Science and Visualization (CMIV), Linköping University, Linköping, Sweden, 3Department of Cardiology in Linköping, and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
Synopsis
Keywords: Flow, Vessels, Aorta
Altered hemodynamics may play a role in the development of ascending aortic aneurysms. In this study, we sought to investigate wall shear stress and flow displacement in patients with tricuspid aortic valve and mild-to-moderate dilatation of the ascending aorta, and age-and sex- matched non-dilated controls. Dilated patients had lower average velocity and wall shear stress in the ascending aorta, and higher flow displacement. This study shows that individuals with dilatation have altered hemodynamics even in an early stage of the disease.
Background
Ascending aortic aneurysm is an asymptomatic disease that it is often not detected until dissection or rupture occurs. Basic vessel dimensions are the primary measurements used clinically to risk-stratify patients. High circumferential wall shear stress (WSS) has been associated with aortic growth in patients with bicuspid aortic valve1,2, but less is known about patients with tricuspid aortic valve (TAV). A recent study suggested that ascending aortic growth is associated with low WSS and high flow displacement in patients with TAV3, although only a small number of patients were available. In this cross-sectional study, we sought to obtain a comprehensive view of WSS and flow displacement in a cohort of TAV patients and age- and sex-matched controls.Methods
40 patients with ascending aortic diameter >40 mm and 35 age- and sex-matched controls with ascending aortic diameter <40 mm were recruited from the Swedish CArdioPulmonary bioImage Study (SCAPIS) in Linköping. Patients had a mild-to-moderate dilation classified from CT coronary angiography. Contrast-enhanced MR angiography (CE-MRA) volumes were acquired with a 1.5 T Philips Ingenia scanner (Philips Healthcare, Best, the Netherlands) following administration of a Gadolinium contrast agent (Magnevist, Bayer Schering Pharma AG) and used to manually determine relevant aortic landmarks, namely the aortic valve and the insertion of the brachiocephalic trunk. 4D Flow MRI data were acquired with a free-breathing, respiratory navigator gated, retrospectively cardiac-gated sequence immediately after the CE-MRA. 4D flow datasets were corrected for background phase offset and phase wrapping. Time resolved segmentations were created automatically with an atlas-based method, combined with manual adjustments4. The ascending aorta was defined from the valve to the insertion of the brachiocephalic trunk, based on the landmarks placed on the CE-MRA. Peak systole was defined as the timeframe with peak average velocity in the ascending aorta. Maximum and average diameter in the ascending aorta were obtained from the cross-sectional planes. 3D peak systolic WSS maps were computed with the method of Potters et al5, and average and maximum WSS in the ascending aorta were reported. Flow displacement at peak systole was assessed at 7 equidistant planes in the ascending aorta6. The method workflow is shown in Figure 1. Student’s t-tests were used to compare values between the two cohorts, with a p value <0.05 considered as significant.Results
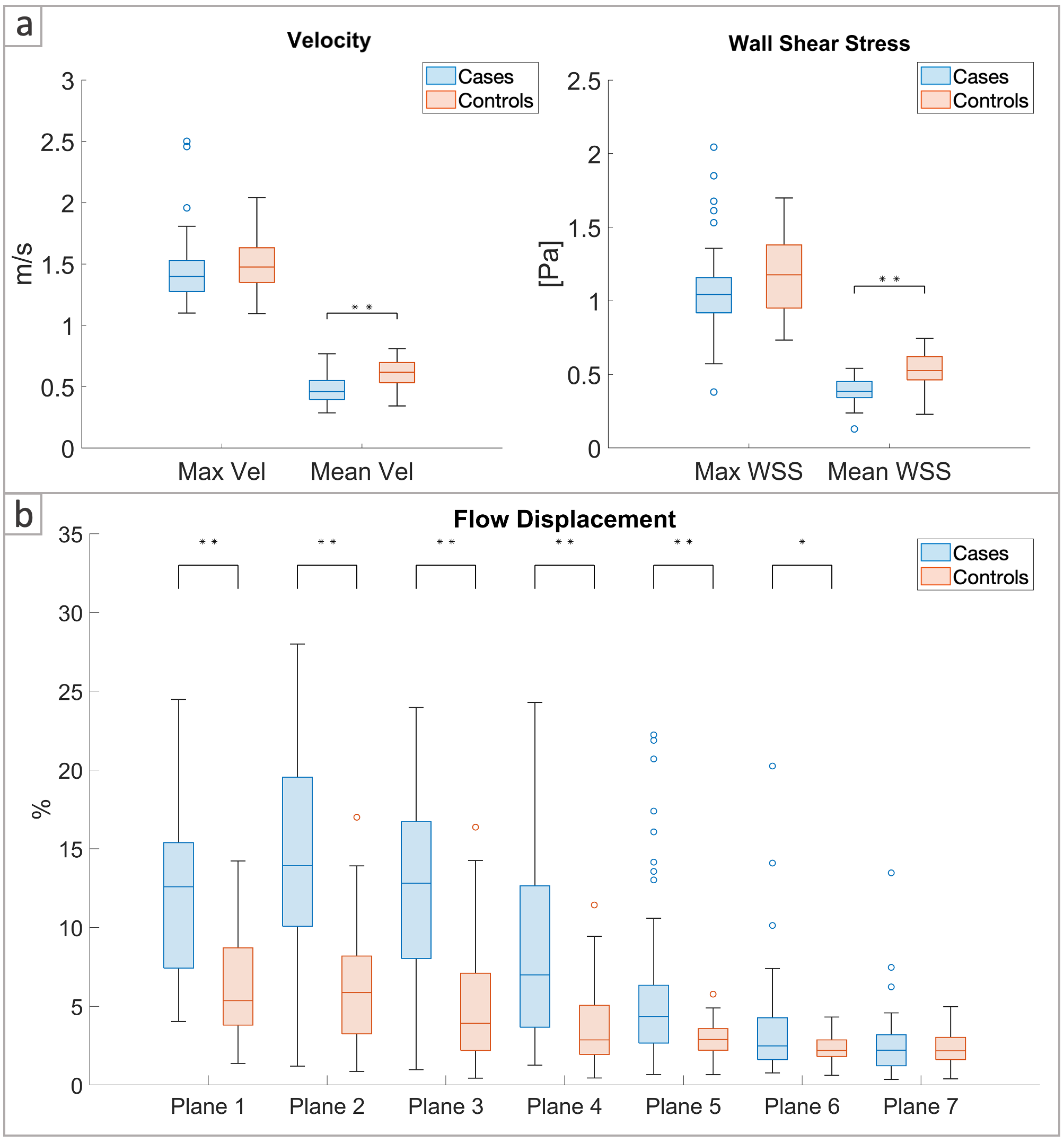
Table 1 reports the demographics and basic hemodynamic parameters for the two groups. Patients had larger maximum and average diameter in the ascending aorta compared to controls (p <0.001). Heart rate, stroke volume and cardiac output did not differ between groups. Velocities and WSS are reported in Figure 2a, and flow displacement values are reported in Figure 2b. Patients had similar maximum velocities and maximum WSS at peak systole compared to controls, but lower average velocities (p <0.001) and average WSS (p <0.001). Also, patients had higher flow displacement in planes 1-6 (p <0.05) and similar flow displacement in the distal ascending aorta (plane 7) at peak systole.Discussion
This study shows that patients with mild-to-moderate ascending aortic dilation and TAV have altered hemodynamics compared to age- and sex-matched controls. Patients had lower average WSS in the ascending aorta, which has been previously associated with aortic growth3. In patients with ascending aortic dilation, the maximum velocity was similar to controls, but flow was more eccentric. In absence of bicuspid aortic valve morphology, aortic stenosis and severe dilation, this eccentric flow may be due to factors such as abnormal cusp opening or the orientation of the left ventricular outflow tract7.Conclusion
This study shows that patients with mild-to-moderate ascending aortic dilation and TAV have altered hemodynamics compared to age- and sex-matched controls. Studying altered hemodynamics in an early stage of aortic disease could improve risk stratification for patients with aortic dilation.Acknowledgements
No acknowledgement found.References
1. Guala, A. et al. Wall Shear Stress Predicts Aortic Dilation in Patients With Bicuspid Aortic Valve. JACC Cardiovasc. Imaging 15, 46–56 (2022).
2. Soulat, G. et al. Association of Regional Wall Shear Stress and Progressive Ascending Aorta Dilation in Bicuspid Aortic Valve. JACC Cardiovasc. Imaging 15, 33–42 (2022).
3. Korpela, T. et al. Flow displacement and decreased wall shear stress might be associated with the growth rate of an ascending aortic dilatation. Eur. J. Cardiothorac. Surg. (2021) doi:10.1093/ejcts/ezab483.
4. Bustamante, M. et al. Automated multi-atlas segmentation of cardiac 4D flow MRI. Med. Image Anal. 49, 128–140 (2018).
5. Potters, W. V., van Ooij, P., Marquering, H., vanBavel, E. & Nederveen, A. J. Volumetric arterial wall shear stress calculation based on cine phase contrast MRI: Volumetric Wall Shear Stress Calculation. J. Magn. Reson. Imaging 41, 505–516 (2015).
6. Sigovan, M., Hope, M. D., Dyverfeldt, P. & Saloner, D. Comparison of four-dimensional flow parameters for quantification of flow eccentricity in the ascending aorta. J. Magn. Reson. Imaging 34, 1226–1230 (2011).
7. Kauhanen, S. P. et al. Aortic dilatation associates with flow displacement and increased circumferential wall shear stress in patients without aortic stenosis: A prospective clinical study. J. Magn. Reson. Imaging 50, 136–145 (2019).
Figures
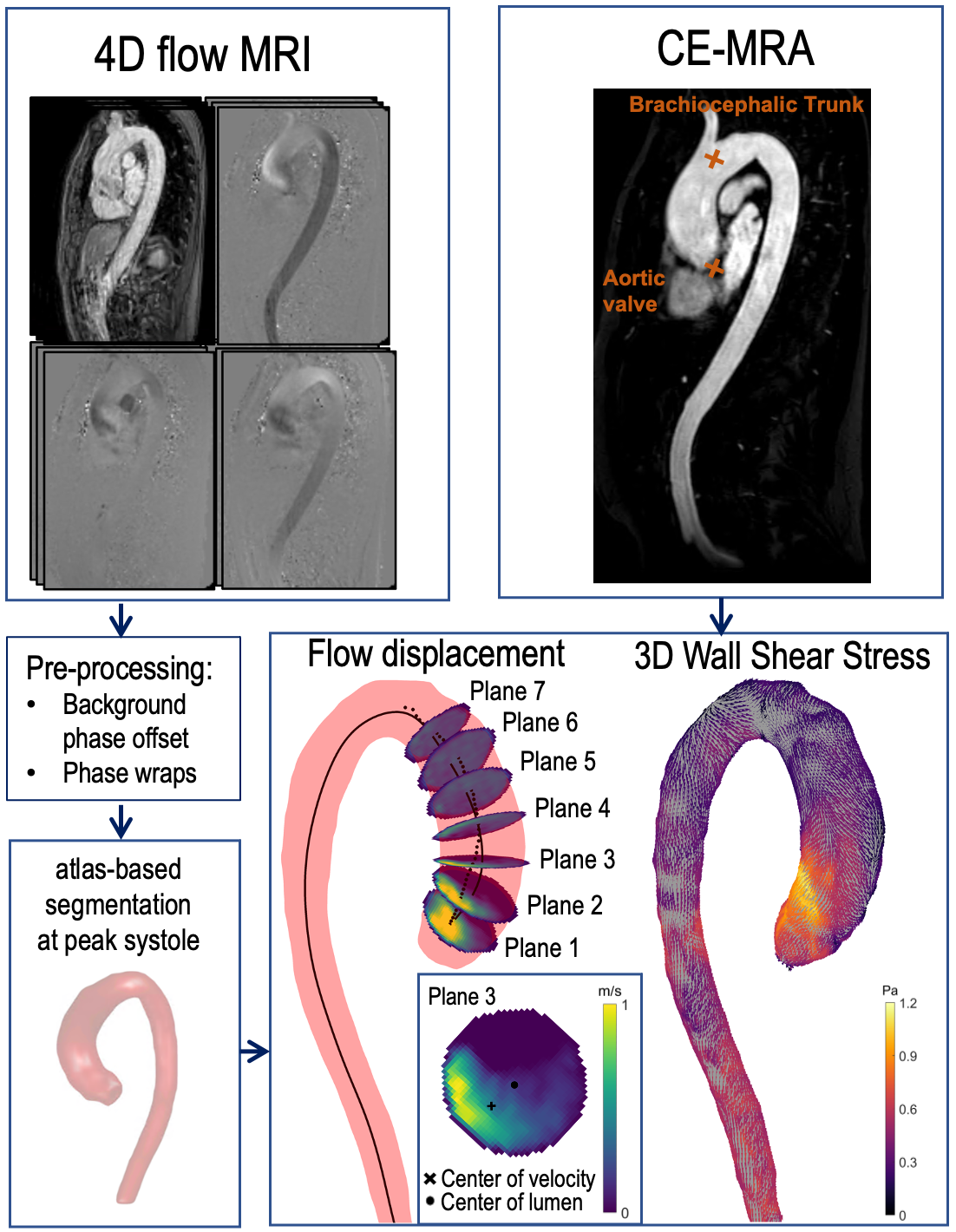
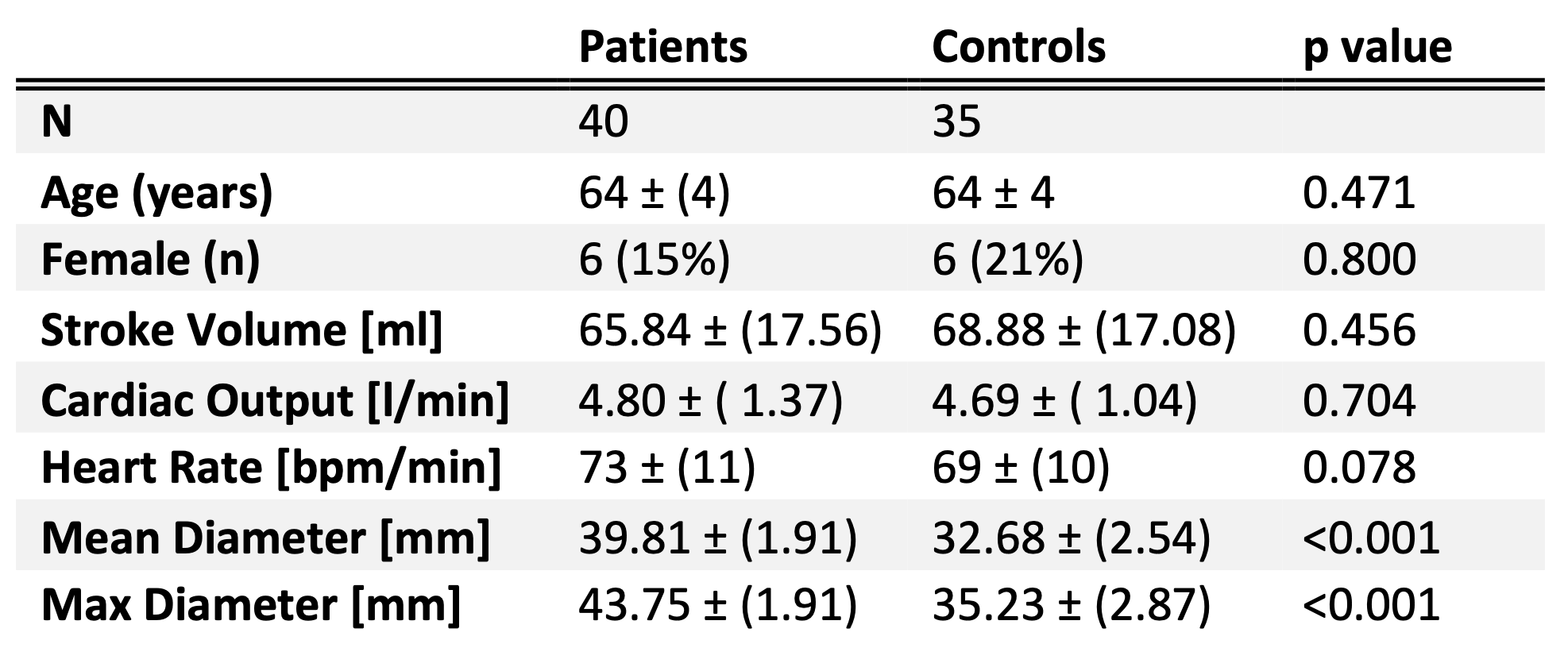
Table 1 Demographics and basic hemodynamic parameters for the two groups.