3729
Can a 38-channel dipolectric antenna array compete with a 32-channel commercial head coil at 7T?
Thomas Dardano1,2, Lijing Xin1,2, and Daniel Wenz1,2
1CIBM Center for Biomedical Imaging, Lausanne, Switzerland, 2Animal Imaging and Technology, Ecole Polytechnique Federale de Lausanne (EPFL), Lausanne, Switzerland
1CIBM Center for Biomedical Imaging, Lausanne, Switzerland, 2Animal Imaging and Technology, Ecole Polytechnique Federale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems
In this work we explore a concept of dipolectric antenna array up to 38 receive channels. We constructed and evaluated an 8-channel version of dipolectric antenna array for human brain MRI at 7T and benchmarked its receive performance against a commercial 1Tx/32Rx head coil. In vivo data obtained for 8-channel array along with simulations (16- and 38-channel) indicate that a 38-channel dipolectric antenna array could provide significantly higher SNR than the current state-of-the-art solutions for human brain at 7T.Introduction
A continuous pursuit for higher SNR in MRI remains valid regardless of the B0 field strength. However, it was arguably ultrahigh field (UHF) which pushed researchers to explore novel RF coil concepts which enabled further receive performance gains. Some of those approaches were particularly promising. For instance, it was demonstrated that dielectric materials, not only in a form of a pad1 but a helmet2 as well, are greatly suitable to increase SNR in human brain at 7T. In general, increasing SNR in the center of human brain can be considered more challenging since it is not expected to be achieved simply by increasing the number of loop coil elements in a receive array3. To address this issue, a 32-channel loop-dipole combined array was developed4. By exploring novel combinations of dielectric structures and dipole antennas, further receive gains are anticipated. Recently, a novel alternative: dipolectric antenna - a combination of a loop-coupled dielectric resonator antenna and a dipole antenna - was introduced5. In this work, we further investigate that approach in multi-channel arrays up to 38-channels and we compare its performance with a standard commercial 32-channel receive-only loop coil array.Methods
Electromagnetic field simulations were performed using Sim4Life (Zurich Medtech, Switzerland). 8-, 16-, and 38-channel dipolectric antenna arrays which were loaded with human voxel model Duke and simulated (Fig.1). For 8- and 16-channel arrays, DRA dimensions were (90x44x5)mm3 and the dipole antenna length was 250 mm. The 38-channel array was composed of 30 cylindrical DRA (diameter=60mm; and 50mm for 8 DRAs at the top of the head; thickness=5mm) and 8 dipole antennas. The geometry of dipole antennas was adjusted to the Duke’s head and were positioned above the cylindrical DRAs. Each DRA had the same electrical properties (εr = 1070, σ=0.2S/m). Scattering parameter matrices were obtained for each array (Fig.1). No additional decoupling strategies were used. The B1- data for each channel were normalized to 0.02 W forward power per channel (2), exported and used for the SNR calculation and optimization (3). An 8-channel dipolectric antenna array was constructed and evaluated at the bench. In vivo MRI experiments using a 7-T head-only MR scanner (Siemens,Germany) were performed in a single subject with the 8-channel dipolectric antenna array and a 1Tx/32Rx commercial RF coil (Nova Medical, USA). B1+ mapping was performed using SA2RAGE6. Two-dimensional (2D) transverse in vivo GRE images (1 mm x 1 mm, slice thickness = 1 mm, TR/TE =1000/3.37 ms, FA = 48°, 192 x 192 matrix) were acquired. Two acquisitions were performed: a standard one and a noise-only (transmit voltage set to 0V) and the data were reconstructed using the Kellman’s approach7 (including B1+ correction) to evaluate in vivo SNR.Results
In simulations, the worst inter-element channel coupling for DRA-DRA was -8.0dB (8-ch), -10.2dB (16-ch), -7.6 and -10.1dB (38-ch) - Fig.1. For dipole-dipole: -6.6dB (8-ch), -6.9dB (16-ch), -9.1 dB (38-ch). For DRA-dipole: -9.5dB (8-ch), -10.6dB (16-ch), -10.5dB (38-ch). SNR was evaluated for each one of the analyzed arrays: in the center of the Duke’s head, the highest SNR was found for 38-ch: from 1.7- to 2.1-fold higher than the one for 8-ch (Fig. 2). An 8-channel dipolectric antenna array was constructed (Fig.3), and to ensure RF safety, B1+ mapping in a spherical phantom was performed observing a very good agreement between the simulations and measurements (Fig.4). When compared with the commercial coil, a peripheral SNR for 8-ch dipolectric array was up to 3-fold higher (Fig.5), but a central SNR was approximately 0-40% lower (along the central horizontal profile – Fig. 5) for the 8-ch dipolectric array. To compensate for imperfections in image overlay a small ROI (Fig.5B) was defined and the difference in SNR was 31.9±13.2% in favor of the commercial coil.Discussion
This study demonstrates for the first time that considerable SNR gains are achievable for a 38-channel dipolectric antenna array for human brain MRI at 7T. An experimental SNR was evaluated for the constructed 8-channel dipolectric antenna array and compared with a commercial 32-channel receive-only array demonstrating significant peripheral SNR gain (up to 3-fold) and a lower central SNR by 31.9±13.2% for a small ROI in the center of the brain (Fig.5B). However, simulations showed that a central SNR for 38-channel array is expected to be 1.7- to 2.1-fold higher than the one for 8-channel dipolectric array. If this gain can be practically realized, it could not only outperform Nova coil but potentially also a 32-channel loop-dipole array which was recently developed by Avdievich et al.4 Unfortunately, due to variations in loading (Duke vs. the subject) and losses which were not included in the simulations (cables, etc.) the results cannot be directly extrapolated. However, the observed differences can be considered significant, and further gains are anticipated by optimizing the DRA’s geometry and electrical properties in the 38-channel array.Acknowledgements
The authors acknowledge access to the facilities and expertise of the CIBM Center for Biomedical Imaging, a Swiss research center of excellence founded and supported by Lausanne University Hospital (CHUV), University of Lausanne (UNIL), Ecole polytechnique fédérale de Lausanne (EPFL), University of Geneva (UNIGE) and Geneva University Hospitals (HUG).References
1. Teeuwisse et al., MRM, 20122. Lakshmanan et al., MRM 2022.
3. Wiggins et al., MRM 2010.
4. Avdievich et al., MRM 2022.
5. Wenz and Xin, ISMRM 2022.
6. Eggenschwiler et al., MRM 2021
7. Kellman et al., MRM 2005.
Figures
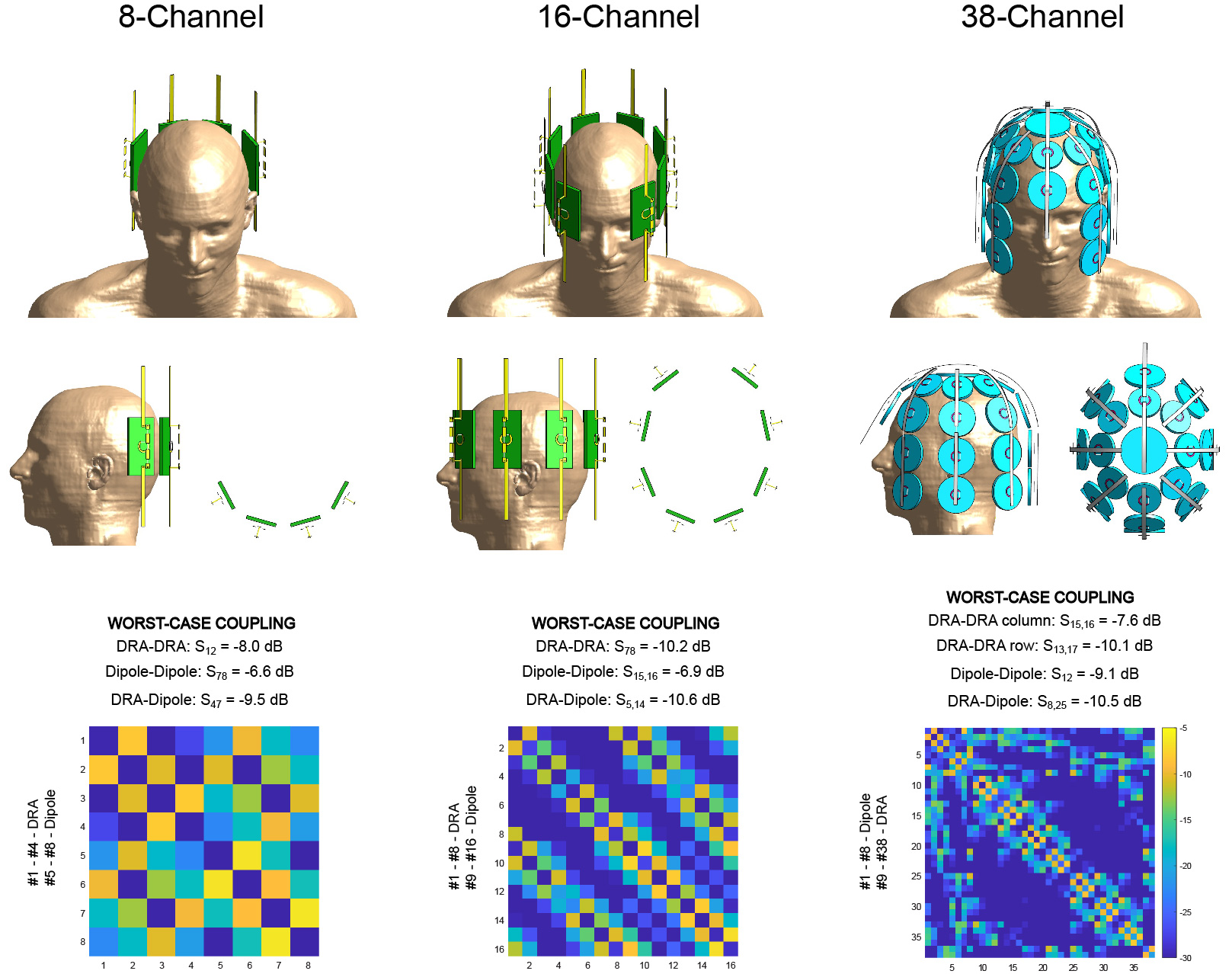
Fig.1. Three
dipolectric antenna arrays which were investigated in our study: 8-, 16-, and
38-channel. 8- and 16-channel were designed using rectangular DRAs while in the
38-channel cylindrical DRAs were used.
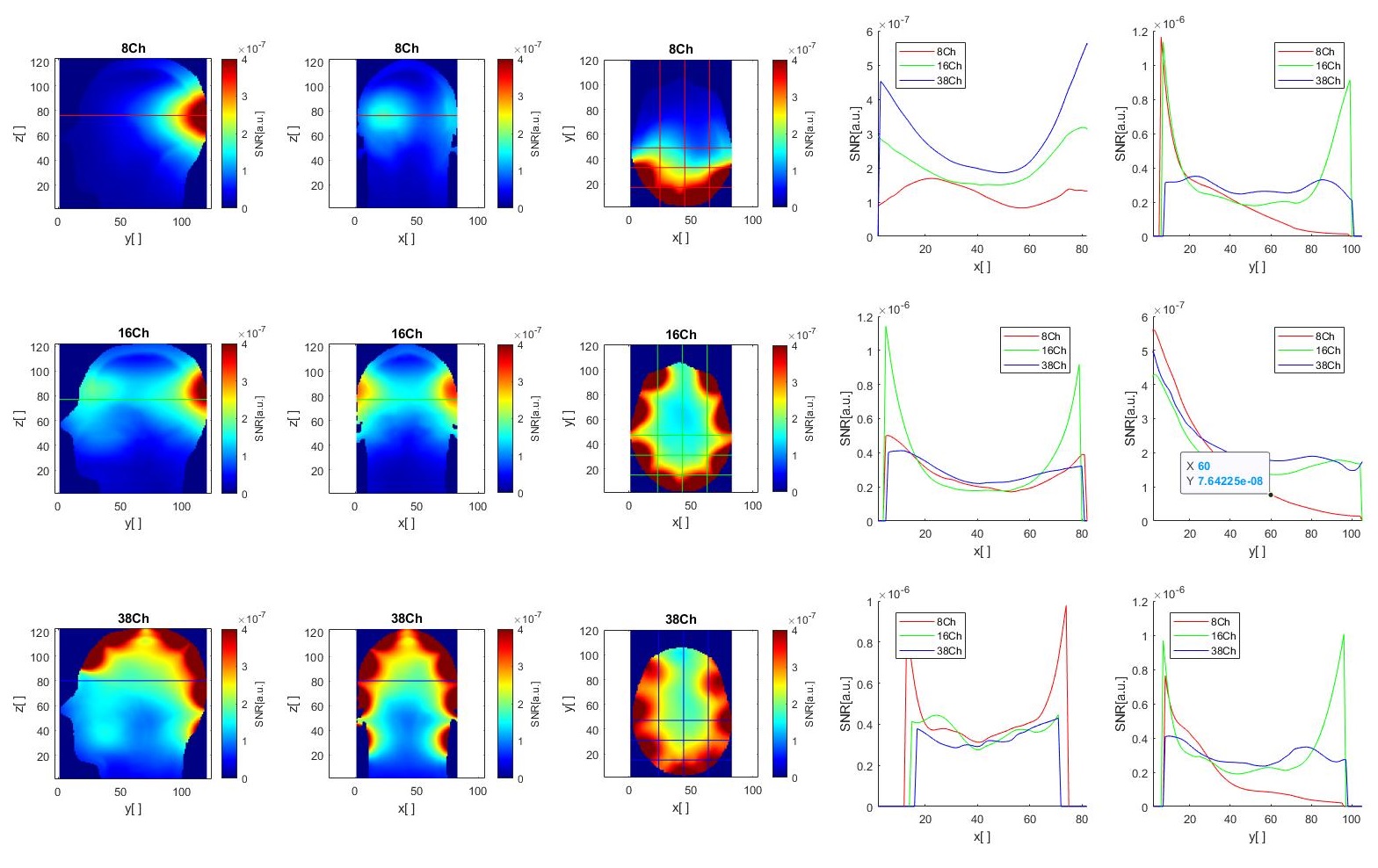
Fig.2. Calculated SNR
for each one of the analyzed dipolectric antenna arrays. It is clear that
16-channel and 38-channel arrays can provide a higher central SNR than 8-channel
array (up to 2.1-fold higher for 38-ch vs. 8-ch).
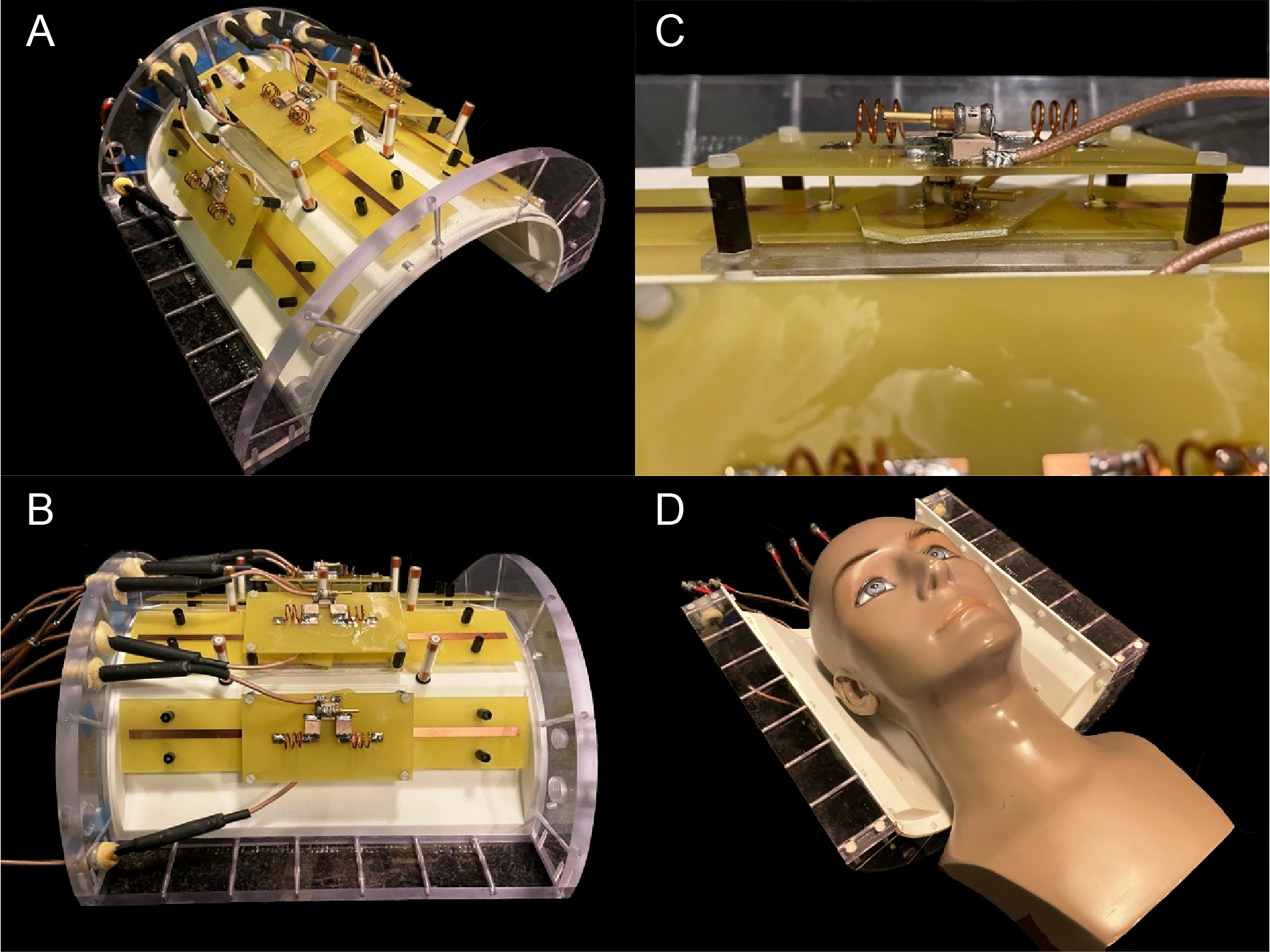
Fig.3. An 8-channel
dipolectric antenna array which was constructed and used in in vivo MRI
experiments.
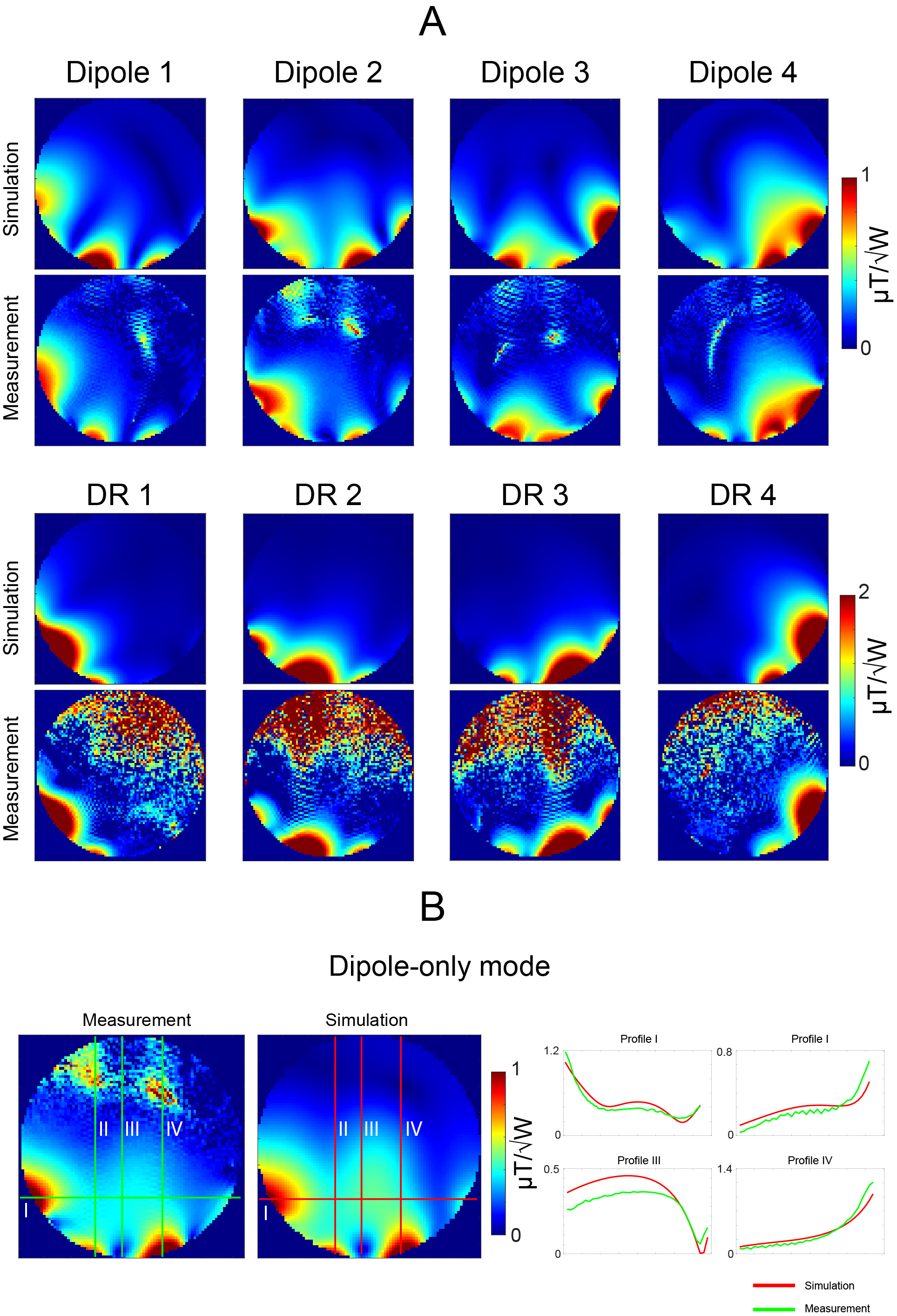
Fig.4. Transmit field
distribution in a spherical phantom: simulations vs. experiments. The data were
acquired using SA2RAGE.
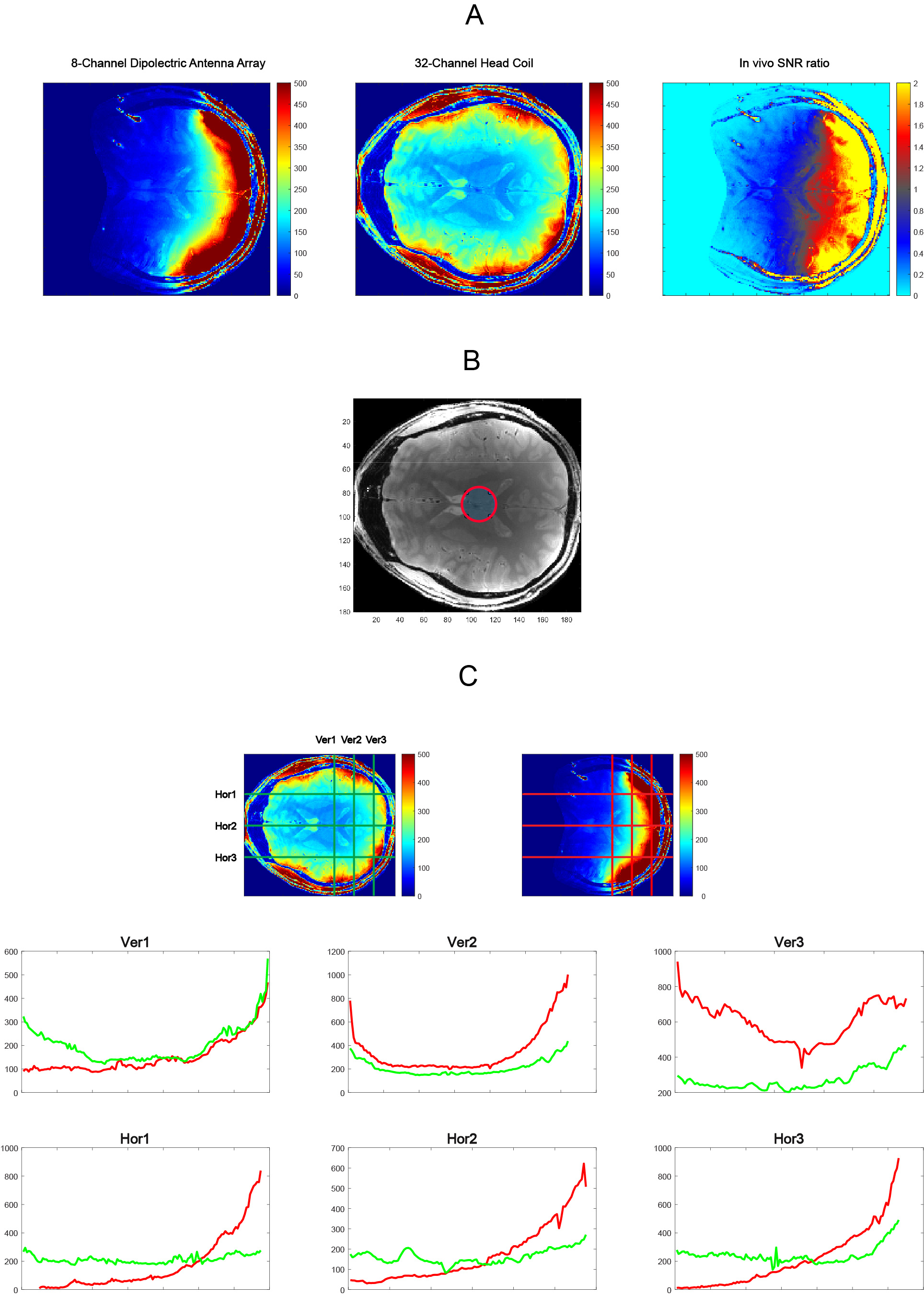
Fig.5. In vivo SNR
comparison: 8-channel dipolectric antenna array vs. a commercial 32-channel array
for human brain MRI at 7T. Ratio maps (A) show that 8-channel dipolectric
antenna array provided approximately up to 3-fold higher peripheral SNR and up
to 40% lower central SNR. Addtionally, SNR difference in % was estimated for a
small ROI: 31.9±13.2% (B) and along different horizontal (Hor) and vertical
(Ver) profiles.
DOI: https://doi.org/10.58530/2023/3729