3659
Accelerated phase-contrast for diastolic function evaluation using k-t PCA methods1Department of Biomedical Engineering, Yale University, New Haven, CT, United States, 2Department of Radiology and Biomedical Imaging, Yale University, New Haven, CT, United States
Synopsis
Keywords: Flow, Quantitative Imaging
Diastolic function evaluation requires estimates of early and late diastolic mitral valve flow velocities (E and A), normally evaluated by echocardiography, using phase contrast (PC). Our goal was to investigate k-t principal component analysis (PCA), constrained by either global and local principal components, for E and A measurements. Importantly, we found that retaining the central k-space used in estimating the principal components improved the final velocity maps. We compared local PCA with global PCA. Retrospectively undersampled images showed strong agreement with standard PC acquisitions. Higher E and A were observed using higher temporal resolution in prospective k-t PCA PC acquisitions.Introduction
Blood flow velocity during filling of the left ventricular (LV) has peaks in early diastole (E wave) and in late diastole (caused by atrial contraction, aka A wave). E/A is a marker of the LV diastolic function1. Though clinically assessed by transthoracic echocardiography (TTE), E and A can be measured with good reproducibility by cardiovascular MR phase-contrast (PC) techniques and validated to have strong relationship with TTE2,3. Since in PC two acquisitions are executed (reference and flow-encoded), standard PC MR techniques have limited temporal resolution, so acceleration is important. K-t PCA (principal component analysis)4 is an established way to accelerate MRI time series, with extensive development of compartment-based or locally low rank methods5,6 for high image acceleration. Our goal was to study k-t PCA’s performance in LV blood inflow PC measurement, comparing global and simple compartment-based k-t PCA methods.Methods
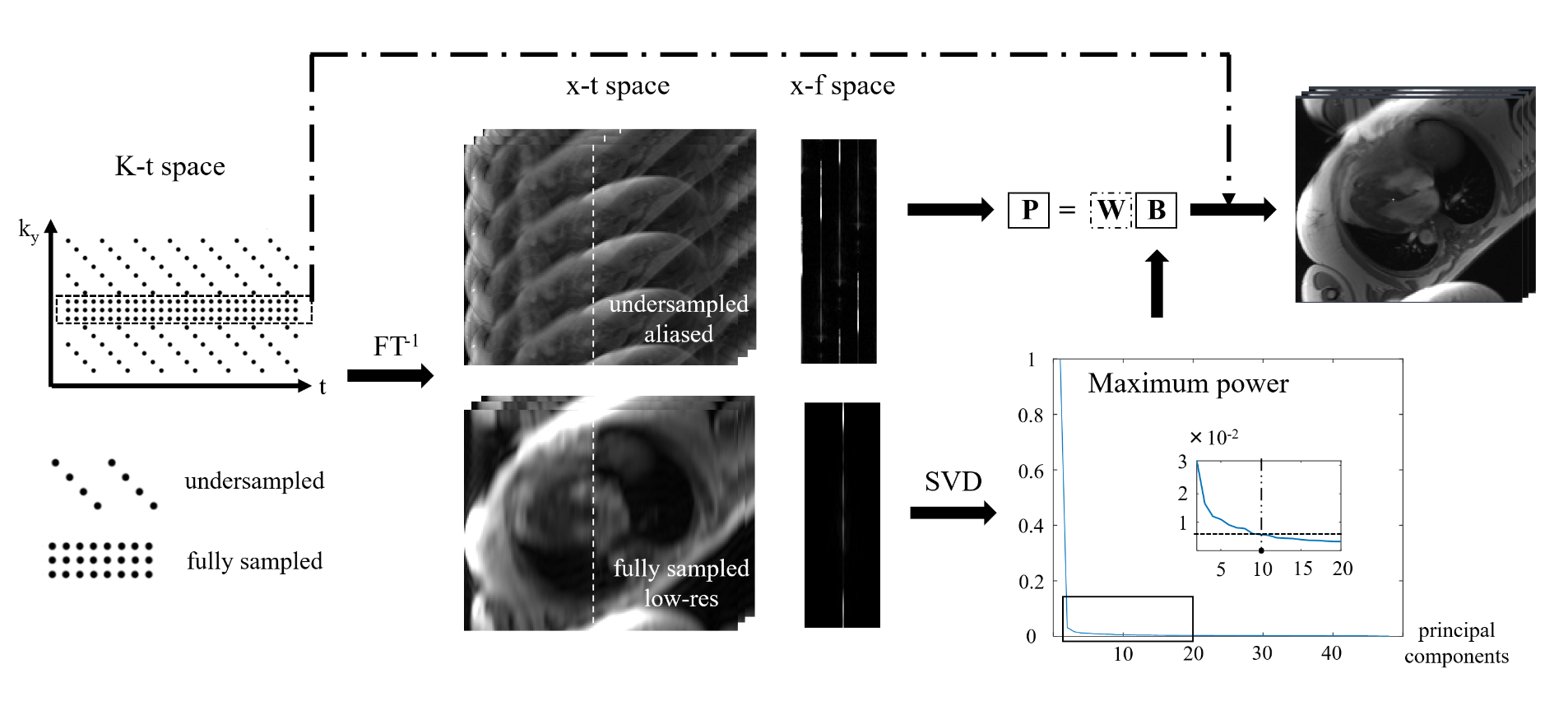
Reconstruction: The k-t PCA method described by Pedersen et al4 was implemented in Matlab (diagram shown in Figure 1). Central k-space was used to generate the principal components in x-f space (i.e., B, both global and compartment-based). The number of components used for reconstruction was set as Nphases/4 - 2. Weighting coefficients W were then estimated using B and the aliased x-f data P from undersampled k-space. Once determined, the W were used to obtain the unaliased high-resolution x-f. Importantly, the recovered full images and k-space were constrained (smoothed) to match the PCAs in the temporal domain, but temporal information is critical for measurement of E and A. We therefore retained the acquired central k-space used in estimating the PCAs and substituted it for the synthesized central k-space.Imaging: All studies were performed on a Siemens 3T scanner. The studies were IRB approved and all subjects provided written informed consent. Scan parameters for conventional PC flow were: 2D Cartesian GRE with ECG retrospectively gated, TR/TE/ q= 4.7ms/2.5ms/15°, 192 matrix, 380mm FOV, 75% phase, 8mm slice thickness, 150cm/s VENC in readout direction, strong asymmetric echo, 2 or 4 views per segment (Nvps, with temporal resolution of 18.8ms or 37.6ms respectively). GRAPPA with acceleration factor R = 2, 24 reference lines. The prospectively and retrospectively undersampled K-t PCA PC acquisitions used the same parameters, with R = 4, and 16 reference lines (see Figure 1 for the sampling pattern of k-t PCA).
Analysis: We first compared standard PC acquisitions with different temporal resolutions, which then served as gold standard to test the accuracy of E and A from the retrospectively undersampled k-t PCA reconstructions. Prospective k-t PCA were performed and compared to the standard PC with similar acquisition time but lower temporal resolution. Finally, the effects of global and different local constraints, retained central k-space, on the k-t PCA reconstruction were investigated.
Results
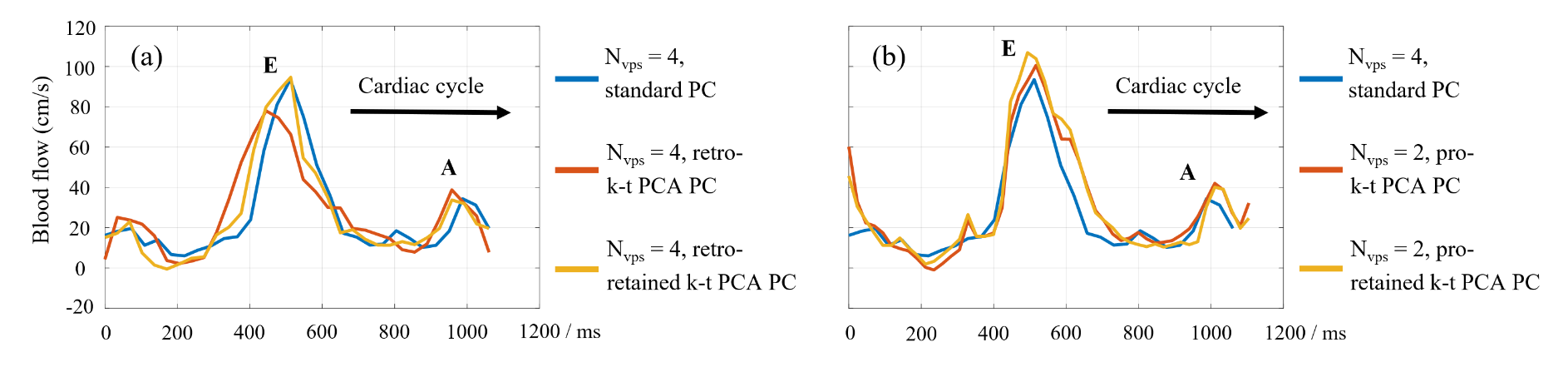
Figure 2 compares standard PC using a long breath-hold (Nvps = 2, 36 heartbeats) and standard breath-hold (Nvps = 4, 18 heartbeats) to a retrospectively undersampled k-t PCA. Images (magnitude and phase) and velocity curves are compared. Improved temporal resolution increased the measured E and A velocities, on the standard PC. K-t PCA was able to recover the accurate velocity waveform, matching high temporal resolution PC. The performance of k-t PCA was improved by retaining the original central k-space information, after k-t PCA processing. However, there appears to be some inconsistency between originally acquired k-space and prospectively accelerated k-t PCA generated k-space, which manifest as focal errors in the phase maps (Figure 1a).With lower temporal resolution (Nvps = 4 and <30 frames, Figure 3a) retrospectively undersampled k-t PCA PC reconstruction exhibited large differences from standard PC, because fewer time frames were acquired, which limited the principal components that could be used. However, when central k-space was retained, this recovered the fidelity of the flow waveform, for both E and A (E: 94.7 vs. 93.6, A: 33.8 vs. 34.4 cm/s compared to standard PC).
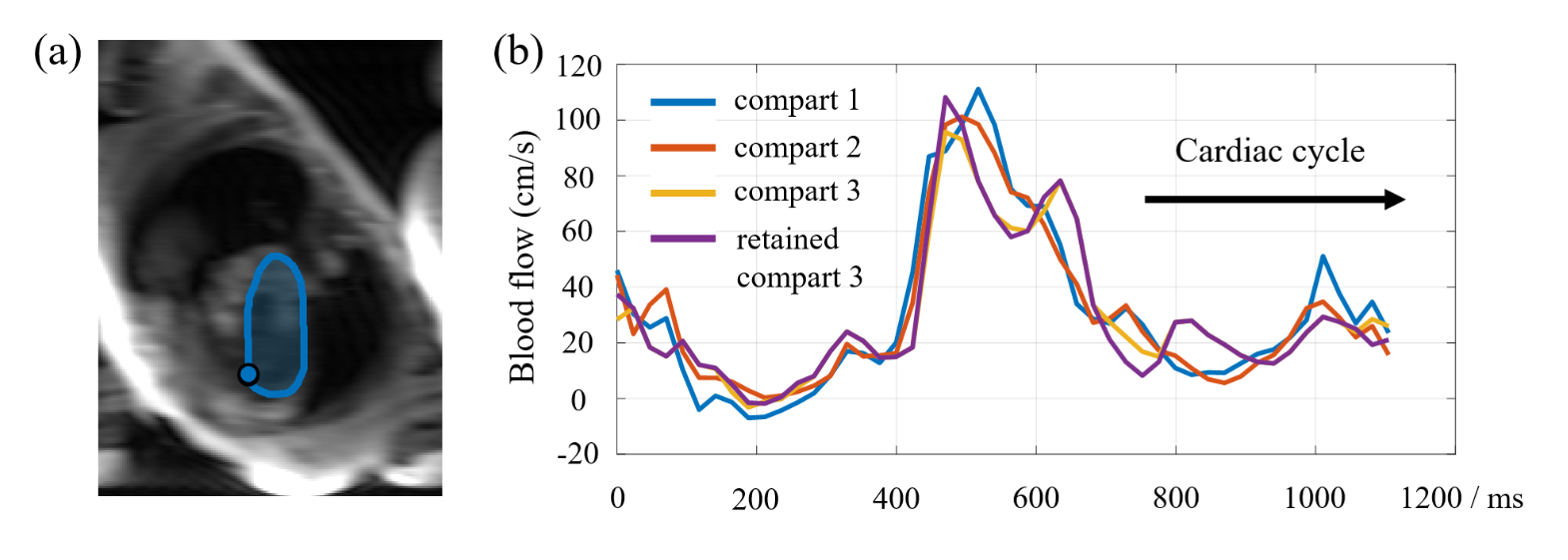
We prospectively acquired k-t PCA PC data, with Nvps = 2, shown in Figure 3b. The peak velocities were both higher than standard PC with Nvps = 4. This may due to the higher temporal resolution, which was consistent with Figure 2b. We also analyzed the use of compartment-based k-t PCA using manually drawn compartments within the left ventricle (see ROIs in Figure 4a). This processing made the velocity waveforms depend on the ROI, making it less reproducible.
Discussion
We explored the potential of k-t PCA PC for left ventricular blood inflow measurement, obtaining peak velocities in early and late diastole (E and A). In vivo experiments showed the high temporal resolution was needed to sample the peak velocities, which could be achieved using highly undersampled k-t PCA PC. Importantly, a new finding is that retaining acquired central k-space after k-t PCA processing helped recover accurate blood velocities; this was explicitly not used in prior early studies4,5. Compartment-based k-t PCA was not useful in our study, compared to prior studies which showed success in aortic PC measurement5.Conclusion
For velocity measurements of E and A, global k-t PCA (retaining central k-space data) showed strong agreement to the standard approach, but with higher acceleration factor, permitting high temporal resolution in a feasible breath-hold.Acknowledgements
No acknowledgement found.References
[1] Galderisi M. Diastolic dysfunction and diastolic heart failure: diagnostic, prognostic and therapeutic aspects. Cardiovasc Ultrasound. 2005;3:9. Published 2005 Apr 4.
[2] Seemann F, Baldassarre LA, Llanos-Chea F, et al. Assessment of diastolic function and atrial remodeling by MRI - validation and correlation with echocardiography and filling pressure. Physiol Rep. 2018;6(17):e13828.
[3] Bollache E, Redheuil A, Clément-Guinaudeau S, et al. Automated left ventricular diastolic function evaluation from phase-contrast cardiovascular magnetic resonance and comparison with Doppler echocardiography. J Cardiovasc Magn Reson. 2010;12(1):63. Published 2010 Nov 9.
[4] Pedersen H, Kozerke S, Ringgaard S, Nehrke K, Kim WY. k-t PCA: temporally constrained k-t BLAST reconstruction using principal component analysis. Magn Reson Med. 2009;62(3):706-716.
[5] Giese D, Schaeffter T, Kozerke S. Highly undersampled phase-contrast flow measurements using compartment-based k-t principal component analysis. Magn Reson Med. 2013;69(2):434-443.
[6] Zhang T, Pauly JM, Levesque IR. Accelerating parameter mapping with a locally low rank constraint. Magn Reson Med. 2015;73(2):655-661.
Figures