3628
Value of mDIXON-Quant mDixon-Quant sequence Imaging in Evaluation of Renal Function Damage in Patients with Liver Cirrhosis
Yue Wang1, Ye Ju1, Nan Wang1, and Ailian Liu1
1the First Affiliated Hospital of Dalian Medical University, Dalian, China
1the First Affiliated Hospital of Dalian Medical University, Dalian, China
Synopsis
Keywords: Kidney, Liver
Patients with liver cirrhosis are easy to be complicated with renal function injury, and symptoms of early renal injury are hidden and often difficult to be detected in time, which may ultimately lead to poor prognosis. mDixon-Quant imaging, a novel fat quantitative MRI technique was used to evaluate the degree of renal function injury in patients with cirrhosis. Results showed that mDixon-Quant imaging can be an effective method for noninvasive diagnosis and early assessment of renal function injury in liver cirrhosis.Introduction
Patients with liver cirrhosis are at high risk of renal impairment due to circulatory disorders and other factors, ultimately leading to high morbidity and mortality. The symptoms of renal injury in the early stage of the disease are often not obvious, and the commonly used clinical indicators of renal function, such as serum creatinine, lack sensitivity; while the gold standard renal biopsy is invasive and prone to complications. Therefore, it is necessary to find a sensitive and effective way to diagnose early renal injury in patients. mDixon-Quant is a novel MRI technology with the characteristics of efficient acquisition speed, excellent water-fat separation accuracy and reliable quantification of fat fraction (FF) and apparent relaxation rate (R2*). mDixon-Quant has been widely used in the study of fat quantification in the liver [1], bone and joint [2] systems. In this study, we aimed to evaluate the efficiency of mDixon-Quant imaging for quantitative assessment of renal impairment in patients with cirrhosis.Methods
A total of 21 patients with liver cirrhosis who underwent 3.0T magnetic resonance scanner (Ingenia CX, Philips Healthcare, Best, the Netherland) in our hospital from August 2019 to October 2022 were retrospectively reviewed. The MR scans included conventional abdominal MR examination and mDixon-Quant imaing (detailed parameters are shown in Table 1). According to the Child-Pugh classification of liver function, the patients were divided into the compensated cirrhosis group (Child-Pugh grade A, group A, 11 cases, mean age: 56.55±8.37, age range: 46-72 years; 4 women) and the decompensated cirrhosis group (Child-Pugh grade B and C, group B, 10 cases, mean age: 61.80±10.49, ranged 49-85 years, 4 women). Twenty-nine healthy volunteers (group C, mean age: 56.19±14.01, ranged 26-79 years, 21 women) were collected as control group. All the original images were imported into the workstation quantitative measurements by two radiologists (7 and 2 years experiences in abdominal imaging diagnosis, respectively). Oval ROIs were placed the upper pole, middle pole and lower pole of the right kidney at both cortex and medulla, respectively, and the R2* and FF values were measured (Fig. 1). Intra-class correlation coefficient (ICC) was used to test the inter-observer agreement. Analysis of variance (ANOVA) test was used to test the differences among the three groups. Shapiro-Wilk test was used to test the normality of data, and Mann-Whitney U test was used to compare the differences between the two groups according to the normality of data. Binary Logistic regression and receiver operating characteristic curve (ROC) were used to analyze the diagnostic efficacy of each single parameter and their combination. Delong test was used to compare the difference between each AUC value, and P < 0.05 was considered statistically significant.Results
The inter-observer agreement was good (ICC>0.75). ANOVA test showed that the cortical FF, medullary FF and cortical R2* value had significant differences among the three groups (P<0.05), while the medullary R2* value had no significant difference among groups (P>0.05). The cortical FF value [2.20 (0.52, 2.65) vs 0.54 (0.47, 0.77) %, P = 0.015), medulla FF value [1.43 (0.90, 2.76) vs 0.56 (0.42, 0.89) %, P < 0.001) and cortical R2* value [19.58 (17.45, 26.70) vs15.52 (14.13, 17.95)/s, P = 0.003) of group A were significantly higher than those of group C; The cortical R2 * value [18.57 (17.30, 20.02) vs 15.52 (14.13, 17.95)/s, P = 0.006) and the medulla FF value [1.31 (0.46, 1.96) vs0.56 (0.42, 0.89)/s, P=0.040] of group B were significantly higher than those in group C (Table 2). The sensitivity, specificity and area under curve (AUC) of each parameter are shown in Table 3. The AUC of the combination of cortical FF, medullary FF and cortical R2* values in differentiating group A from group C was higher than that of any single parameter. The combined diagnostic parameters of medullary FF and cortical R2* values had the highest AUC value in differentiating group B and group C (Figures 2 and 3).Discussion
The imbalance of endogenous vasoactive substances and secondary neurohumoral regulation in patients with liver cirrhosis led to vasospasm and contraction of renal vessels, that can lead to reduced blood perfusion in renal cortex. In addition, the function of the Na+ pump in the proximal medullary tubule can be reduced during renal injury, subsequently the reduced oxygen consumption and the increased oxygenation. As a result, no significant difference in the medullary R2* value was observed among the three groups. On the other hand, there were lipid metabolism disorders and lipid deposition in the kidney during renal damage, so the cortical and medullary FF values of group A and the medullary FF values of group B were higher than those of group C. In addition, the renal medulla is mainly composed of renal tubules and collecting ducts, so renal tubular fibrosis mainly occurs in the medulla. With the increased degree of renal fibrosis, renal lipid content will decrease. So there is no significant difference in cortical FF value between groups B and C.Conclusion
mDixon-Quant can be used as a non-invasive, sensitive and effective method to assess early renal function damage in patients with liver cirrhosis, which has certain significance for clinical decision-making, early intervention of the disease and improvement of prognosis.Acknowledgements
None.References
1.Zhang Y, Wang C, Duanmu Y, Zhang C, Zhao W, Wang L, Cheng X, Veronese N, Guglielmi G. Comparison of CT and magnetic resonance mDixon-Quant sequence in the diagnosis of mild hepatic steatosis. Br J Radiol. 2018 Nov;91(1091):20170587. doi: 10.1259/bjr.20170587. Epub 2018 Jul 20. PMID: 30028193; PMCID: PMC6475942.2.Li J, Wang Y, Zhang X, Zhang P, Su Y, Bai L, Wang Y, Wang M, Zhao J. Associations of muscle size and fatty infiltration with bone mineral density of the proximal femur bone. Front Endocrinol (Lausanne). 2022 Sep 27;13:990487. doi: 10.3389/fendo.2022.990487. PMID: 36237187; PMCID: PMC9552015.3.Gupta K, Bhurwal A, Law C, Ventre S, Minacapelli CD, Kabaria S, Li Y, Tait C, Catalano C, Rustgi VK. Acute kidney injury and hepatorenal syndrome in cirrhosis. World J Gastroenterol. 2021 Jul 14;27(26):3984-4003. doi: 10.3748/wjg.v27.i26.3984. PMID: 34326609; PMCID: PMC8311533.Figures
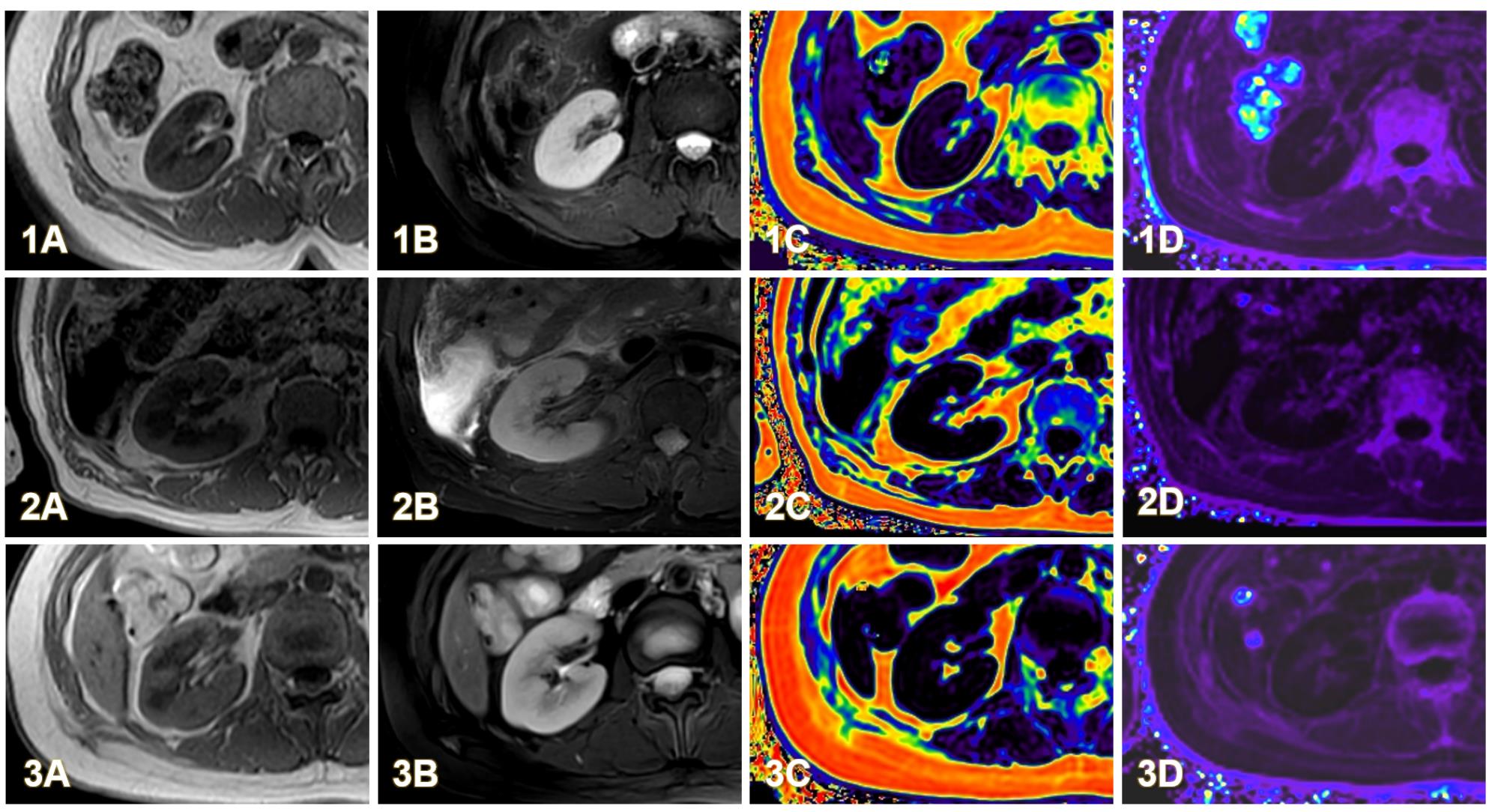
Figure 1. A 62-year-old female with compensated cirrhosis (group A). T1WI (1A), T2WI (1B), FF (1C), and R2* (1D) images. A 63-year-old female with decompensated cirrhosis (group B). T1WI (2A), T2WI (2B), FF (2C), and R2* (2D) images.A 26-year-old female, healthy volunteer (group C). T1WI (3A), T2WI (3B), FF (3C), and R2* (3D) images.
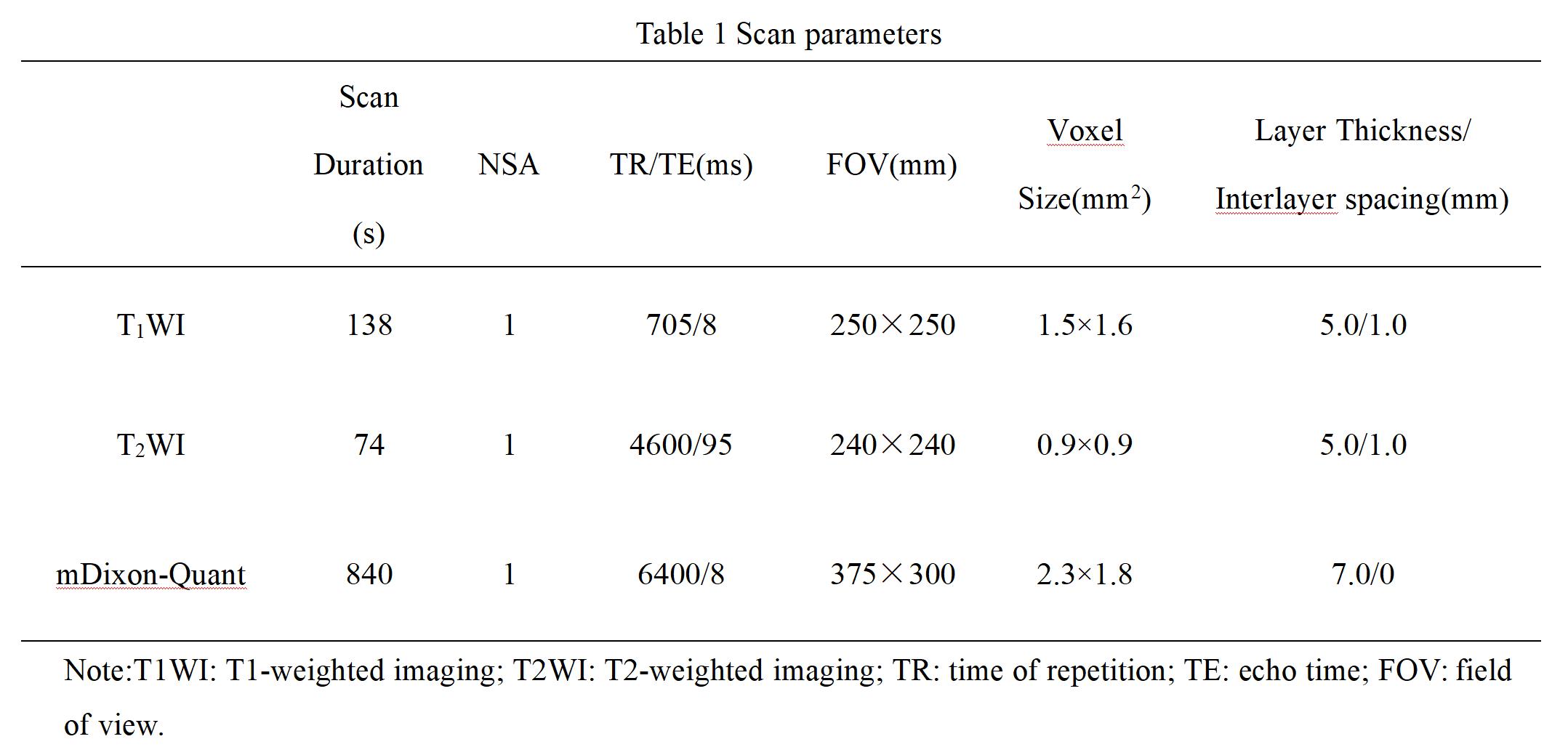
Table 1 Scan parameters
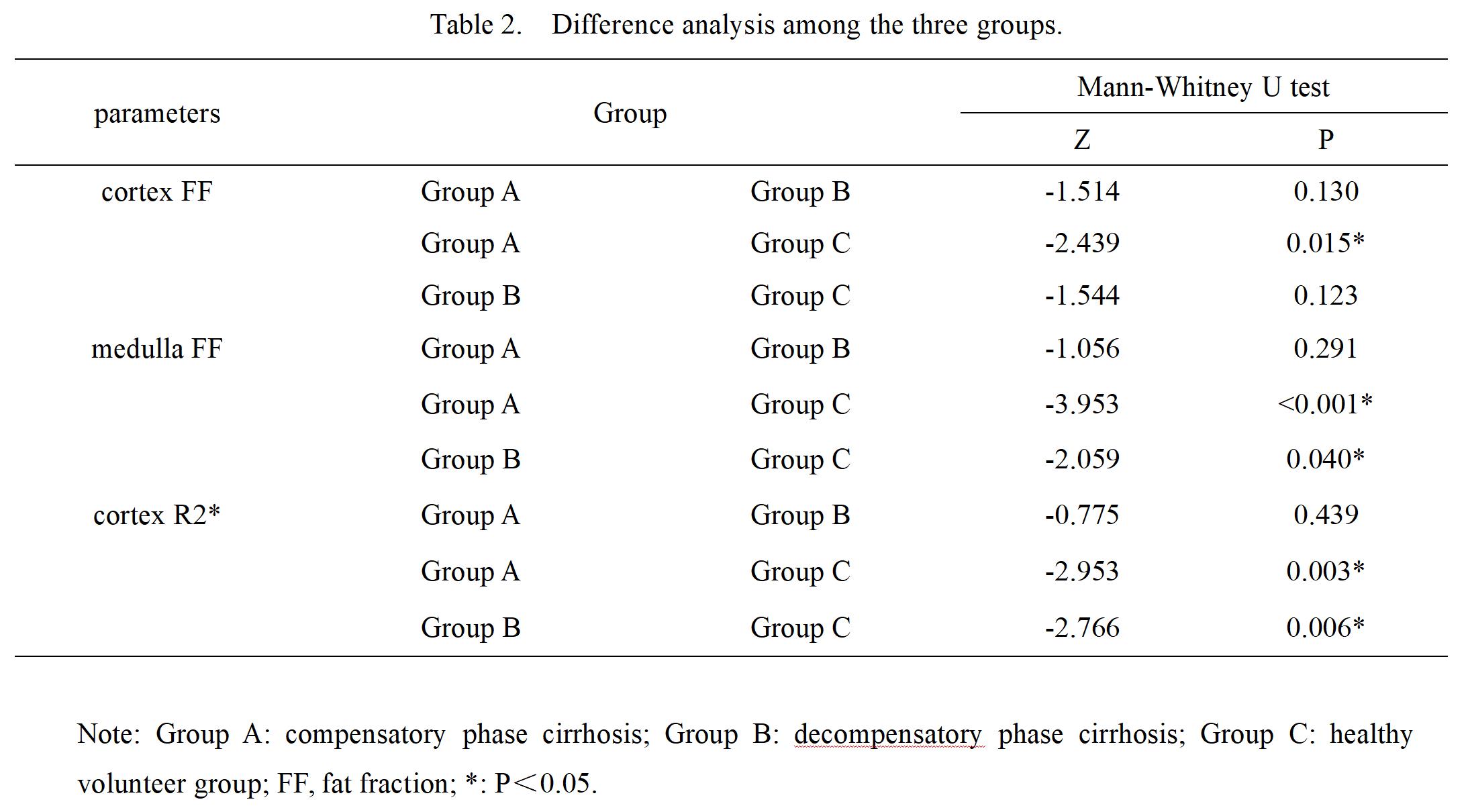
Table 2. Difference analysis among the three groups.
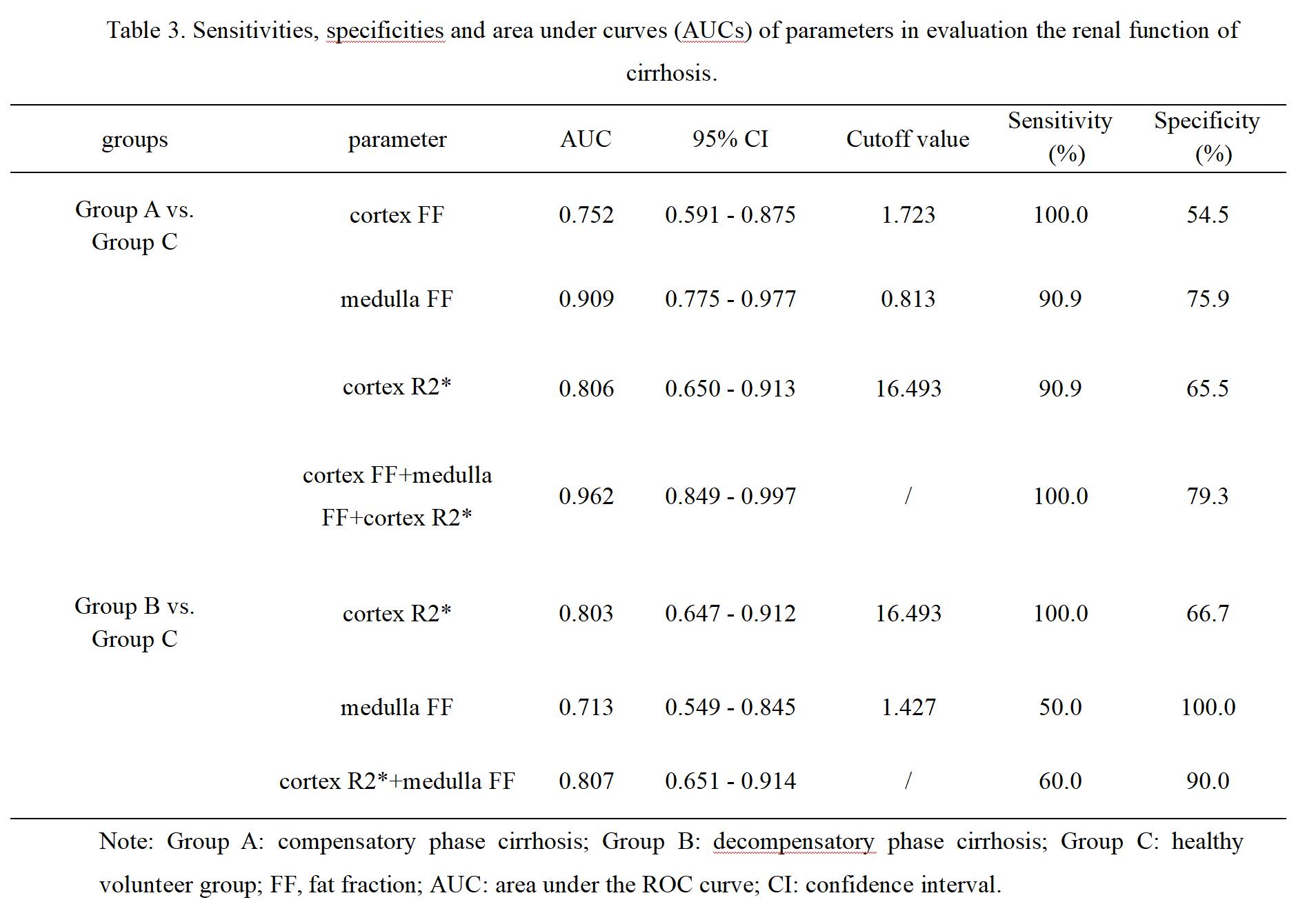
Table 3. Sensitivities, specificities and area under curves (AUCs) of parameters in evaluation the renal function of cirrhosis.
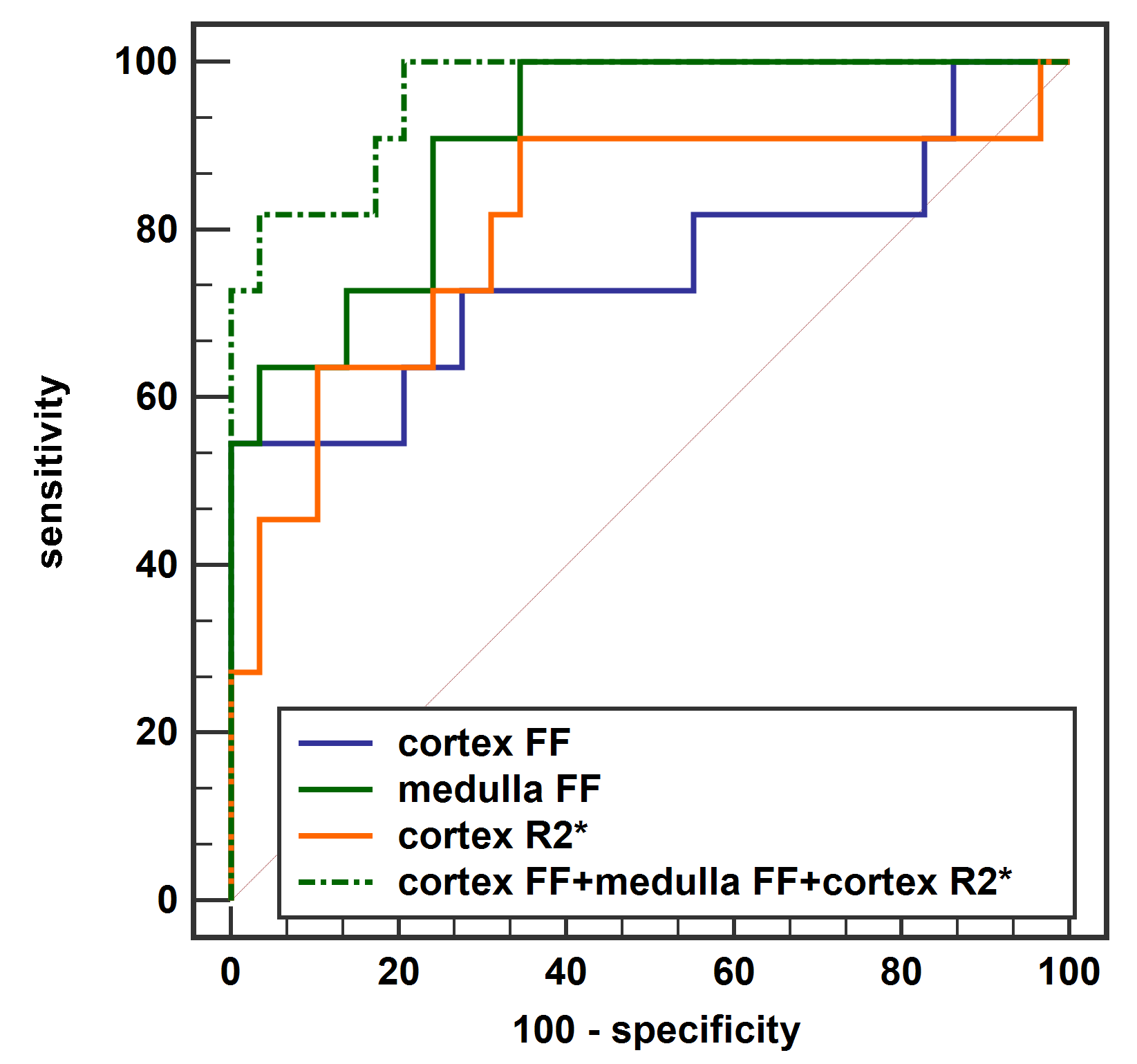
Figure 2. ROC curves showed performance of cortex FF, medulla FF and cortex R2* and their combination to differentiate between compensatory phase cirrhosis group and healthy control group.
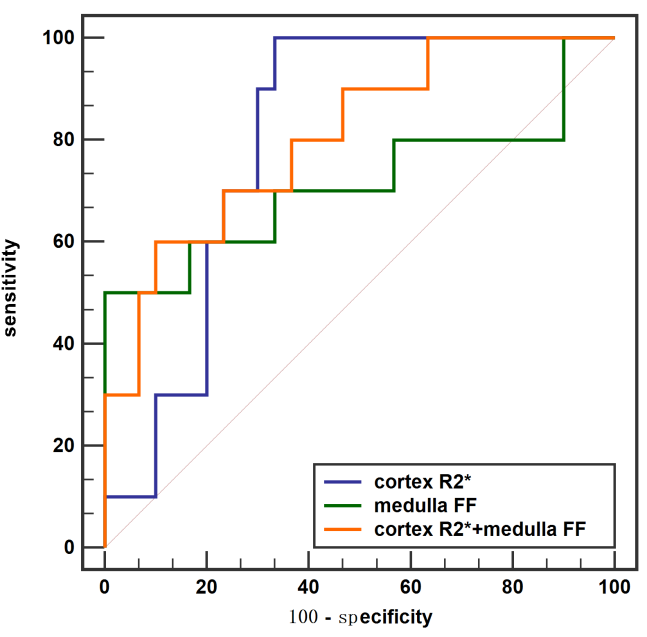
Figure 3. ROC curves showed performance of cortex R2*and medulla FF and their combination to differentiate between decompensatory phase cirrhosis group and healthy control group.
DOI: https://doi.org/10.58530/2023/3628