3478
BPAS-MRI combined with MRA to identify intracranial vertebrobasilar lesions1XI'AN INTERNATIONAL MEDICAL CENTER HOSPITAL, Xi'an, China, 2Philips Healthcare, Xi'an, China
Synopsis
Keywords: Blood vessels, Blood vessels
Basi-parallel anatomic scanning magnetic resonance imaging (BPAS-MRI) is an MRI technique that can reveal the outer contour of the vertebrobasilar artery, even in the presence of occlusion. A total of 53 patients with 106 segments of blood vessels were scanned by BPAS+MRA, and the results were verified by comparing with VW-MRI. It was found that BPAS+MRA could significantly improve the detection rate of vertebrobasilar lesions, which was of great value for the diagnosis and differential diagnosis of arterial dysplasia, arteriosclerosis and arterial occlusion, and could improve the diagnostic confidence of radiologists.Introduction
Basi-parallel anatomic scanning magnetic resonance imaging (BPAS-MRI) is a kind of heavy T2-weighted MRI sequence, which can clearly show the surface anatomical contour of intracranial vertebrobasilar artery (vessel external diameter)[1,2]. Time-of-flight magnetic resonance angiography (TOF-MRA) is commonly a routine MRI sequence used as non-invasive substitute for DSA for intracranial vertebrobasilar imaging and assessment. TOF-MRA can only show the inner diameter of blood vessels with blood flow. Limited by its imaging principle, it cannot show the occlusion of blood vessels without blood flow, and cannot identify the cause of vascular stenosis[3]. BPAS can be used for the differential diagnosis of intracranial vertebrobasilar artery lesions, to distinguish the slender or occluded vessels from congenital or acquired, due to congenital dysplasia, arteriosclerosis or dissection occlusion[4]. The purpose of this study is to verify the advantages of using BPAS-MRI combined with TOF-MRA to identify intracranial vertebrobasilar artery lesions.Material and Methods
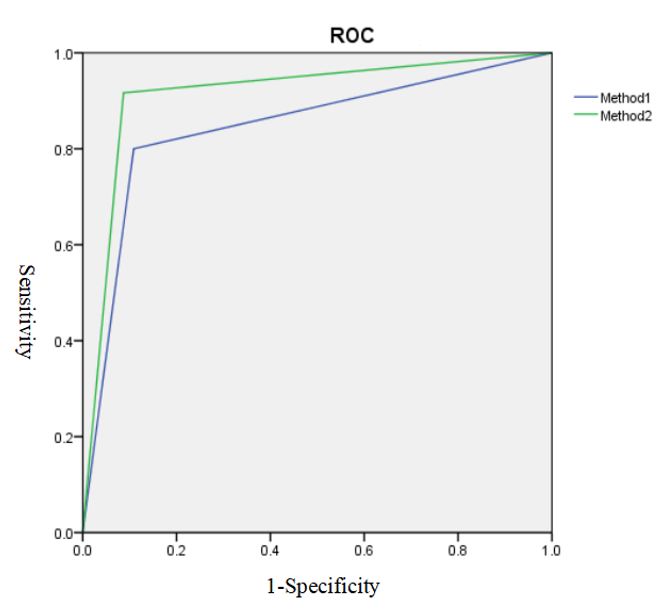
A total of 53 patients with headache and dizziness who underwent MRA examination and BPAS examination in our hospital from January 2021 to October 2021 were retrospectively analyzed. All patients underwent MR examination on a 3.0T MR scanner (Ingenia, Philips, the Netherlands) using 20 channel head-neck coil. The imaging parameters suitable for BPAS on 3.0T-MR were explored by radiologists and radiographer from departments of medical imaging, Xi’an international medical center hospital. At the same time, these patients had high-resolution vessel wall (vw)-MR imaging within 2 weeks as the interpretation standard. We counted the vertebral artery and basilar artery lesions separately. A total of 106 segment vessels were finally found. The MRA and MRA+BPAS images of 106 segments of blood vessels were reviewed by two experienced radiologists (with 5 and 8 years of diagnosis experiences) who were unaware of the patient's VV-MR results. First the presence or absence of vascular lesions was determined. Then the diseased vessels were divided into three suspected diagnoses: arteriosclerosis, dysplasia and vascular occlusion. Receiver Operating Characteristic (ROC) curves were performed by the diagnostic results, and the diagnostic confidence of doctors using the two methods was divided into four grades (Grade 1-very positive, grade 2-positive, grade 3 -not sure, and grade 4 -uncertain). Poor diagnostic confidence was defined as a score of 3 or higher. The consistency of diagnosis results of 2 observers were analyzed by calculating interclass correlation coefficient (ICC).Results
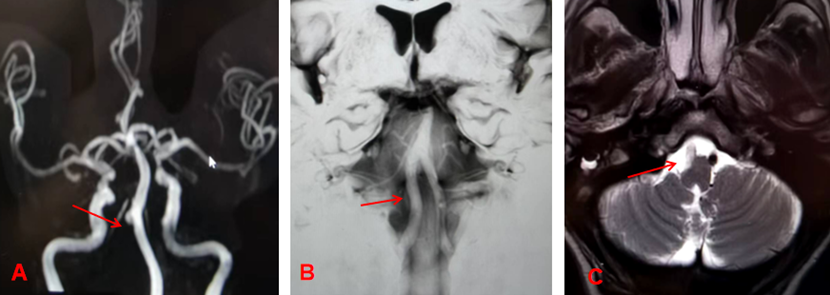
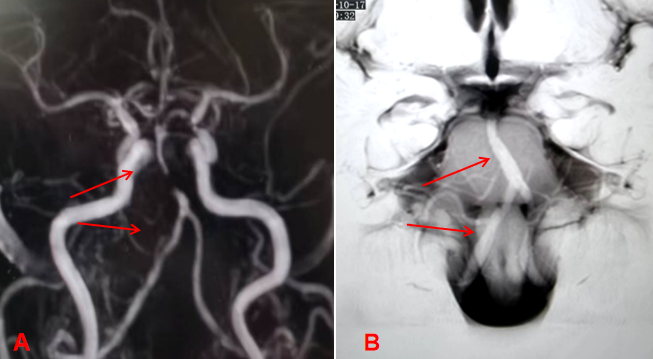
The area under the curve was increased significantly by combining BPAS imaging findings with MRA (0.92 Vs 0.85), the sensitivity, specificity of MRA and MRA+BPAS were 66.67% vs 95.00%,89.13% vs 93.48%, respectively (Figure 1). A total of 60 segments of 106 arteries had lesions. In the arteriosclerosis group, MRA+BPAS was more accurate than MRA alone (93.88% vs 69.39). In the occlusion group, the accuracy of MRA+BPAS was significantly higher than that of MRA (100% vs 42.86%). The diagnostic accuracy of the two methods was both 100% in the dysplasia group, table 1. The diagnostic confidence of MRA+BPAS was significantly higher (0.81 vs 0.95 P=0.237). The consistency of diagnosis results of 2 observers was excellent (Kappa=0.94). Figure 2 and 3 showed the two patients' images of MRA and BPAS-MRI.Discussion
MRA+BPAS has better diagnostic efficiency than TOF-MRA alone. Consider of the insufficient number of cases, the positive rate of lesions in our study was only 56%, which can still reflect the diagnostic trend. MRA+BPAS can identify vascular occlusion much better, while it's difficulty for TOF-MRA to distinguish occlusion from dysplasia. MRA+BPAS can significantly improve the confidence of Radiologists.Conclusion
Compared with MRA, BPAS-MRI can show the outer contour of the vertebrobasilar artery system. Combined with TOF MRA, it may be used to recognize among vertebrobasilar artery abnormalities, and be used in hospitals where conventional high-resolution MRI cannot.Acknowledgements
No acknowledgement found.References
[1] Liu J,Zhao L,Yao L,et al. Basi-parallel anatomic scanning (BPAS-MRI) compared with high-resolution MRI for the diagnosis of vertebrobasilar artery abnormalities. Eur J Radiol,2020,123: 08791.
[2] Fatima Z,Motosugi U,Okumura A,et al. Basi-parallel anatomical scanning (BPAS)-MRI can improve discrimination of vertebral artery dissection from atherosclerosis and hypoplasia. Acad Radiol,2012,19 (11 ): 1362-1367.
[3] Iwata R, Yamashita K, Nishikawa T, et al. Diagnosis of anterior inferior cerebellar artery occlusion on magnetic resonance angiography with reference to basiparallel anatomic scanning-magnetic resonance imaging. Neurol Med Chir (Tokyo), 2010, 50(11): 987-989.
[4] Nagahata M, Abe Y, Ono S et al. Surface appearance of the vertebrobasilar artery revealed on basi parallel anatomic scanning (BPAS)-MR imaging: its role for brain MR examination. ANJR Am J Neuroradiol,2005, 26(10): 2508-2513.
Figures