3423
Cardiac T1 and T2 Mapping: The Importance of Rest Periods in Quantitative Tissue Property Mapping
Seth Garrett, B.S.1, Jesse Hamilton, Ph.D.1, and Nicole Seiberlich, Ph.D.1
1Michigan Medicine- Department of Radiology, University of Michigan, Ann Arbor, MI, United States
1Michigan Medicine- Department of Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Artifacts, Cardiovascular
The aim of this study is to assess whether the presence of rest periods in the form of breathhold commands affects T1 and T2 values measured in the myocardium using both clinically standard pulse sequences and cardiac Magnetic Resonance Fingerprinting (MRF). When mapping data are collected immediately following cine acquisitions, T1 maps from both MOLLI and MRF show significant errors, although T2 maps from both T2-prepared bSSFP and MRF are unaffected by the absence of a pause between sequences.Introduction
Current CMR protocols strive for efficiency, as these examinations tend to be time consuming and difficult for the patient due to the number of images that must be collected. More and more sites are moving to 30-minute (or shorter) scan slots and automated scanning to reduce idle time1. However, while rapid scanning with little time between the application of one pulse sequence and the next may not impact qualitative image sequences (i.e. cine), such a set-up has the potential to impact measured T1 and/or T2 values if insufficient time is allowed for complete relaxation of the magnetization between scans. Given the need for precise T1 and T2 measurements to assess cardiac pathologies, this becomes an important consideration. Thus, the study aims to assess the differences in measured myocardial T1 and T2 values using both clinically standard pulse sequences and cardiac Magnetic Resonance Fingerprinting (MRF)2 when scans are performed with and without rest periods (breathhold commands) after cine or mapping sequences.Methods
Two healthy subjects were scanned in this IRB-approved study on a 1.5T MRI scanner (MAGNETOM Sola, Siemens Healthineers, Erlangen, Germany) at a mid-ventricular short-axis slice. Three pulse sequences for quantitative tissue property mapping were assessed: T1 mapping with 5(3)3 MOLLI (11-heartbeat breathhold), T2 mapping with T2-prepared bSSFP (10-heartbeat breathhold with 0, 25, and 55ms T2-prep times), and simultaneous T1-T2 mapping with 15-heartbeat MRF. These will be referred to as the “test” sequences. All sequences were performed during breathholds at end-expiration as instructed by the automated breathhold commands on our system. First, the test sequence was applied, preceded and followed by a 30-second rest interval to allow the magnetization to completely relax. Subsequently, a clinical cine scan was collected in a breathhold, again followed by a short rest period in which the subject inhaled and was immediately given an automated breathhold command before the test sequence was applied. The same series was fully repeated using the same test sequence but without breathhold commands before the test sequence to shorten the time between application of these sequences (the subject held their breath continuously through the entire set of two sequences). T1 maps from MOLLI and T2 maps from bSSFP were produced using in-line vendor software. T1 and T2 maps from MRF were generated using a low-rank subspace reconstruction followed by matching to a scan-specific dictionary with corrections for slice profile and preparation efficiency. ITK-SNAP was used to segment myocardial regions of interest in T1 and T2 maps using the AHA 17-segment model to calculate parameter values within ROIs. The mean T1 and T2 values for each myocardial segment were analyzed and compared within the same set of data utilizing 1-sample t-tests to assess statistical significance.Results
Example tissue property maps collected with MOLLI and T2-prepared bSSFP both with and without breathhold commands are shown in Figure 1. When the automated breathhold instructions were given between the collection of cine images and the mapping sequence, there were no statistically significant differences in the measured T1 and T2 values and the baseline T1 and T2 measurements for either subject (Figures 2-5). When breath hold instructions were removed and there was no significant delaytime between the end of the cine sequence and the start of a mapping sequence, there were statistically significant decreases in T1 values by up to 8% for MOLLI and 12% for MRF. There were no statistically significant differences for either T2 mapping approach when breathhold commands were not deployed and no pause was inserted between measurements.Discussion
When breathhold instructions were present, there were no statistically significant differences in either T1 or T2 values in quantitative tissue property mapping sequences compared to baseline measurements. Given that the breath hold instructions take approximately 8 seconds, this time is sufficient for the magnetization to relax such that the measurements are reliable. However, when breathhold instructions were removed from the protocol and sequences were applied directly back-to-back, there were statistically significant decreases in T1 values measured using both MOLLI and MRF. Interestingly, there were no changes in the T2 values measured for either pulse sequence, indicating that these sequences are less susceptible to errors due to incomplete relaxation. While this may be expected for the T2-prep bSSFP method, the fact that MRF still produces accurate T2 measurements despite errors in the simultaneously derived T1 maps is unexpected. This observation may not change how data are collected using current breathhold-driven protocols, but as free-breathing methods move into clinical practice, care should be taken to ensure appropriate rest periods before T1 mapping sequences are applied. Additionally, it should be noted that these trends may not hold true for all MRF sequences, and likely depend on the specific parameters (flip angle patterns, etc.) that are employed.Conclusion
The results of this study suggest that while it is possible to induce significant decreases in T1 values measured using MOLLI and MRF if sufficient time for relaxation between sequential scans is not provided, the time required to give a breathhold command is sufficient to ensure relaxation of the magnetization. T1 values can be affected if sequences are run without pauses, which should be considered when using free-breathing scans.Acknowledgements
We acknowledge Michigan Institute for Imaging Technology and Translation for institutional support and Siemens Healthineers for research support.References
1. Raman SV, Markl M, Patel AR, Bryant J, Allen BD, Plein S, Seiberlich N. 30-minute CMR for common clinical indications: a Society for Cardiovascular Magnetic Resonance white paper. J Cardiovasc Magn Reson. 2022 Mar 1;24(1):13. doi: 10.1186/s12968-022-00844-6. PMID: 35232470; PMCID: PMC8886348.
2. Hamilton JI, Jiang Y, Chen Y, Ma D, Lo WC, Griswold M, Seiberlich N. MR fingerprinting for rapid quantification of myocardial T1 , T2 , and proton spin density. Magn Reson Med. 2017 Apr;77(4):1446-1458. doi: 10.1002/mrm.26216. Epub 2016 Apr 1. PMID: 27038043; PMCID: PMC5045735.
Figures
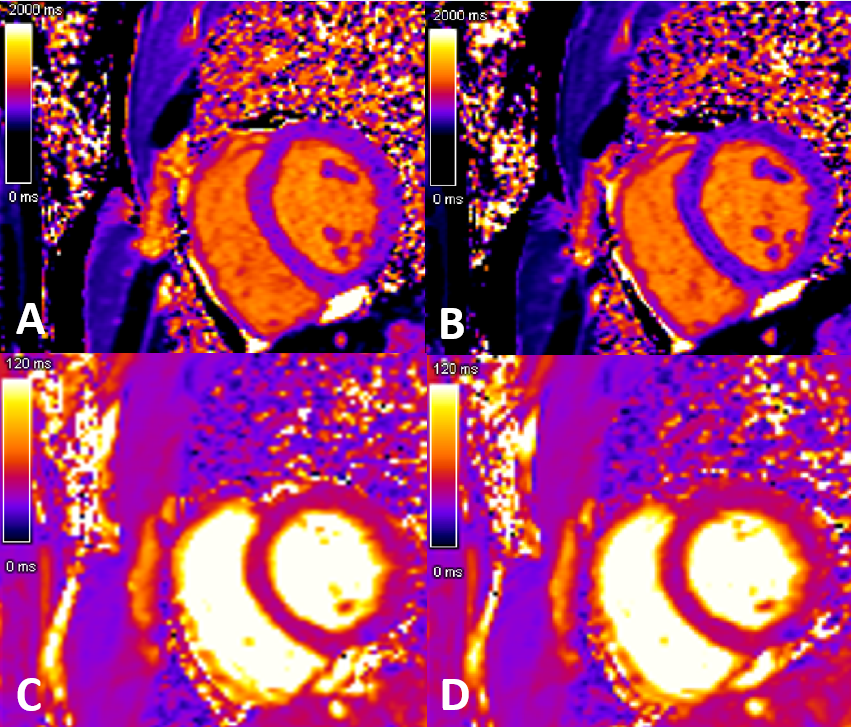
Figure 1. (A) Control MOLLI T1 map with full rest interval. (B) MOLLI T1 map immediately post-cine without a pause for breathhold commands, showing decreased T1 values in the myocardium. (C) Control bSSFP T2 map with full rest interval. (D) bSSFP T2 map immediately post-cine without a pause for breathhold commands, showing consistent T2 values in the myocardium.
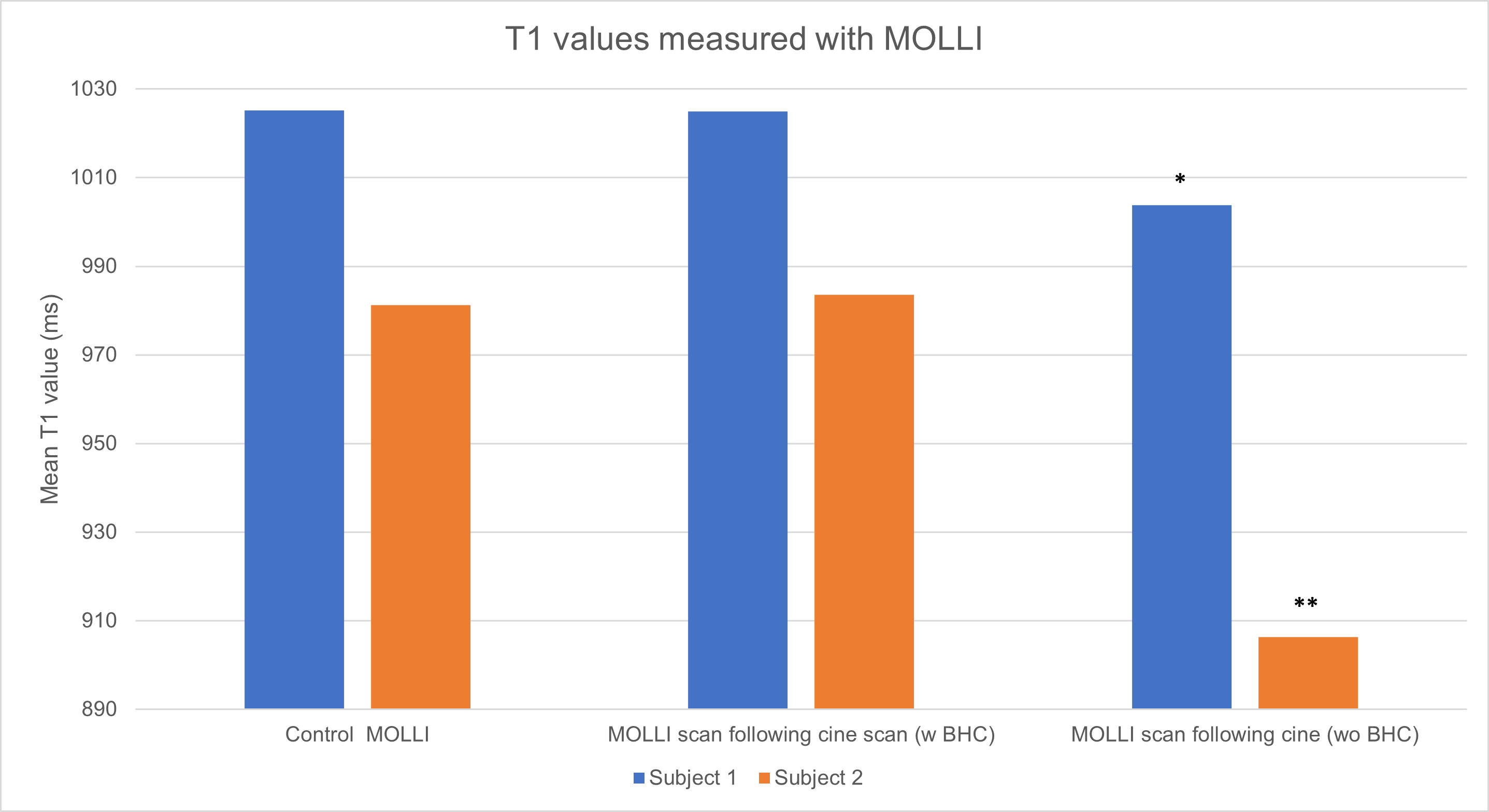
Figure 2. T1 values collected using MOLLI in two healthy subjects. Values measured at baseline, following a cine scan with breathhold commands (w BHC) and following a cine scan without breathhold commands (wo BHC) are shown. Statistically significant differences are seen in both in vivo subjects, with a decrease in T1 values compared to the control scan (with full relaxation) when no pause to deliver breathhold commands is included.
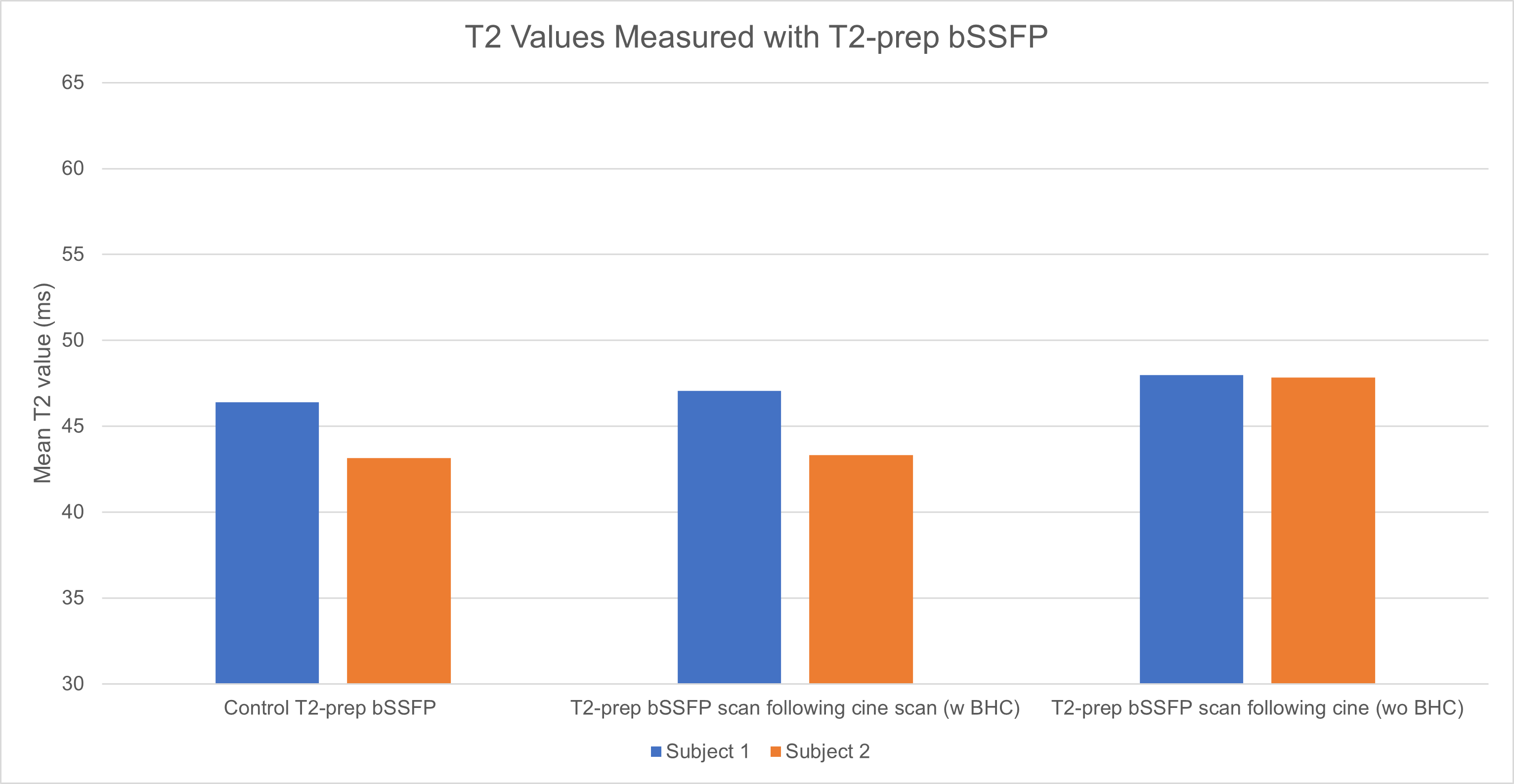
Figure 3. T2 values collected using T2-prep bSSFP in two healthy subjects. Values measured at baseline, following a cine scan with breathhold commands (w BHC) and following a cine scan without breathhold commands (wo BHC) are shown. No significant differences are seen in either in vivo subject for T2 values compared to the control scan (with full relaxation) when no pause to deliver breathhold commands is included.
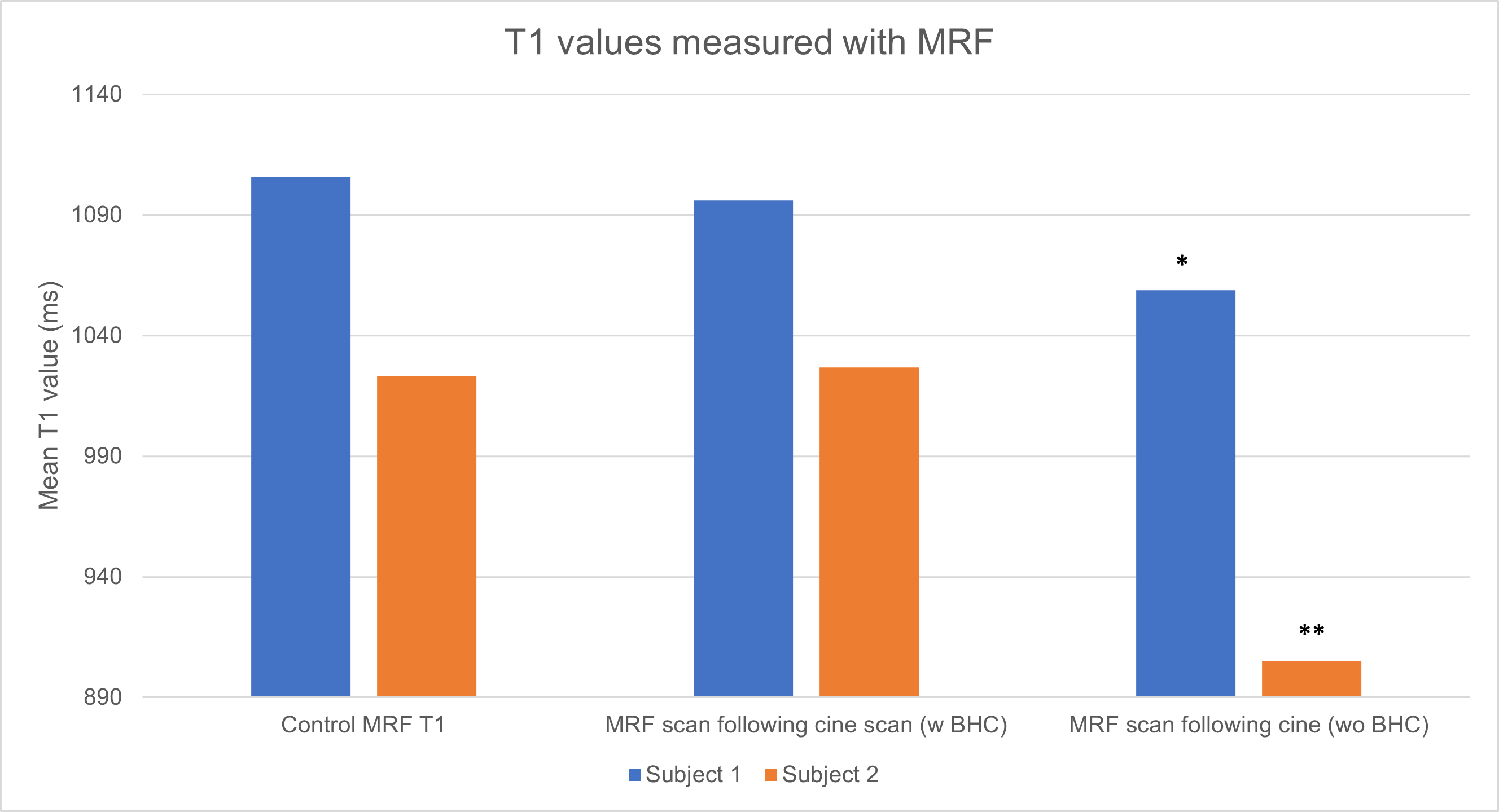
Figure 4. T1 values collected using MRF in two healthy subjects. Values measured at baseline, following a cine scan with breathhold commands (w BHC) and following a cine scan without breathhold commands (wo BHC) are shown. Statistically significant differences are seen in both in vivo subjects, with a decrease in T1 values compared to the control scan (with full relaxation) when no pause to deliver breathhold commands is included.
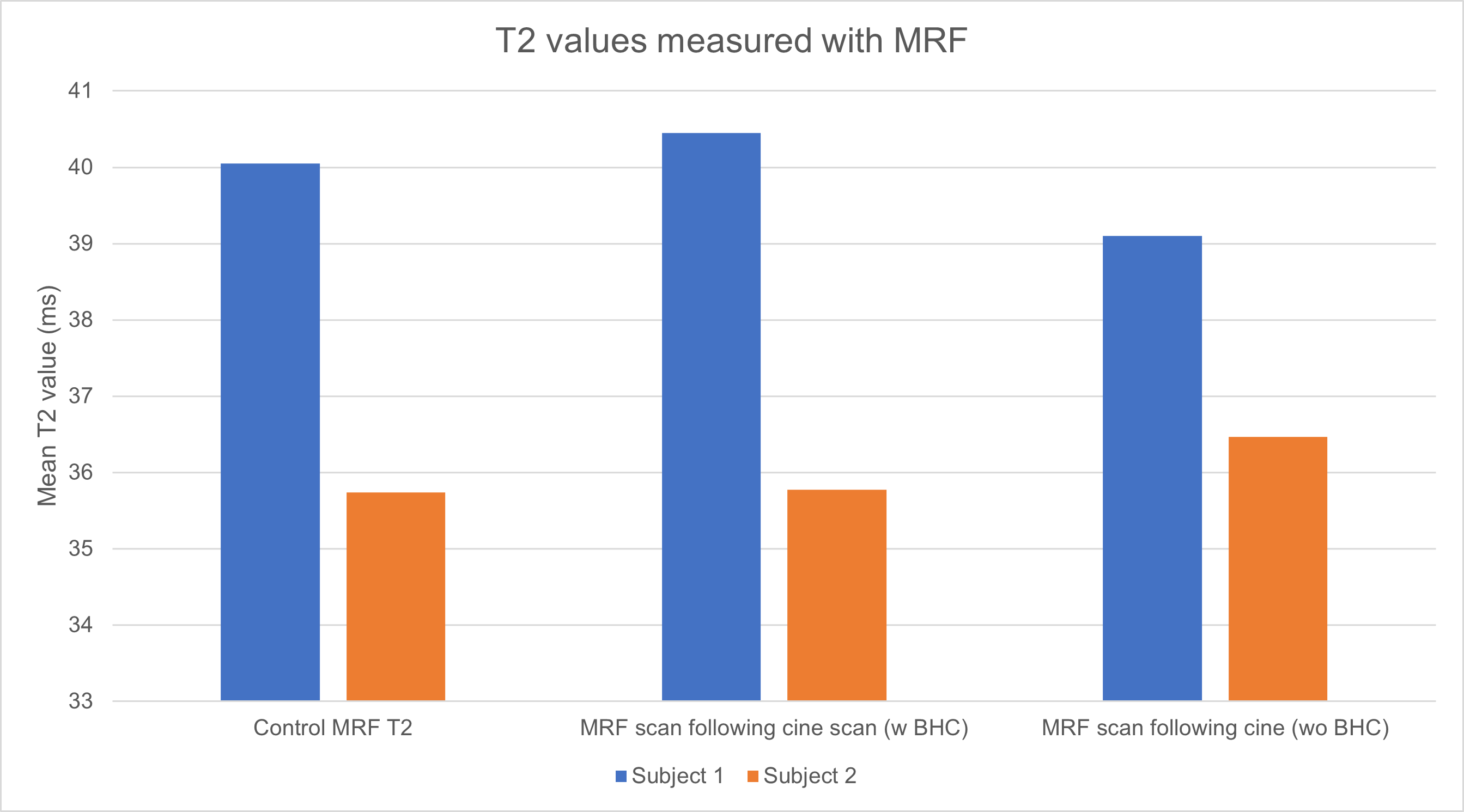
Figure 5. T2 values collected using MRF in two healthy subjects. Values measured at baseline, following a cine scan with breathhold commands (w BHC) and following a cine scan without breathhold commands (wo BHC) are shown. No significant differences are seen in either in vivo subject for T2 values compared to the control scan (with full relaxation) when no pause to deliver breathhold commands is included.
DOI: https://doi.org/10.58530/2023/3423