3418
Demonstration of motion-dependent magnetic field inhomogeneity in the kidneys and its retrospective correction for renal DWI1Department of Radiology, NYU Langone Health, New York, NY, United States, 2Siemens Medical Solutions USA Inc., New York, NY, United States, 3Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Artifacts, Kidney, TOPUP, Field Inhomogeneity
Echo planar imaging is highly affected by field map inhomogeneity distortion artifact. Field map inhomogeneity has shown to be motion dependent in the kidneys. In the present work, we propose an alternative method for correction of magnetic field inhomogeneity for renal DWI in respiratory-resolved fashion. Specifically, we collect a series of forward and reverse phase encoded b=0 images to sample kidney motion caused by breathing, map the spatial and respiratory phase dependence of the magnetic field inhomogeneity, and correct each image of free-breathing DWI series according to their respiratory phase.Introduction
Echo planar imaging, a common readout for diffusion weighted imaging (DWI), is sensitive to eddy currents, static magnetic field (B0) inhomogeneity, and respiratory motion 1. Solutions include using bipolar gradients, acquiring reverse and forward phase encodings for distortion correction 2, and prospective triggering or retrospective registration. Breathing causes craniocaudal kidney movements of 10-16 mm 3,4 and modulates field inhomogeneity (FI). Several studies have demonstrated motion dependence of FI and corrected it retrospectively 5 or prospectively 6-9. Coll-Font et al. 6 performed correction of renal DWI distortion using forward and reverse images of the same directional diffusion encoding acquired with multiple echoes allowing for correction of each image at each breathing phase separately. In the present work, we propose an alternative method for correction of FI for renal DWI in respiratory-resolved fashion. Specifically, we employ 32 forward and 32 reversed b=0 images to sample kidney motion, and map the spatial and respiratory phase dependence of the B0 inhomogeneity. These B0 maps are then applied to correct the DWI series according to their respiratory phase.Methods
In this HIPAA-compliant and IRB-approved prospective study, 8 volunteers (6M, ages 28-51) provided written informed consent and had abdominal imaging performed in a 3 T MRI system (MAGNETOM Prisma; Siemens Healthcare, Erlangen, Germany) in supine position with posterior spine array and anterior body array RF coils and chest leads for ECG gating. Coronal oblique T2-weighted SSFSE (HASTE) images were collected for anatomical reference. Sagittal phase-contrast (PC) MRI images through the left renal artery were collected at multiple cardiac phases to estimate systolic and diastolic phases for kidney. With a DWI research application sequence with dynamic field correction, cardiac triggered oblique coronal DWI (TR/TE 2800/81 ms, matrix 192/192/1, resolution 2.2/2.2/5 mm) were collected at 10 b-values between 0-800 s/mm2 and 12 directions. To correct for FI, 32 right-to-left and 32 left-to-right phase-encoding b=0 images were acquired, half before and half after the DWI acquisition to account for bulk motion. Figure 1 is a pictorial description of our method. The 64 b=0 images were registered using mutual information (MI) metrics to one of the forward images in the set taken as reference using the FireVoxel software, build 380, https://firevoxel.org/. The craniocaudal translation of this rigid transformation was logged to create a limited number of discrete motion bins, each containing at least five forward and reverse images. Each bin was corrected using the TOPUP function of FSL software (version, 6.0.1) and its FI map was outputted. Each image of the DTI set was registered to the previous reference image, and distortion corrected with the appropriate B0 map for its location. The corrected and uncorrected images were registered to their corresponding HASTE image, and their MI metrics compared. Finally, a line profile analysis evaluated the variability of the apical region over the full DTI acquisition with and without motion-resolved distortion correction. The dependence of field map inhomogeneity on the kidney side (i.e. right and left), region (i.e. lower, middle, upper, and apical), and breathing phase was statistically analyzed using mixed model analysis of variance. Tests for significant variation with each factor in this model were quantified by an F statistic and p-value. Mixed model analysis of variance was used to assess the effect of each DWI, side and method (N (No correction), O (one bin correction), and M (multi-bin correction)) on MI. MI metrics from different methods (N,O,M) were compared via t-statistics of pairwise comparisons for all acquired images. For the line profile analysis, all line profile standard deviations for a given subject, kidney, and correction method (O or M) were averaged and compared with a paired sample t-test between correction methods.Results
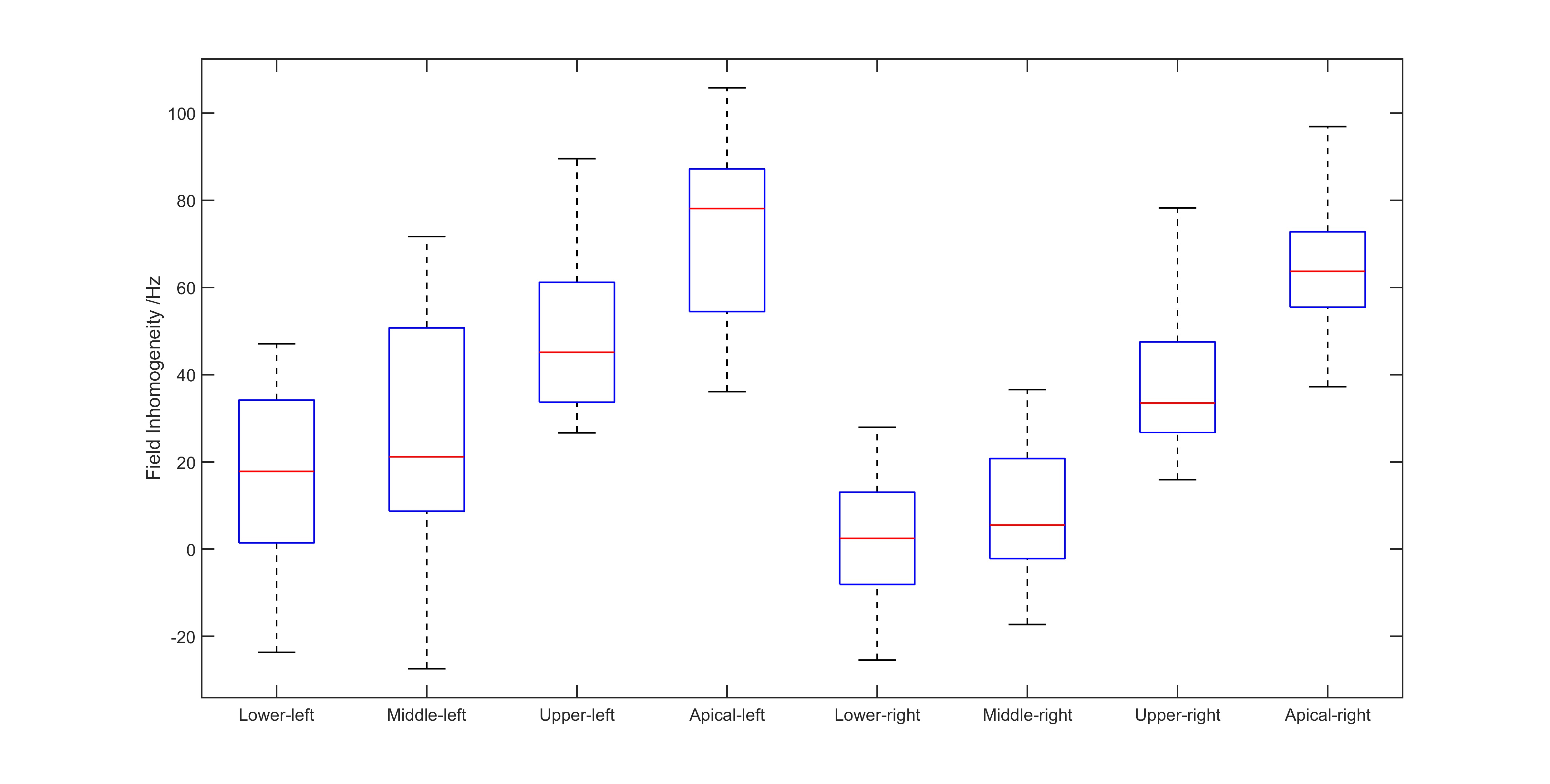
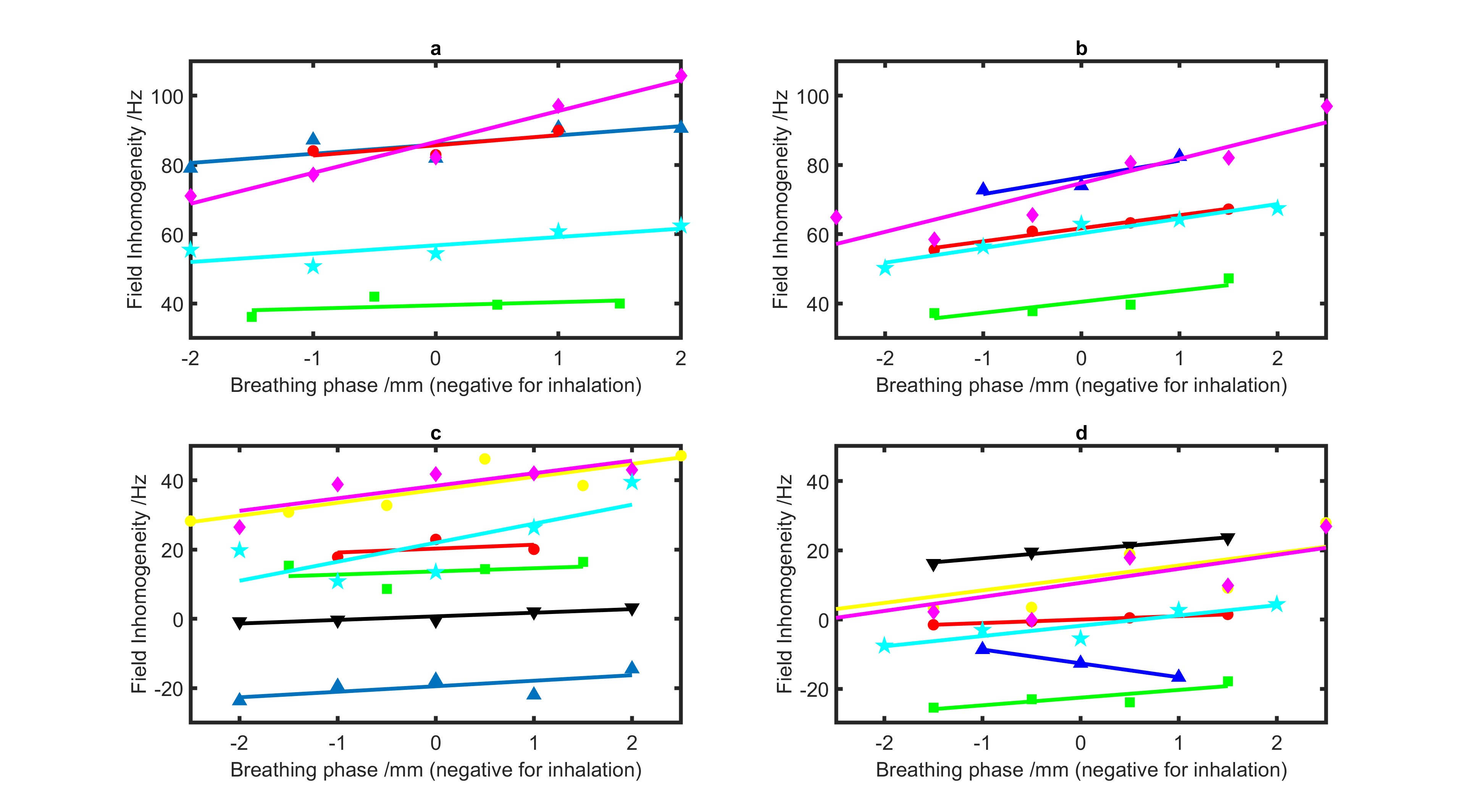
After exclusion of one subject due to low image quality, seven subjects contributed to FI derivations for the lower, middle and upper regions and five subjects contributed to FI derivations for the apical layer, registration comparison and line profile analysis. Figure 2 shows motion-dependent FI maps of one subject. FI was found to vary significantly (p<0.001) with each factor considered (Region : F = 294.36; Side: F = 61.32; Phase: F = 4.5). Figures 3, 4, and 5 show the group dependence of field inhomogeneity on kidney side, region, and breathing phase, respectively. MI was found to vary significantly (p<0.001) with consideration of factors kidney side: F = 374.9 and correction method: F= 574.4. MI was significantly lower for N than for each of the corrected methods on each side and over both sides combined (p<0.001). Additionally, MI was significantly lower for O than M in the left kidney (p<0.001), whereas, MI difference for the two methods was not significant in the right kidney (p=0.86). In the line profile analysis, multi-binning resulted in significantly better registration (p=0.006).Discussion
Improvements in morphologic accuracy can be obtained with motion-resolved distortion correction in the kidney. The presented method utilizes 64 reverse and forward images acquired in 230 seconds, which may be beneficial for minimizing scan time. The results of this study also indicate significant dependence of field inhomogeneity on kidney side, region, and breathing phase. The information in this spatiotemporal mapping might facilitate prospective B0 shimming on 7T scanners, similar to earlier works 5.Acknowledgements
Funding support is acknowledged from the National Institute of Health (NIH).References
1. Pierpaoli, C., Artifacts in diffusion MRI. Diffusion MRI: theory, methods and applications, 2010: p. 303-318.
2. Smith, S.M., et al., Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage, 2004. 23 Suppl 1: p. S208-19.
3. Hallman, J.L., et al., A four-dimensional computed tomography analysis of multiorgan abdominal motion. Int J Radiat Oncol Biol Phys, 2012. 83(1): p. 435-41.
4. Bussels, B., et al., Respiration-induced movement of the upper abdominal organs: a pitfall for the three-dimensional conformal radiation treatment of pancreatic cancer. Radiother Oncol, 2003. 68(1): p. 69-74.
5. Vannesjo, S.J., et al., Spatiotemporal characterization of breathing-induced B0 field fluctuations in the cervical spinal cord at 7T. Neuroimage, 2018. 167: p. 191-202.
6. Coll-Font, J., et al., Retrospective Distortion and Motion Correction for Free-Breathing DW-MRI of the Kidneys Using Dual-Echo EPI and Slice-to-Volume Registration. J Magn Reson Imaging, 2021. 53(5): p. 1432-1443.
7. Afacan, O., et al. Dual-echo blip reversed EPI acquisition enables distortion correction in the presence of motion in diffusion-weighted MRI. in Int Soc Magn Reson Med. 2019.
8. Afacan, O., et al., Simultaneous Motion and Distortion Correction Using Dual-Echo Diffusion-Weighted MRI. J Neuroimaging, 2020. 30(3): p. 276-285.
9. Gallichan, D., et al., Reducing distortions in diffusion-weighted echo planar imaging with a dual-echo blip-reversed sequence. Magn Reson Med, 2010. 64(2): p. 382-90.
Figures
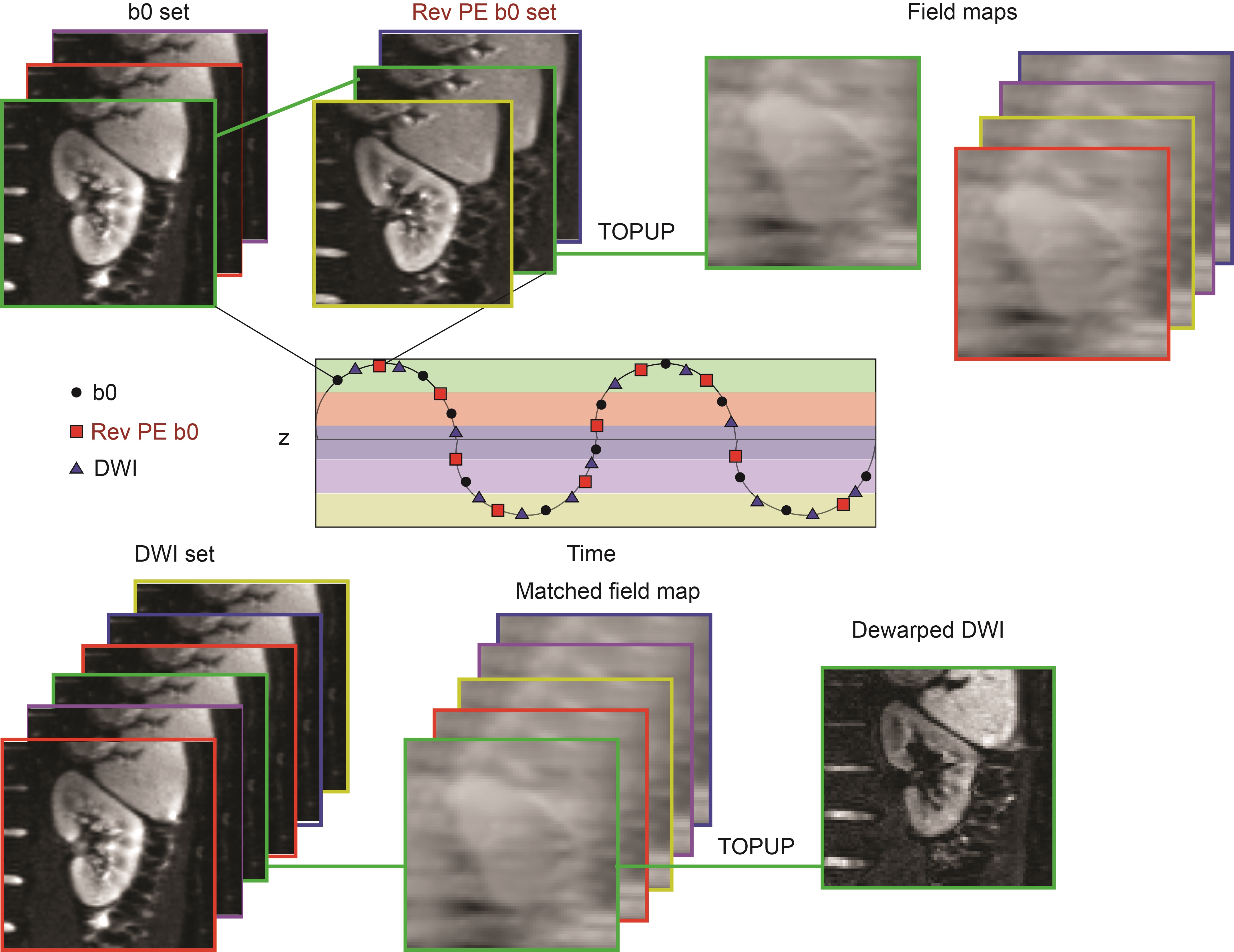
Figure 1: The diagram for the proposed workflow including registration, motion binning, and field inhomogeneity-based distortion correction (TOPUP algorithm).
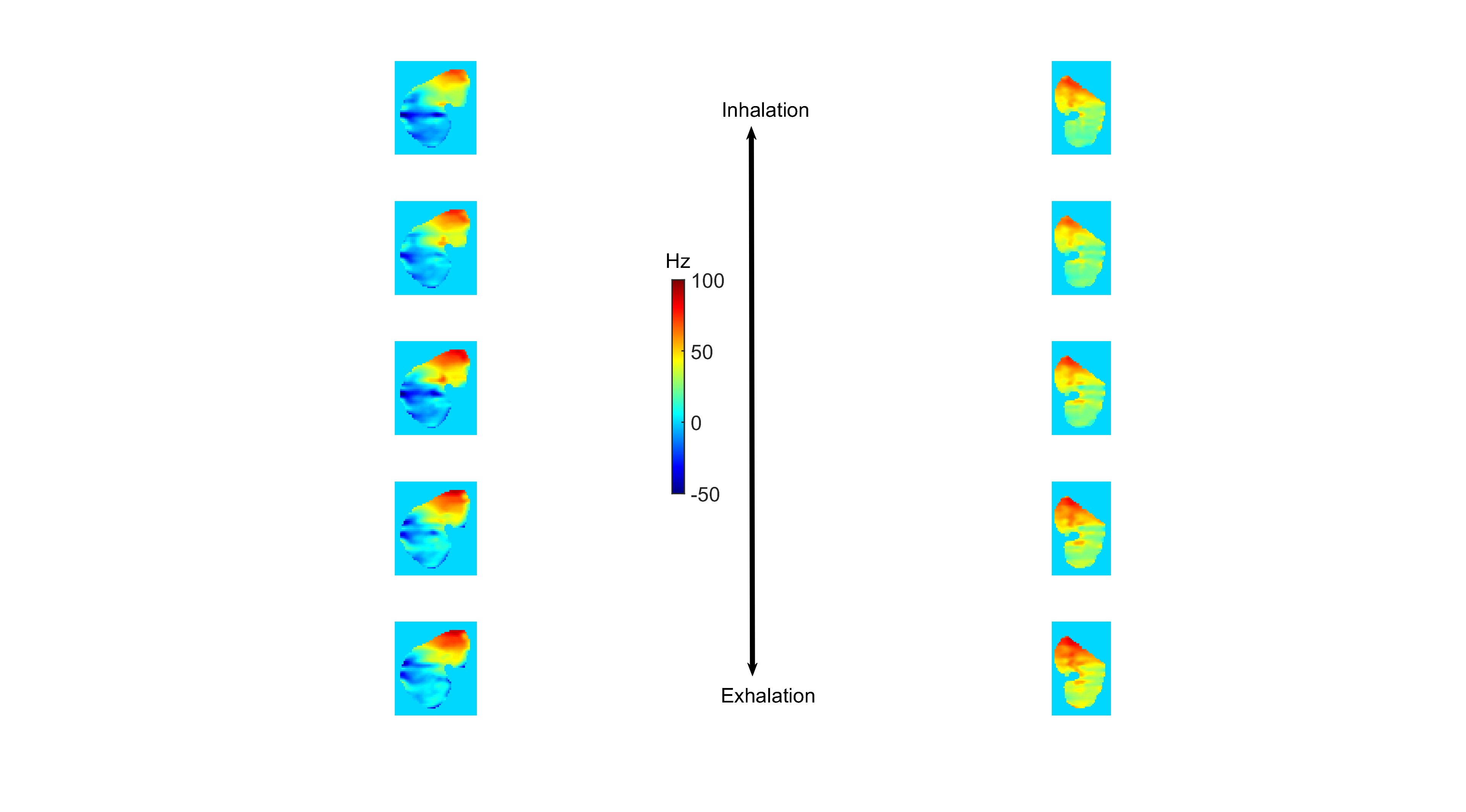
Figure 2: Example field inhomogeneity maps in left and right kidneys throughout breathing cycle showing clear dependencies on kidney side, region, and respiratory phase.
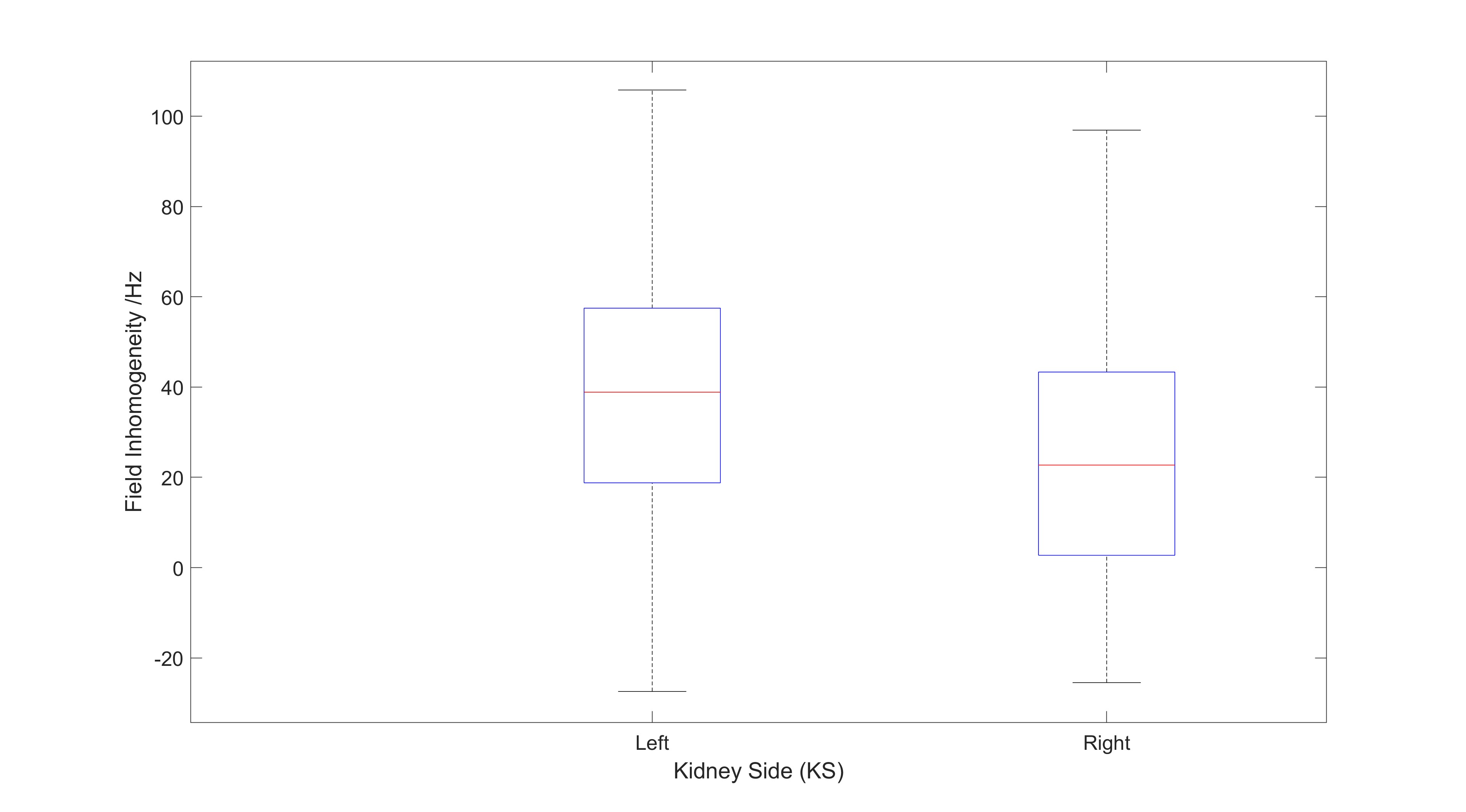
Figure 3: Group boxplot of field inhomogeneity vs. kidney laterality or side (KS), including all breathing phases and kidney regions.