3347
Brain activity alterations in premature ejaculation patients before and after treatment with sertraline1Radiology, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, China, 2Andrology, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, China, 3GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Brain Connectivity, Brain Connectivity
This study aimed to explore the central neural mechanisms underlying sertraline in the treatment of premature ejaculation (PE). Resting-state functional magnetic resonance imaging (rs-fMRI) of PE patients before and after treatment with sertraline were acquired. The brain regions with altered regional homogeneity (ReHo) values were found. Increased activity in the occipital lobe and decreased activity in the prefrontal and parietal lobe and thalamus might be the mechanisms of sertraline in the treatment of PE.Introduction
Sertraline is considered a common treatment for patients with premature ejaculation (PE), and abnormal brain activities have been found in PE patients by resting state-functional magnetic resonance imaging (fs-MRI)[1, 2]. However, the differences of brain function in PE patients before and after administration of sertraline have not been explored. Therefore, the main goal of this study was to investigate if alterations of brain activities can be found for PE patients after sertraline treatment by means of fs-MRI.Materials and Methods
SubjectsA total of 25 PE patients aged from 20 to 45 years were recruited in this study. PE patients were diagnosed according to the PE Guidelines published by International Society for Sexual Medicine (ISSM)[3]: (1) ejaculation always or nearly always occurred prior to or within approximately 1 minute of vaginal penetration since the first sexual experience and remained throughout life (primary PE) or had a clinically significant and bothersome reduction in IELT (by self-report) at some point in the life after a period of normal ejaculatory function (acquired PE); (2) inability to delay ejaculation on all or nearly all vaginal penetrations; (3) negative personal consequences related to PE and/or the avoidance of sexual intimacy.
Each of 25 PE patients underwent rs-MRI measurement before and 4 weeks after the treatment with sertraline 50 mg once a day. A written consent was obtained from each patient.
MRI experiments
All MRI experiments were performed on an 3T scanner (Signa Architect, GE, USA) with 48 channel head coil employed. All participants were instructed to relax, think of nothing in particular, stay awake with eyes closed and move as little as possible during the scan. Structural high resolution 3D-T1 weighted images were acquired with scan parameters of repetition time (TR)=7.7ms, echo time (TE)=3.1ms, number of slices=160, slice thickness=1mm, field of view (FOV)=256×256mm2, matrix size=256×256, flip angle (FA)=9°. For rs-MRI imaging, the scan parameters were of TR=2000ms, TE=30ms, number of slices=33, slice thickness=3.5mm, FOV=224×224mm2, matrix size=80×80, FA=90°. All subjects had no obvious structural damage examined by two radiologists based on conventional MRI images.
Data analysis
The preprocessing of MRI data was performed using the software of Data Processing Assistant for Resting-State fMRI (DPARSF) (Advanced Edition; State Key Laboratory of Cognitive Neuroscience and Learning, Beijing Normal University, Beijing, China), a software plug-in within Data Processing & Analysis for Brain Imaging (DPABI)[4]. Regional Homogeneity (ReHo) was calculated using the software of DPARSF. Individual ReHo map for each participant was obtained by calculating Kendall’s coefficient concordance (KCC) of the time series of a given voxel with 26 voxels adjacent to it, which was then divided by the global mean KCC value. KCC was measured as the correlations between the time series of a given voxel and those of its nearest neighbors in a voxel-wise manner. Finally, standardized map was spatially smoothed with a 6mm×6mm×6mm FWHM Gaussian kernel, which could decrease spatial noise. For subsequent statistical analysis, ReHo map was standardized using Fisher’s r-to-z transformation, improving the normality of the correlations.
Statistic analysis
All statistic analyses were performed with the REST Software (version: V1.8; State Key Laboratory of Cognitive Neuroscience and Learning, Beijing Normal University, Beijing, China)[5]. The whole-brain regional homogeneity (ReHo) values were calculated and compared for patients before and after treatment by two sample t‐test using the REST Software. The significant difference was set at P <0.001 for voxel and P<0.05 for cluster (a minimum cluster size of 6 voxels, corrected by the AlphaSim program).
Results
Compared with patients before treatment, increased ReHo values were detected in the left inferior occipital gyrus and right cuneus of patients after treatment. (Table 1; Figure 1);Compared with patients before treatment, decreased ReHo values were detected in the left thalamus, supplementary motor area and paracentral lobule, right superior frontal gyrus, triangular part of inferior frontal gyrus and posterior cingulate gyrus of patients after treatment. (Table 1; Figure 1)
Discussion and Conclusion
In this study, we investigated the differences of rs-MRI derived ReHo values of PE patients before and after administration of sertraline. Increased activity in the occipital lobe and decreased activity in the prefrontal, parietal lobe and thalamus were found in PE patients after the treatment of sertraline. These brain regions play a central role in cognitive, sensory, and emotional information processing, and are also involved in several diseases, such as depressive disorder. This may be an effective method to screen PE patients with positive response to sertraline relative to a self-reported sexual history, helping the clinical diagnosis for PE patients.In conclusion, these findings in this study improved the understanding of central neural mechanisms of sertraline in the treatment of PE patients, and provided useful biomarkers for redicting the therapeutic effect of sertraline in the treatment of PE.
Keywords
Premature ejaculation; Sertraline; Resting-state fMRI; Regional homogeneityAcknowledgements
No acknowledgement found.References
1.Liu S, Zhang X, Wang Q, Xu Y, Huang X, Liu T, et al. Increased attentional network activity in premature ejaculation patients with anxiety revealed by resting-state functional magnetic resonance imaging. The European journal of neuroscience. 2021;54(4):5417-26. Epub 2021/07/31. doi: 10.1111/ejn.15402. PubMed PMID: 34327757.
2.Chen J, Wu W, Xiang Z, Wang Q, Huang X, Lu C, et al. Aberrant default mode network and auditory network underlying the sympathetic skin response of the penis (PSSR) of patients with premature ejaculation: A resting-state fMRI study. Andrology. 2021;9(1):277-87. Epub 2020/10/01. doi: 10.1111/andr.12914. PubMed PMID: 32996293.
3.Althof SE, McMahon CG, Waldinger MD, Serefoglu EC, Shindel AW, Adaikan PG, et al. An update of the International Society of Sexual Medicine's guidelines for the diagnosis and treatment of premature ejaculation (PE). The journal of sexual medicine. 2014;11(6):1392-422. Epub 2014/05/23. doi: 10.1111/jsm.12504. PubMed PMID: 24848686.
4.Chao-Gan Y, Yu-Feng Z. DPARSF: A MATLAB Toolbox for "Pipeline" Data Analysis of Resting-State fMRI. Frontiers in systems neuroscience. 2010;4:13. Epub 2010/06/26. doi: 10.3389/fnsys.2010.00013. PubMed PMID: 20577591; PubMed Central PMCID: PMCPMC2889691.
5.Song XW, Dong ZY, Long XY, Li SF, Zuo XN, Zhu CZ, et al. REST: a toolkit for resting-state functional magnetic resonance imaging data processing. PloS one. 2011;6(9):e25031. Epub 2011/09/29. doi: 10.1371/journal.pone.0025031. PubMed PMID: 21949842; PubMed Central PMCID: PMCPMC3176805.
Figures
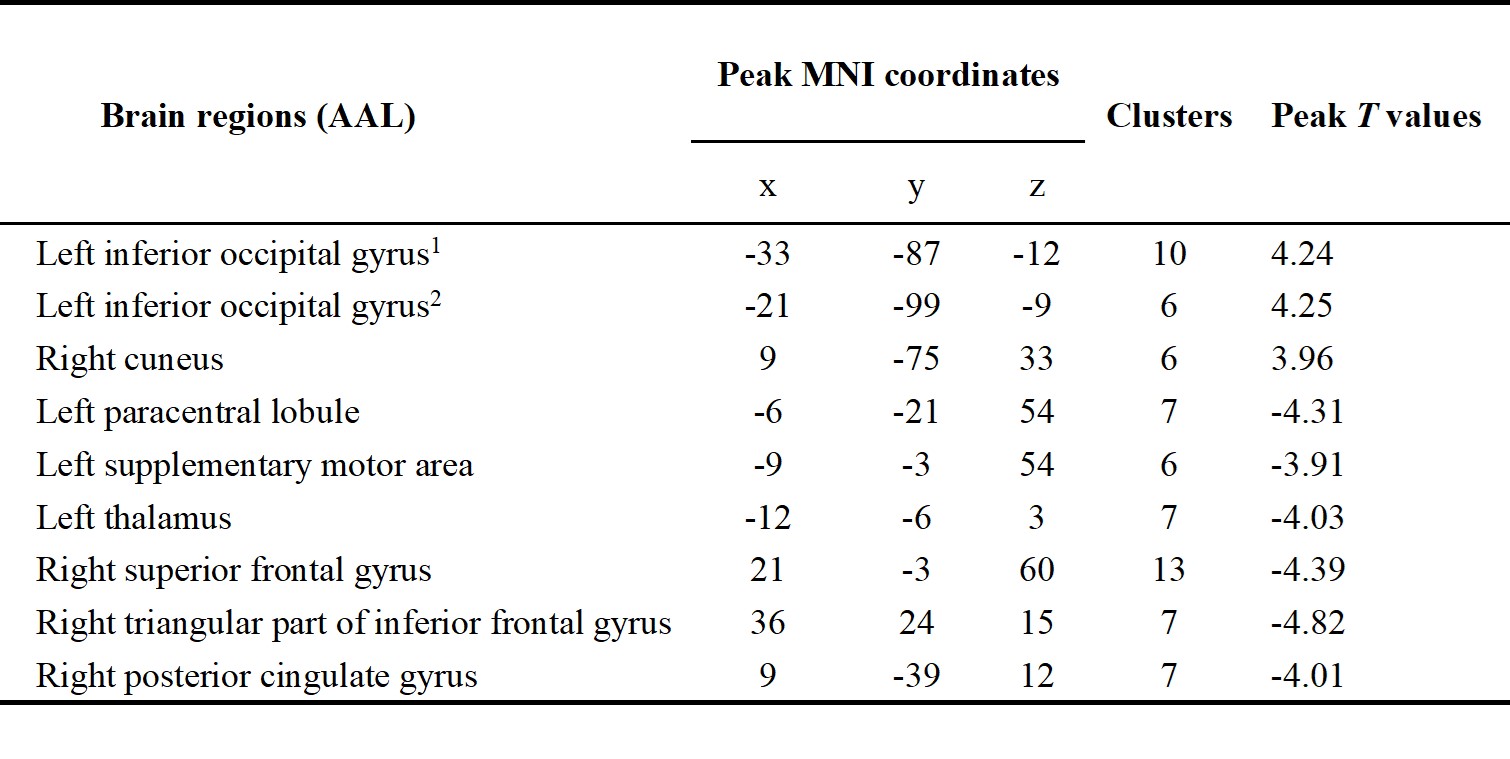
Table 1. Brain regions showed differences in ReHo values for PE patients before and after administration of sertraline.
PE: premature ejaculations. ReHo: regional homogeneity. AAL: anatomic automatic labeling; MNI: Montreal Neurological Institute; x, y and z: the coordinates of peak voxel of each cluster in the MNI space. The significant difference was set at P <0.001 for voxel and P<0.05 for cluster (a minimum cluster size of 6 voxels, corrected by the AlphaSim program).
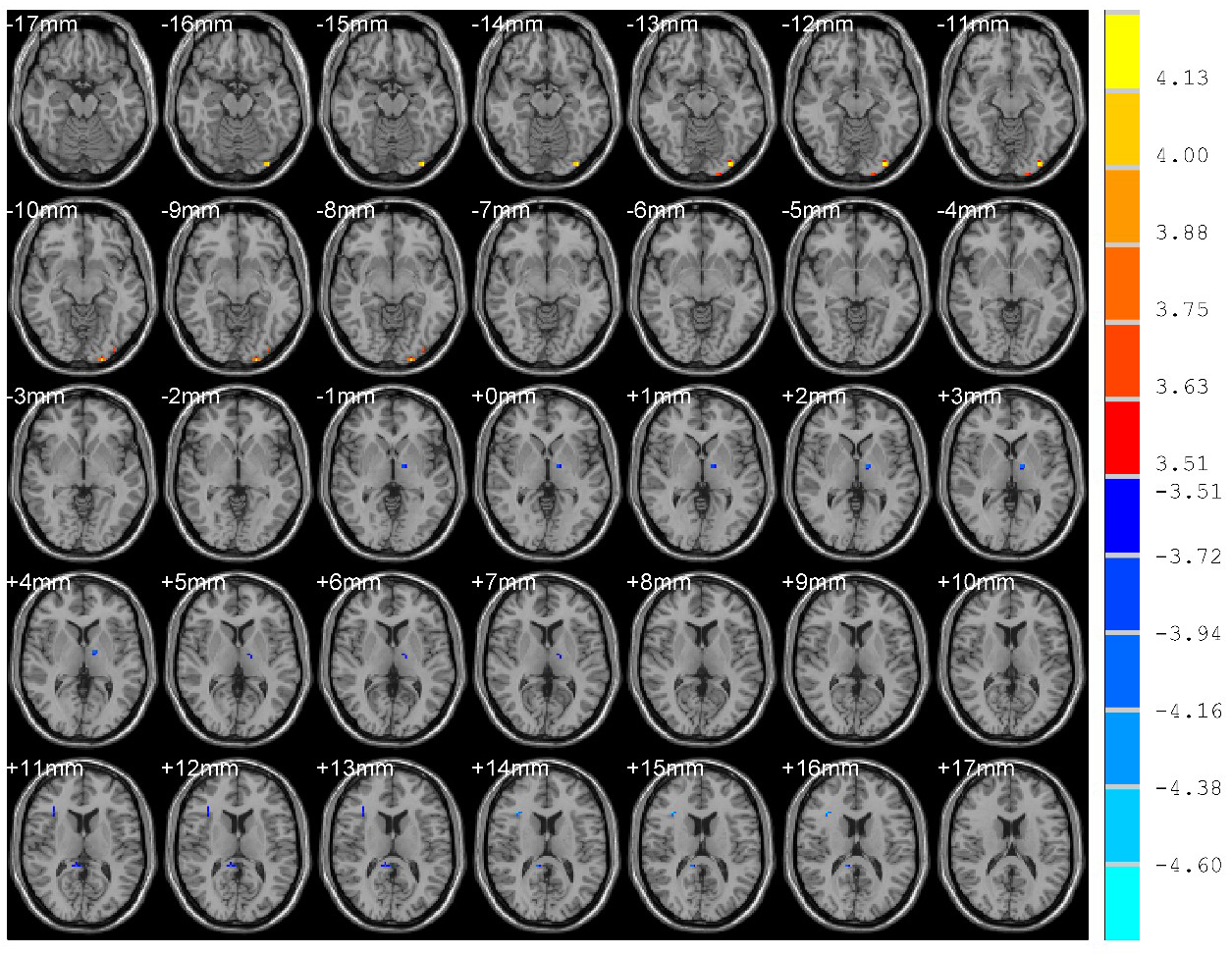
Figure 1. Brain regions showed differences in ReHo values for PE patients before and after administration of sertraline.