3271
Imaging female pelvic anatomy with a portable, low field Magnetic Resonance Imager.1Promaxo, Oakland, CA, United States, 2Cleveland Clinic Indian River Hospital, Vero Beach, FL, United States
Synopsis
Keywords: Pelvis, Body, Pelvic Imaging, Low field MRI
Promaxo's single sided, low-field MRI is used for female pelvic imaging. Five healthy female subjects were scanned. The butterfly shape of vagina and normal anatomy of the puborectails regions were observed. Delineation between puborectails and pubococcygneus muscles are clearly seen. MRI’s improved soft tissue contrast provides better visualization of anatomical regions and is less invasive than transvaginal ultrasound.
INTRODUCTION AND OBJECTIVES:
Promaxo has developed a single sided, low-field MRI for pelvic imaging. It is an open system which projects a magnetic field from its face The static magnetic field is generated by a permanent magnet array and varies from 55mT to 74mT. The gradient and the transmit coils are also in a single sided configuration, mounted to the face of the magnet array. This scanner is FDA-approved for prostate biopsy and treatment guidance. In the present study, we evaluate the use of this low-field MRI for female pelvic floor anatomy. This use case is advantageous as MRI provides a method of non-invasive imaging for diagnosis of Pelvic Organ Prolapse (POP) and following lower urinary symptoms, but 1.5 and 3T MRIs are often not feasible or practical. Using the office-based, low-field MRI, we are able to identify vagina, puborectalis (PR) and pubococcygneus (PC) muscles1 in clinically healthy female patients.METHODS:
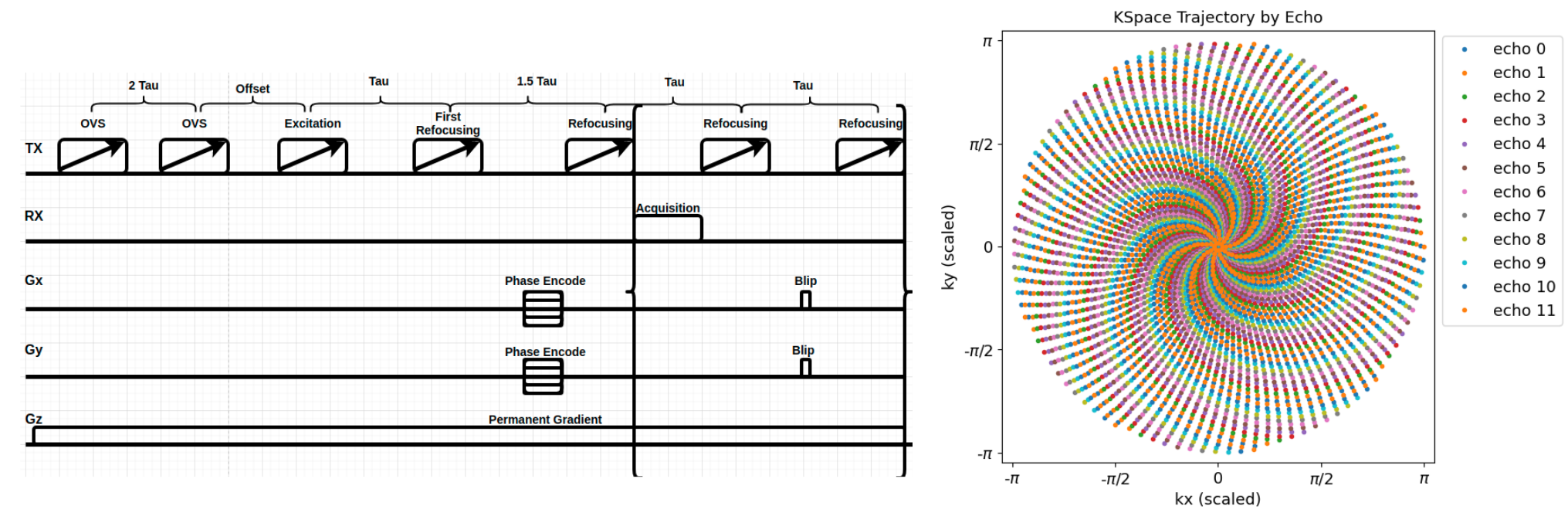
Healthy female subjects (n=5) were positioned in the open sided scanner in high lithotomy as shown in figure 1. A 5 channel receive coil was strapped around the subject’s pelvis. Prior to scanning, baseline characteristics of subjects were recorded to exclude subjects with lower urinary symptoms or symptoms of POP.3D, T2 weighted imaging of the pelvis was performed. The T2 weighted pulse sequence uses broadband, chirped RF pulses in a CHORUS type sequence to minimize the effects of B1 inhomogeneity2 . Blipped RARE phase encoding with a center out spiral trajectory was used3 (Figure 2). In this trajectory, each echo in the echo train phase encodes a different kx-ky point while kz is frequency encoded with the permanent z gradient used as the readout gradient. The sequence has echo train length of 12 (TR= 1.45 s, echo spacing 8.6 ms, in plane encoding 56 x 56, FOV = 33 X 33 X10 cm).
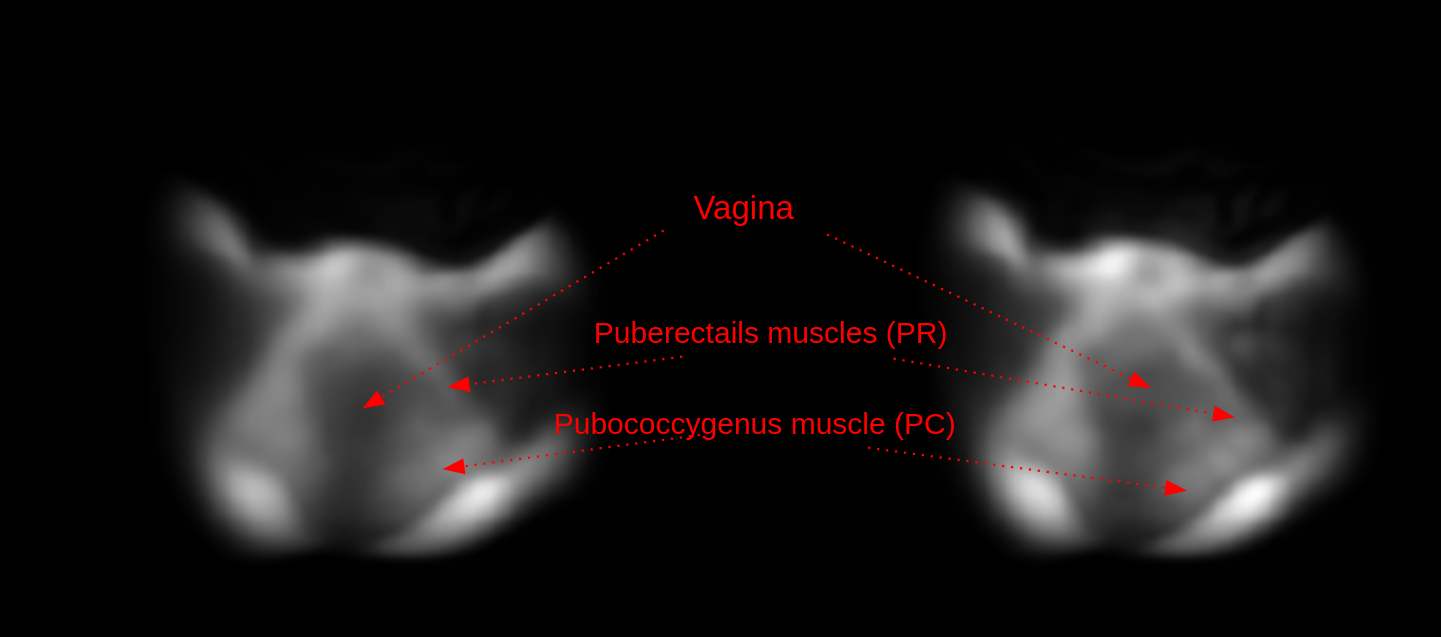
Images were reconstructed with 1.5 X 1.5 mm in plane resolution, effective field of view 18 X 18 cm, and slice thickness of 2.8 mm. The reconstruction was performed using an iterative, conjugate gradient least square (CGLS) method with Tikhonov regularization and a system matrix which incorporates the nonlinear B0 and gradient fields. Images were visualized in all three planes, and the axial orientation was mainly used to identify vagina, puborectails (PR) and pubococcygneus (PC) muscles which are critical for clinical inference of any pelvic floor abnormalities.
OBSERVATION AND CONCLUSIONS:
The butterfly shape of vagina and normal anatomy of the PR muscles were clearly visible on the low-field MR images, consistent with images from high-field MRI literature4 . A delineation of PR with PC muscle is also seen (Figure 3). We conclude that a low-field, office-based MRI could be a compact and inexpensive alternative to 1.5 or 3T MRI for pelvic floor assessment. MRI’s improved soft tissue contrast provides better visualization of anatomical regions and is less invasive that transvaginal ultrasound. Future work will focus on imaging additional subjects with and without pelvic floor dysfunction to evaluate the diagnostic efficacy of this low field MRI.Acknowledgements
No acknowledgement found.References
1.) Herschorn S, Female Pelvic Floor Anatomy: The Pelvic Floor, Supporting Structures, and Pelvic Organs. Rev Urol 2004: 6 (Suppl 5) S2-S10.
2.) Power JE, Foroozandeh M, et. al., Increasing the quantitative bandwidth of NMR measurements Chem. Commun., Isuue 14. 2016
3.) Tan H and Meyer C.H. Estimation of k-space trajectories in spiral MRI, Magn Reson Med. 2009 Jun;61(6):1396-404.
4.) Tunn R, Rieprich M, Kaufmann O, Gauruder-Burmester A, Beyersdorff D. Morphology of the suburethral pubocervical fascia in women with stress urinary incontinence: a comparison of histologic and MRI findings. Int Urogynecol J Pelvic Floor Dysfunct. 2005 Nov-Dec;16(6):480-6.
Figures