3259
Feasibility of synthetic diffusion weighted images using computed with 5b protocol in uterine tumors1Department of Biomedical Engineering, Hubei University of Medicine, Hubei, China, 2GE Healthcare, Beijing, China, 3Department of Radiology,Taihe Hospital, Hubei University of Medicine, Hubei, China
Synopsis
Keywords: Pelvis, Cancer
High-b-value DWI has been widely applied in clinical practices, but it is challenging to acquire several high b-value images for long acquisition time and more eddy distortion as b-value increases, leading to patient discomfort, increased motion artifacts and decreased SNR. High-b-value SyDWIs showed better SNR and less image distortion than scanned high-b-value DWIs. Our study demonstrate the feasibility of 5b-value synthetic high-b-value reduced full-of-view diffusion weighted imaging with the pros of short scan time, better lesion clarity and higher image quality in comparison of 13b-protocol rFOV-syDWIs and 5b-protocol synthetic ADCmean and ADCminimum offered reliably diagnostic value compared to 13b-protocol ones.Introduction
The incidence rate of benign and malignant tumors in female uterus is on the increase [1]. Previous studies have shown that DWI can effectively assess the invasion depth of uterine corpus and infiltration range of parauterine organ by cervical cancer, especially high b-value DWIs [2,3]. Although high-b-value DWI has been widely applied in clinical practices, it is challenging to acquire several high b-value images for long acquisition time and more eddy distortion as b-value increases, leading to patient discomfort, increased motion artifacts and decreased signal-to-noise ratio (SNR) [4-6]. Synthetic DWIs (syDWIs) are calculated from a group of scanned DWIs with different b-values by extrapolating the fitted signal attenuation curve [7,8]. High-b-value SyDWIs showed better SNR and less image distortion than scanned high-b-value DWIs. Some studies have shown that setting 2 to 5 b-values on a DWI can generate relatively reliable high-b-value DWI images [9,10]. However, no relevant studies have confirmed whether synthetic high b-value DWIs that were computed using a set of 5b DWIs can be used for the clinical diagnosis of cervical cancer. Therefore, we examined the feasibility and reliability of high-b-value rFOV-syDWIs and rFOV-syADCs in clinical diagnosis of cervical disease using 13b-protocol synthetic DW images as standard reference via image quality and diagnostic efficiency including lesion clarity and contrast between lesion and parenchyma.Materials and methods
We retrospectively evaluated the data of 35 patients with cervical cancer and 35 healthy volunteers from May to November 2021. All patients and volunteers underwent rFOV-DWI scans, including a 13b-protocol: b =0, 25, 50, 75, 100, 150, 200, 400, 600, 800, 1000, 1200 and 1500 s/mm2 and a 5b-protocol: b =0, 100, 400, 800,1500 s/mm2. 13b protocol was chosen as standard reference due to more accurate ADC maps using a mono- or bi-exponential computation model when more used b values are used and show good diagnosis efficiency in cervical cancer. rFOV-syDWIs with b values of 1200 (rFOV-syDWIb=1200) and 1500 (rFOV-syDWIb=1500) were generated from two different multiple-b-value image data sets using a mono-exponential fitting algorithm. Qualitative evaluation with 5-point scale (anatomical details, magnetically sensitive artifacts, degree of geometric distortion, and overall diagnostic effectiveness) and quantitative assessment [SNR = Slesion/SDbackground and CNR = Slesion/ (square root of SDlesion2 and SDtissue2)] were done by two radiologists respectively with 5- and 10-year experience in diagnosis of uterine. Intraclass correlation coefficient (ICC) and Cohen’s Kappa was respectively used to test the qualitative consistency. According to homoscedasticity and normality assessed by Levene test and Shapiro–Wilk test, the inter-modality differences of quantitative measurements were respectively examined by Wilcoxon signed rank test or paired t test and the inter-group differences of ADC values were examined by independent t test or Mann-Whitney U test.Results
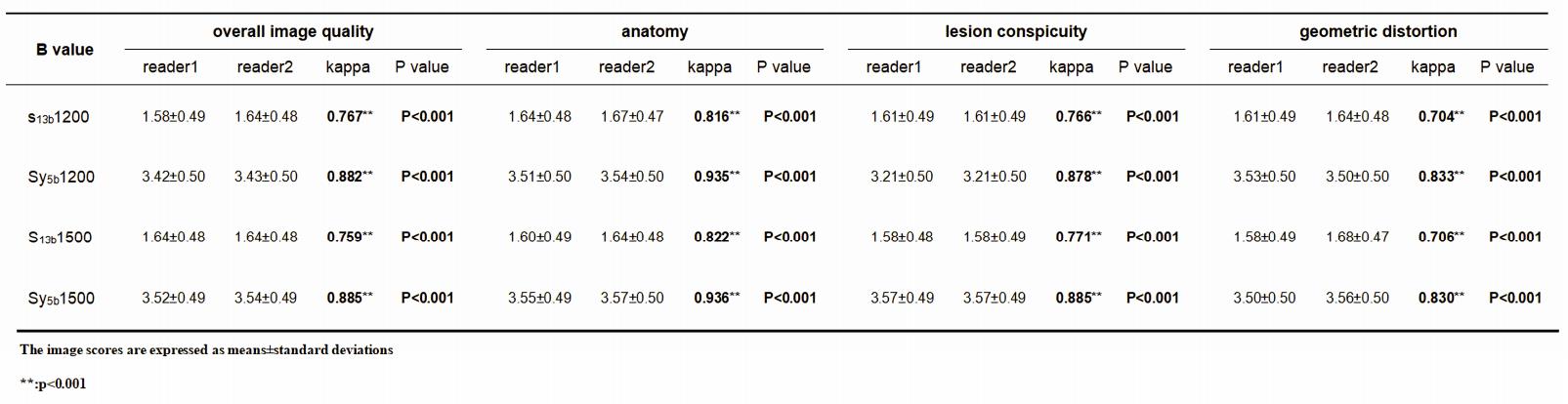
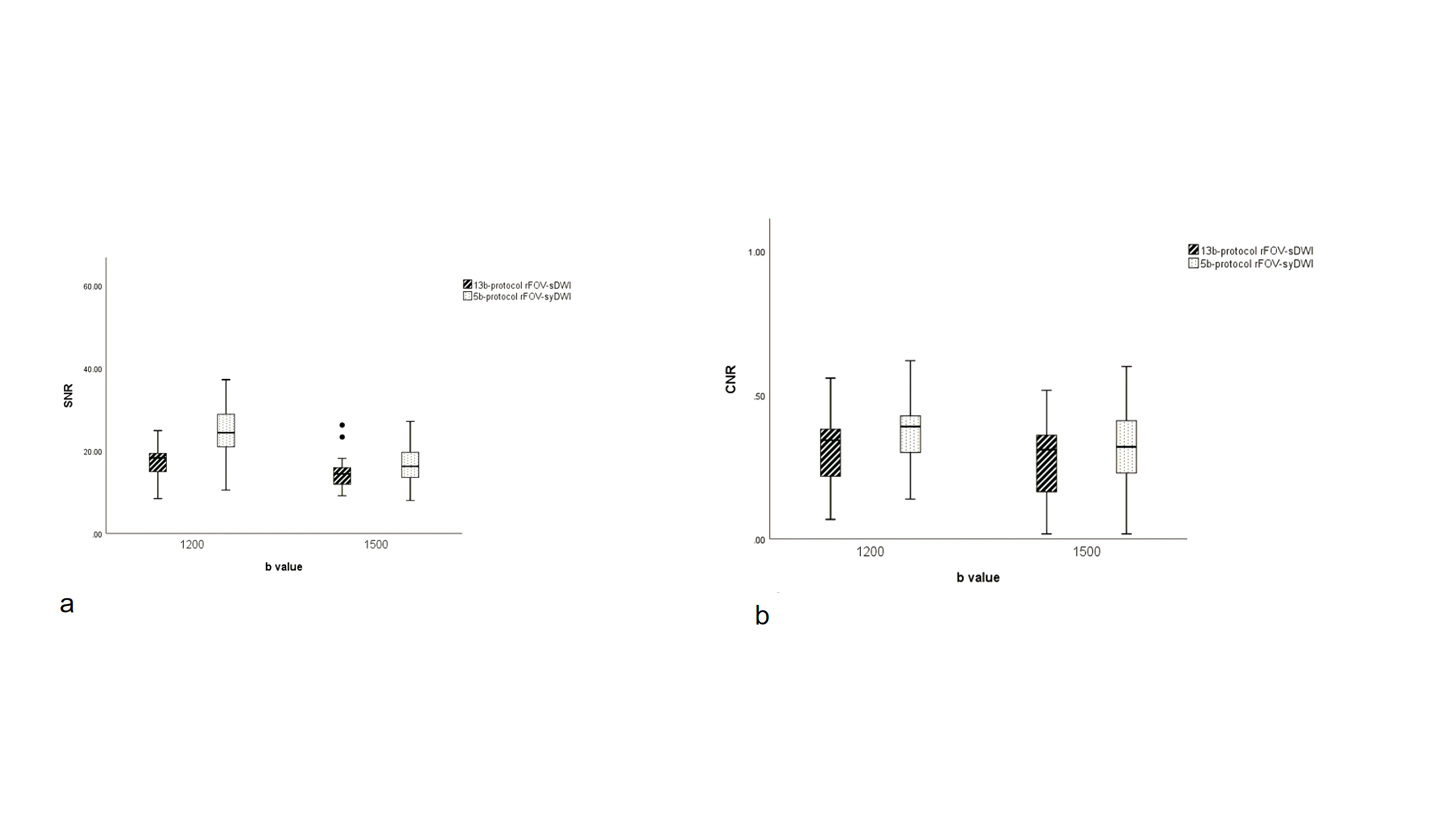
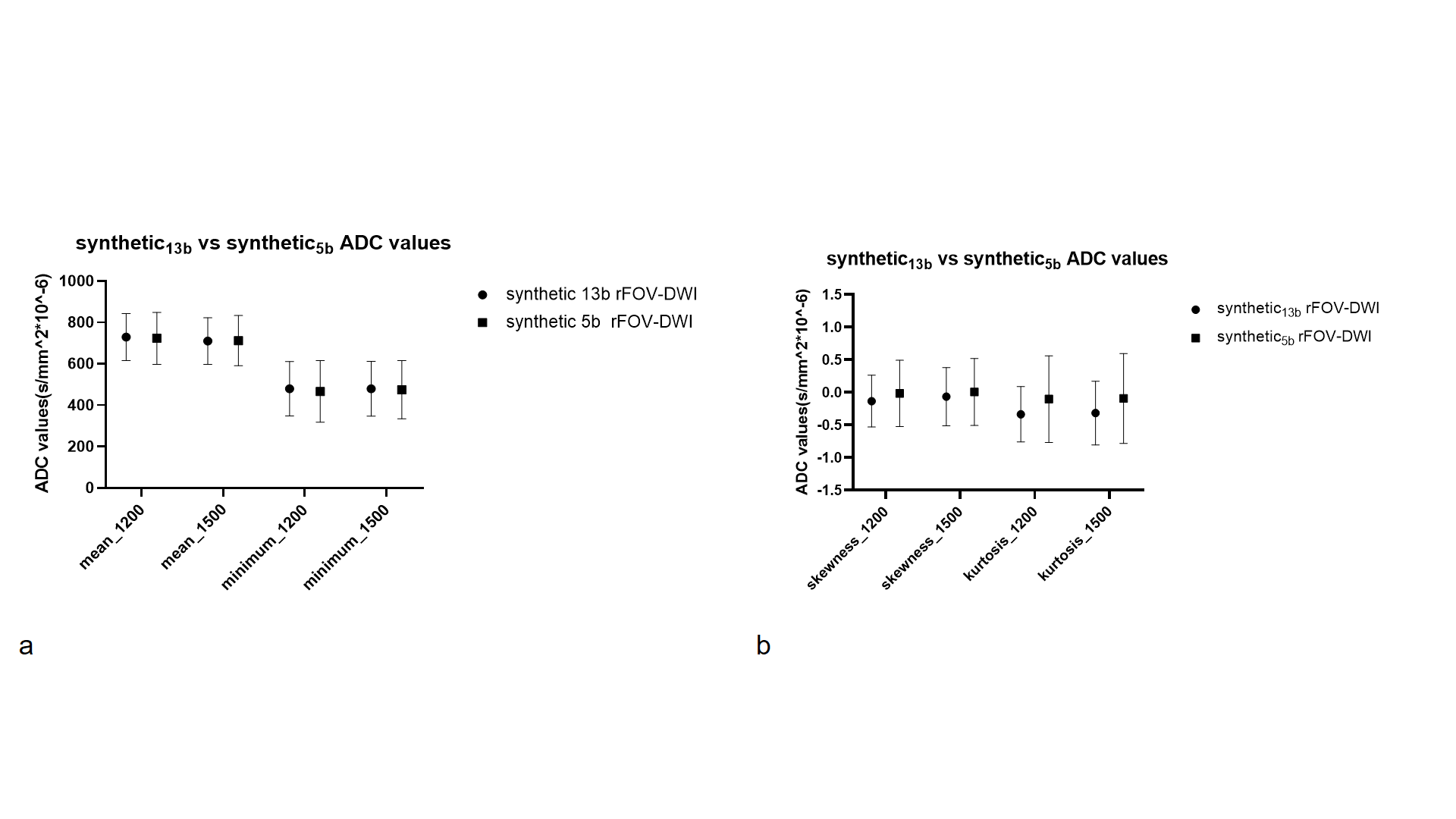
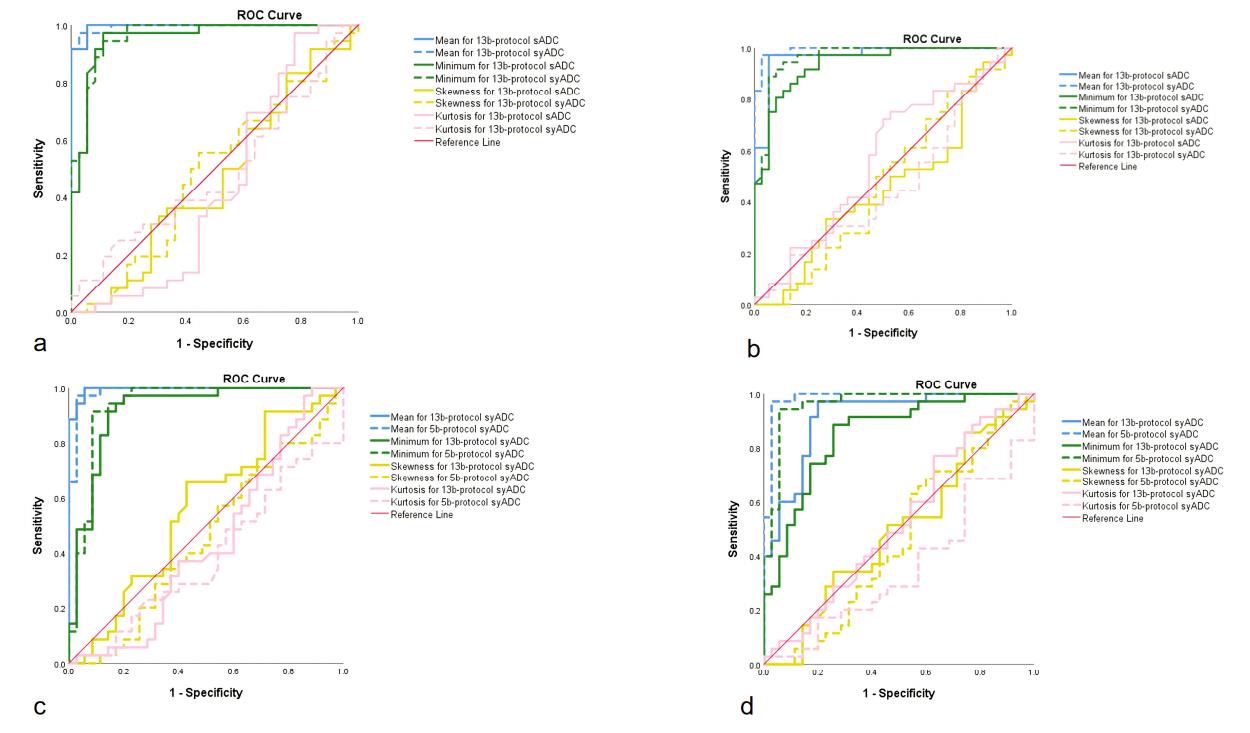
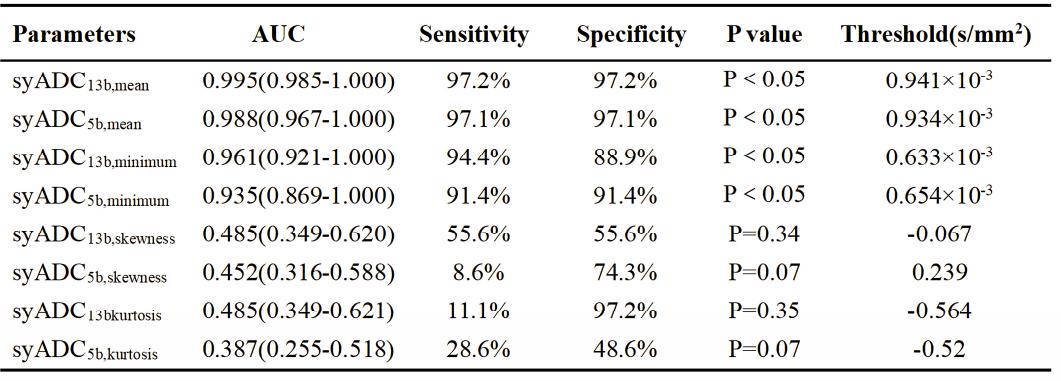
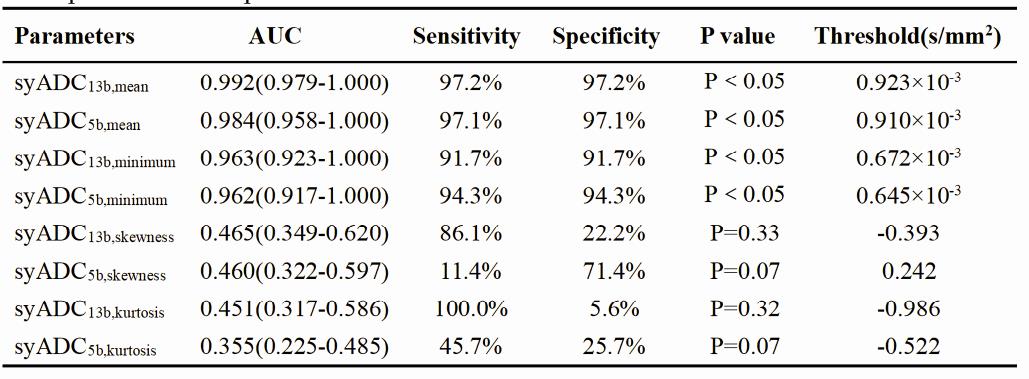
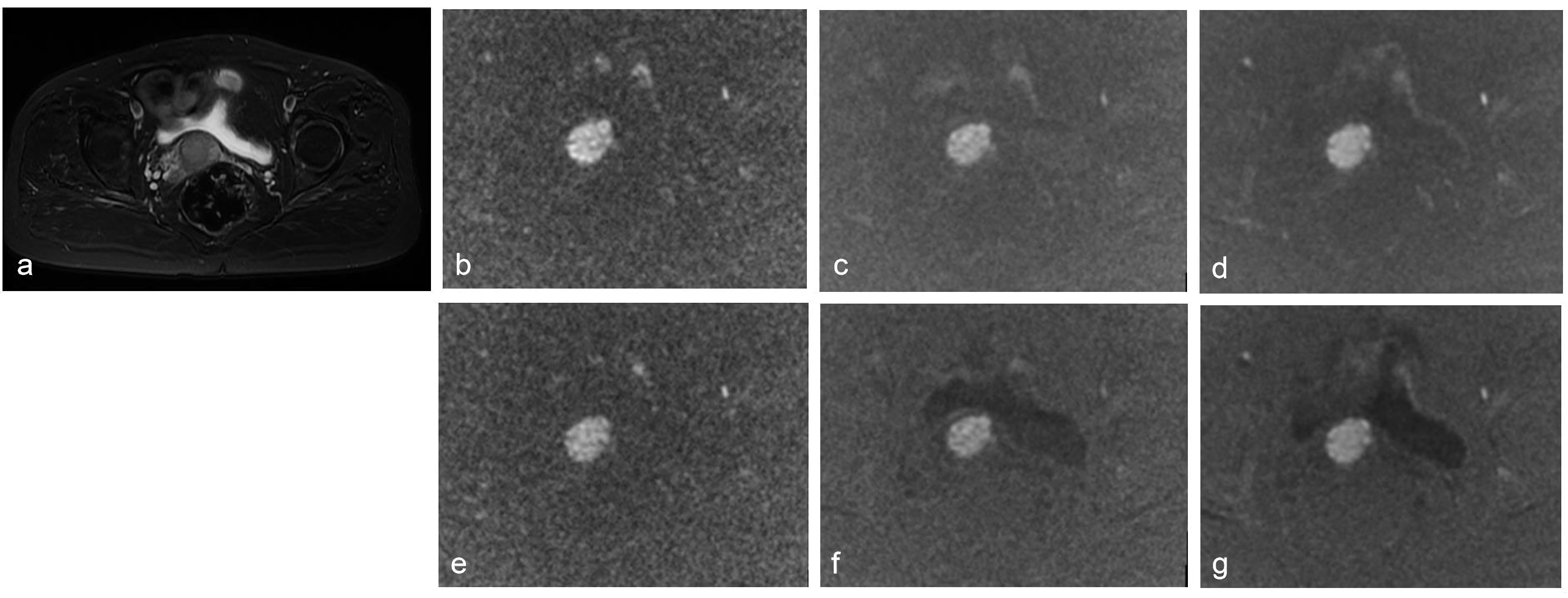
Image quality scores of rFOV-syDWIb=1200/1500 computed based on 5b- and 13b-protocols were evaluated by two radiologists (Table 1). For both multiple-b-value protocols, there were statistically higher scores (U1-U4) between scanned and synthetic DWIs (P < 0.05) and statistically higher inter-reader agreements on synthetic DWIs.SNRs of 13b-protocol and 5b-protocol rFOV-syDWIb=1200/1500 (13b protocol: 31.48±7.44, 21.9±6.01; 5b protocol: 24.6±6.01, 16.79±4.43) were significantly higher than that of 13b-protocol rFOV-sDWIb=1200/1500 (17.18±3.95, 14.39±3.52)(Figure.1). CNRs of 13b-protocol and 5b-protocol rFOV-syDWIb=1200/1500 (13b protocol: 0.36±0.11,0 .33±0.13; 5b protocol: 0.36±0.12, 0.31±0.14) were also significantly higher than that of 13b-protocol rFOV-sDWIb=1200/1500 (0.32±0.12, 0.27±0.12) (Figure.1). For ADC computed by 5b- and 13b-protocol rFOV-syDWIs, no significant difference of histogram-derived parameters from both syADCb=1200/1500 (Fig2). In addition, the AUCs of 5b-protocol syADCmean and syADCminimum were approximately equivalent to those of 13b-protocol syADCmean and syADCminimum (Figure.3, Table2,Table3). Figure. 4 illustrates the scanned and synthetic rFOV-DW images and a corresponding axial T2 weighted image of a patient with cervical cancer.Discussion
We validated 5b-protocol DWI could be an optimal approach to generate high-b-value rFOV-DW images and corresponding ADC maps due to its equivalent diagnosis performance to 13b-protocol one at both aspects of subjective and objective assessment. In our study, four measurements in subjective evaluation of image quality (overall image quality, anatomic deformation degree, background suppression and geometric deformation degree), two independent readers obtained nearly identical Kappa scores on the 13b- and 5b-protocol synthetic DWI images with b =1200 and 1500 s/mm2.An ADC value is influenced by molecular viscosity, membrane permeability, and cell structures, and histogram-derived parameters based on ADC values reflect cell heterogeneity in different physiological states[11]. In our study, both 13b- and 5b-protocol syADCmean and syADCminimum showed good differentiation of cervical cancer from normal tissues and equivalent or even higher diagnostic performance than sADCmean and sADCminimum. But ADCskewness and ADCkurtosis had low diagnostic power probably [12-13] due to absence of hemorrhagic, necrotic or cystic areas within the delineated ROIs in our study in spite that the presence of these excluding areas is considered to be an indicator of tumor heterogeneity.Conclusions
5b-protocol rFOV-syDWIs shorten scan time and provide better lesion clarity and higher image quality. 5b-protocol synthetic ADCmean and ADCminimum offered reliably diagnostic value compared to 13b-protocol ones.Acknowledgements
No acknowledgement found.References
[1] Koh DM, Collins DJ (2007) Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 188(6):1622-35. DOI:10.2214/AJR.06.1403.
[2] Beddy P, Moyle P, Kataoka M et al (2012) Evaluation of depth of myometrial invasion and overall staging in endometrial cancer: comparison of diffusion-weighted and dynamic contrast-enhanced MR imaging. Radiology 262(2):530-7. DOI: 10.1148/radiol.11110984.
[3] Takeuchi M, Matsuzaki K, Harada M (2016) Computed diffusion-weighted imaging for differentiating decidualized endometrioma from ovarian cancer. Eur J Radiol 85(5):1016-9. DOI: 10.1016/j.ejrad.2016.03.009.
[4] Dietrich O, Biffar A, Baur-Melnyk A et al (2010) Technical aspects of MR diffusion imaging of the body. Eur J Radiol 76(3):314-22. DOI: 10.1016/j.ejrad.2010.02.018.
[5] Le Bihan D, Poupon C, Amadon A (2006) Lethimonnier F. Artifacts and pitfalls in diffusion MRI. J Magn Reson Imaging 24(3): 478-88.DOI: 10.1002/jmri.20683.
[6] Blackledge MD, Leach MO, Collins DJ et al (2010) Computed diffusion-weighted MR imaging may improve tumor detection. Radiology 261(2):573-81. DOI: 10.1148/radiol.11101919.
[7] Ortendahl DA, Hylton NM, Kaufman L et al (1984) Signal to noise in derived NMR images. Magn Reson Med 1(3):316-38. DOI: 10.1002/mrm.1910010304.
[8] Maas MC, Fütterer JJ, Scheenen TW et al (2013) Quantitative evaluation of computed high B value diffusion-weighted magnetic resonance imaging of the prostate. Invest Radiol 48(11):779-86. DOI: 10.1097/RLI.0b013e31829705bb.
[9] Harder FN, Jung E, McTavish S et al (2022) High-Resolution, High b-Value Computed Diffusion-Weighted Imaging Improves Detection of Pancreatic Ductal Adenocarcinoma. Cancers (Basel) 14(3):470. DOI: 10.3390/cancers14030470.
[10] Ablefoni M, Surup H, Ehrengut C, et al (2021) Diagnostic Benefit of High b-Value Computed Diffusion-Weighted Imaging in Patients with Hepatic Metastasis. J Clin Med 10(22):5289. DOI: 10.3390/jcm10225289.
[11] Jendoubi S, Wagner M, Montagne S et al (2019) MRI for prostate cancer: can computed high b-value DWI replace native acquisitions? Eur Radiol 29(10):5197-5204. DOI:10.1007/s00330-019-06085-z.[12] Becker AS, Ghafoor S, Marcon M et al (2017) MRI texture features may predict differentiation and nodal stage of cervical cancer: a pilot study. Acta Radiol Open 6(10):2058460117729574. DOI: 10.1177/2058460117729574.
[13] King AD, Chow KK, Yu KH et al (2013) Head and neck squamous cell carcinoma: diagnostic performance of diffusion-weighted MR imaging for the prediction of treatment response. Radiology 266(2):531-8. DOI: 10.1148/radiol.12120167.
Figures