3240
Semi-automated analysis to reduce operator variability in oxygen extraction fraction using susceptometry-based oximetry1Department of Electrical Engineering, National Sun Yat-sen University, Kaohsiung, Taiwan, 2Department of Radiology, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: Data Analysis, Oxygenation
SvO2 and OEF were estimated via susceptometry-based oximetry (SBO). The impact of user-defined ROI was investigated in this study. The results show that (1) the consistency of SvO2 estimation depends on operators’ comprehension of MR-oximetry, (2) SvO2 might be under-estimated with manual ROI selection, and (3) the operator-induced bias can be eliminated by the semi-automatic analysis. The preliminary data indicate the feasibility of the constructed semi-automatic analysis for consistent estimation of SvO2 among operators and its potential for bulk analysis and clinical use.INTRODUCTION
Cerebral oxygen extraction fraction (OEF), defined as the fractional amount of oxygen consumption over oxygen supply, can reflect the balance between cerebral blood flow (CBF) and oxygen consumption (CMRO2). Accordingly, it has been considered as a potential biomarker for brain tissue viability and widely investigated in causality in a variety of diseases, such as Alzheimer’s disease1 and metabolic disorders2. In comparison to 15O PET and T2-based oximetry, susceptometry-based oximetry (SBO), as a calibration-free approach without administration of radiation tracers, has become a great noninvasive alternative for measurement of venous oxygen saturation level (SvO2) which can be subsequently used for OEF estimation3. The reliability and reproducibility of SvO2 via SBO mainly depends on the accumulated phase of venous draining vessel relative to the surrounding brain tissue. However, errors might be additionally propagated into SvO2 estimation in the analysis in terms of experienced and inexperienced operators. Specifically, ill-defined regions-of-interest (ROIs) of the draining vessel and the surrounding compartment might hamper estimation of phase modulation. In this study, we constructed a standardized semi-automatic analysis to eliminate the operator-induced bias in SvO2 estimation. The inter-analyst agreement of SBO was investigated in SvO2 in healthy subjects.METHODS
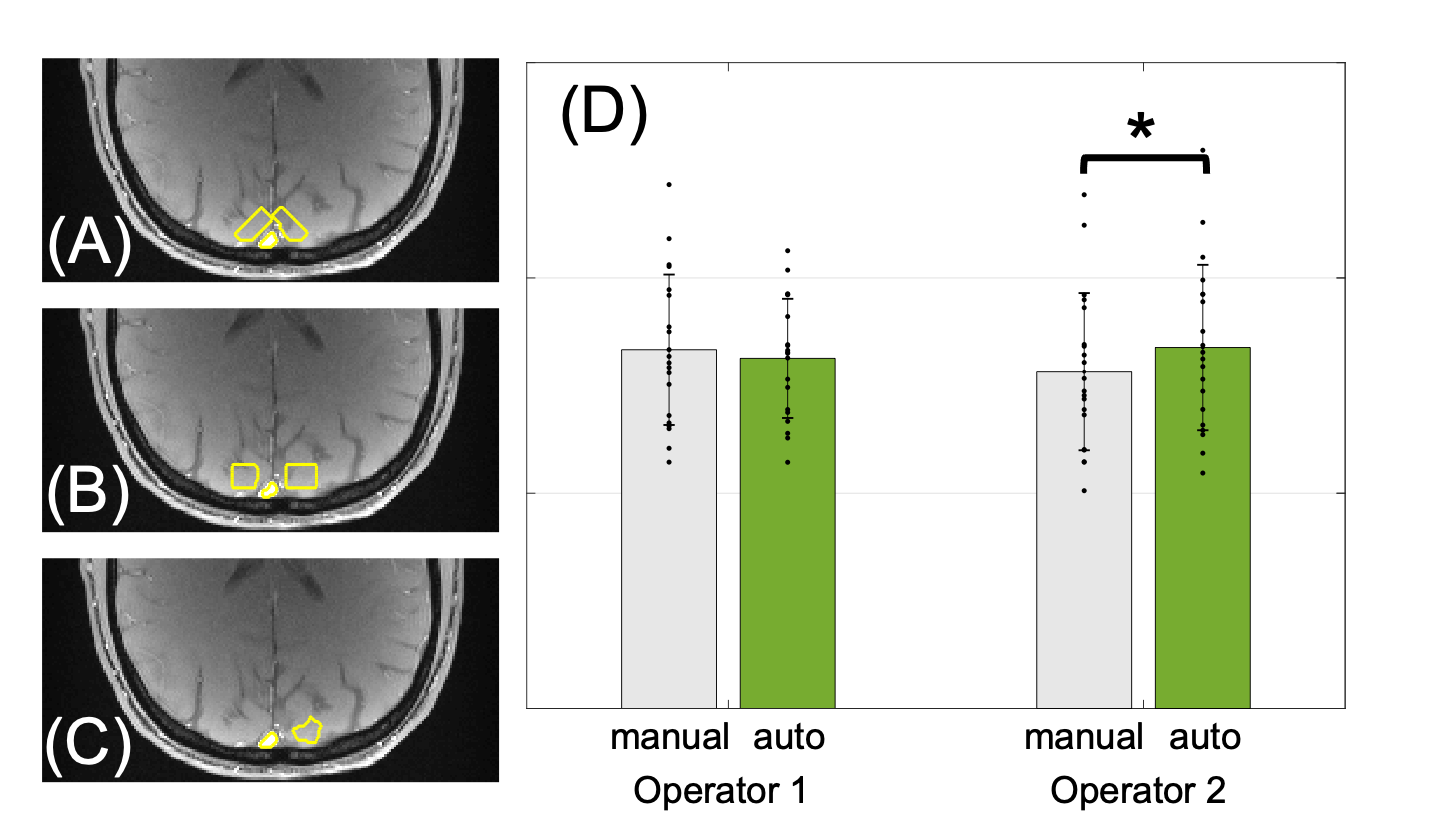
Twenty healthy volunteers (13 males and 7 females, age mean 28.9±5.4 years) were enrolled. Based on SBO approach, SvO2 was determined by measuring phase difference (∆𝜙) between intra-and extravascular compartments accrued over a time ∆𝑇𝐸, $$SvO_2=1-\frac{2|\Delta\phi|}{\gamma B_0\Delta\chi _{do} Hct(\cos^{2}\theta-1/3)\Delta TE}$$ where γ is the gyromagnetic ratio, Δχdo represents the susceptibility difference between fully oxygenated and deoxygenated erythrocytes, Hct is the volume fraction of red blood cells, and θ is the vessel tilt angle relative to the main magnetic field (B0).A two-slice interleaved OxFlow sequence was conducted, which was originally developed to simultaneously quantify SvO2 and whole-brain CBF4, 5. Imaging was performed at 3.0T (Siemens Prisma) using a 64-channel head coil. The scanning parameters of OxFlow protocol were: 1x1x5 mm3 voxel size, flip angle of 15°, TR/TE1/ΔTE=20/5.5/3.71 ms in the superior sagittal sinus (SSS) for SvO2 estimation. Image reconstruction and analysis were performed with in-house MATLAB (MathWorks, Natick, MA) scripts. To improve the consistency of SvO2 estimation, in the semi-automatic post-processing, operators merely needed to locate the data for analysis and determine the ROI span via a rectangle comprising SSS. The SSS in the following was isolated by means of optimum global thresholds determined by maximizing the between-class variance6. The area surrounding the SSS (ref mask) was automatically segmented via morphological processing (i.e., dilation and erosion) of the SSS mask, generating an irregular shape of ten pixels length and four pixels above the SSS, with tiny vessel pixels excluded whose values are larger than the mean +3 standard deviations (Fig. 1A).
The operators comprised one experienced MR physicist (operator 1) with 5 years of practical experience in MR-based oximetry and one inexperienced trainee (operator 2) with more than one-year training period. The training for the latter included didactic lectures on MR physics and supervised OxFlow data analysis to get familiar with the in-house analysis pipeline. For comparison, free-hand ROIs for SSS and ref masks were also extracted by both operators. The measurement from the operator 1 was considered as the reference.
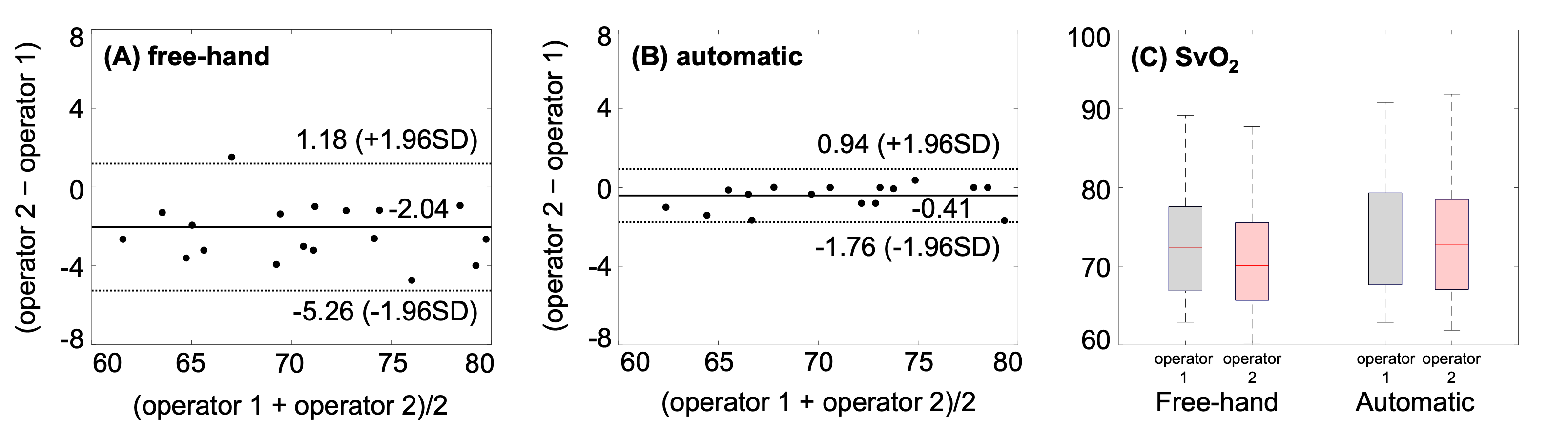
Descriptive data were presented as mean±SD. Wilcoxon signed-rank test and Spearman’s correlation were applied to analyze significance of differences in SvO2 and OEF between manual and automatic ROI selections. Bland and Altman analysis was computed for comparison between operators. A probability value < 0.05 was considered as the criterion for statistical significance.
RESULTS
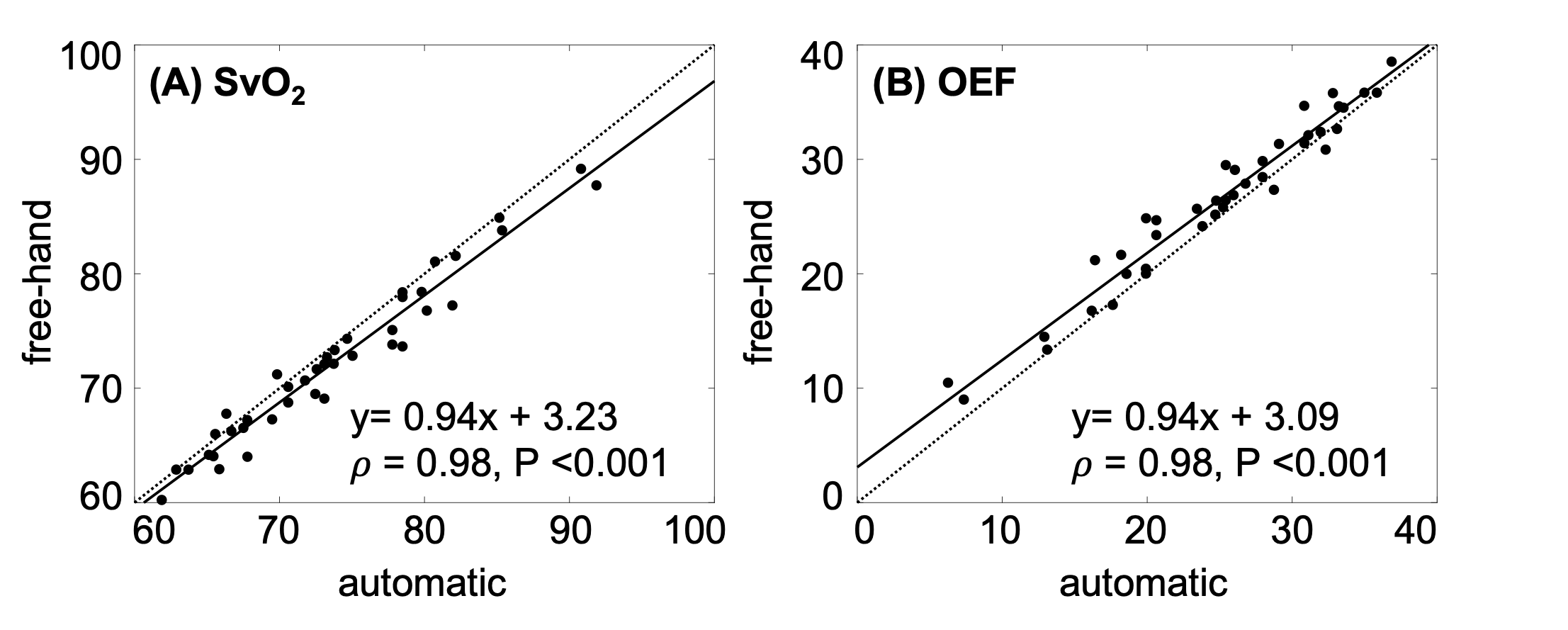
The ROIs (yellow contours) extracted by the semi-automatic analysis (Fig. 1A) and manually by the experienced operator (Fig. 1B) and the inexperienced operator (Fig. 1C) are overlaid on the SSS and the surrounding compartment in a representative magnitude image, showing that the ROIs are well-extracted by the constructed post-processing with the tiny vessel close to SSS excluded. Table 1 lists the SvO2 and OEF estimated with semi-automatic and manual ROI selections. The mean SvO2 is comparable in measurements by the experienced operator (left in Fig. 1D, P=0.39), regardless of the different ROI placements in the surrounding area (Fig. 1A and 1B), but significantly different between methods by operator 2 (right in Fig. 1D, P<0.001). Estimation with free-hand ROI shows smaller values of SvO2 in operator 2 (Fig. 2A and left red box in 2C). On the other hand, parallel SvO2 are found between operators when the semi-automatic analysis is applied (Fig. 2B and two right boxes in 2C). Extremely high correlation in SvO2 between operators indicates the reliability and reproducibility of the semi-automatic analysis (data not shown, 𝜌 = 0.98, P <0.001). Figure 3 demonstrates that manual values are generally under-estimated in SvO2 (𝜌=0.98, P<0.001, slope = 0.94).CONCLUSIONS
The purpose of the study was to present a standardized semi-automatic analysis for elimination of operator-induced bias in SvO2 estimation, which has direct impact on OEF assessment. Note that the measurements of SvO2 by the experienced operator is well consistent with the previous study using a similar pulse sequence5 and considered as the reference. In conclusion, the results show a great inter-analyst agreement, indicating the standardized analysis can significantly maintain reliability and reproducibility of SvO2 via SBO.Acknowledgements
This work was supported by the National science and Technology Council (MOST 110-2314-B-110-005 -)References
1. Jiang, D., et al., Brain Oxygen Extraction Is Differentially Altered by Alzheimer's and Vascular Diseases. J Magn Reson Imaging, 2020. 52(6): p. 1829-1837.
2. Cho, J., et al., Brain oxygen extraction fraction mapping in patients with multiple sclerosis. J Cereb Blood Flow Metab, 2022. 42(2): p. 338-348.
3. Jiang, D. and H. Lu, Cerebral oxygen extraction fraction MRI: Techniques and applications. Magn Reson Med, 2022. 88(2): p. 575-600.
4. Jain, V., M.C. Langham, and F.W. Wehrli, MRI estimation of global brain oxygen consumption rate. J Cereb Blood Flow Metab, 2010. 30(9): p. 1598-607.
5. Rodgers, Z.B., et al., High temporal resolution MRI quantification of global cerebral metabolic rate of oxygen consumption in response to apneic challenge. J Cereb Blood Flow Metab, 2013. 33(10): p. 1514-22.
6. Otsu, N., A threshold selection method from gray-level histograms. IEEE transactions on systems, man, and cybernetics, 1979. 9(1): p. 62-66.
Figures