3215
Evaluation of postcontrast images of glioma using 7T and 3T magnetic resonance imaging: an intraindividual comparison study
Chenxi Li1, Kun Cheng1, Jianxun Qu2, Xiaoxiao Ma1, and Xin Lou1
1Department of Radiology, Chinese PLA General Hospital, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd., Beijing, China
1Department of Radiology, Chinese PLA General Hospital, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd., Beijing, China
Synopsis
Keywords: Tumors, Brain
With the advent of the 7T device meeting the need for ultra-high resolution, we planned to explore the advantages of 7T over 3T in terms of the internal detail display of gliomas. Seventeen patients with glioma were individually rated for internal tumor structure and feeding artery by 6 radiologists at 7T and 3T MR, and the DCS score was calculated. 7T revealed better details of internal tumor structure and higher diagnostic confidence than 3T.BACKGROUND AND PURPOSE
The signal-to-noise ratio and the longitudinal relaxation time have increased with the increase in magnetic field, thus benefiting high-resolution imaging and contrast-enhanced imaging based on the T1 mechanism1. A previous study demonstrated that the 7T 3D contrast-enhanced T1w sequence with higher resolution could detect 8% more metastases compared with the high-field platform2. Another study on gliomas reported that the 7T 3D contrast-enhanced T1w sequence provided excellent image contrast of presumed microvasculature and necrosis in astrocytomas, which was only a descriptive evaluation 3. Quantitative assessment of the internal structure of glioma is still lacking. This study aimed to evaluate the degree of visualization of the internal structure and feeding arteries of gliomas using 7T and 3T magnetic resonance imaging (MRI) scanners and calculate the diagnostic confidence scores to determine the potential benefits of ultra-high-field MRI for clinical applications.METHODS
This prospective study included 17 patients (age 46.23 ± 9.50 years, 10 male and 7 female) with newly diagnosed and histopathologically confirmed glioma [8 patients with World Health Organization (WHO) grade 4 and 9 patients with WHO grade 2–3]. The inclusion criteria were patients with MRI findings suspicious of glioma, previously untreated, age >18 years, and willing to undergo surgical resection or puncture biopsy at our institution. Patients with contraindications to MRI scans, such as metal implants, dentures, claustrophobia, contrast agent allergy, and kidney failure, were excluded from the study. Only supratentorial tumors were included to avoid the influence of the deteriorated B1 field beneath the subtentorial region. All 17 patients had good image quality and were free of motion and other artifacts. The study was approved by the local research ethics committee and registered at ClinicalTrials.gov (NCT05287750), and all patients provided signed informed consent.This study was performed with a 7T whole-body MR scanner (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) equipped with an 8-channel transmitting and 32-channel receiving head coil and a 3T whole-body MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) equipped with a 20-channel head coil. The circular polarity mode was used for 7T transmission. All the patients received 3D T1-weighted magnetization-prepared rapid acquisition of gradient echo (MPRAGE) at first 3T and 7T after administering gadolinium contrast agent at 0.1 mmol/kg. The 3T and 7T MPRAGE scans were performed successively within 20 minutes to reduce the changes in lesion enhancement 4,5. The acquisition time for 3T and 7T was nearly 5 minutes. For 7T, the imaging parameters were as follows: repetition time (TR)/echo time (TE)/inversion time (TI) =2300/1.99/1050 milliseconds; field of view (FOV) = 224mm × 224 mm; flip angle = 8°; resolution = 320 × 320; and slice thickness = 0.7 mm. For 3T, the imaging parameters were TR/TE/TI = 2300/2.98/900 milliseconds; FOV=224mm × 210mm; flip angle = 9°, resolution = 224 × 210, and slice thickness = 1.0 mm. The protocols were adjusted to achieve a higher spatial resolution at 7 T in a similar acquisition time, ensuring the feasibility of its clinical application.
Six experienced radiologists, all specialized in neuroimaging, scored the tumor details for the 3T and 7T images on 2 aspects: internal structures and feeding arteries. The images were rated with 5 levels according to the degree of the display: “Definitely display,” “Probably display,” “Small chance of display,” “Quite likely undisplay,” and “Definitely undisplay”6. The diagnostic confidence score (DCS) was calculated as the averaged tumor detail score6,7. The higher the DCS score, the greater the confidence in a definitive diagnosis. The statistical analyses were performed with SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The interobserver agreement of MRI readings was assessed using the intraclass correlation coefficient (ICC). The paired-sample t tests were performed to examine the group difference in DCS between 7T and 3T. A P value <0.05 indicated a statistically significant difference.
RESULTS
For tumor detail evaluation, 6 radiologists achieved moderate-to-excellent reliability in data measurement and assessment (ICC > 0.6). The mean DCSs of both internal structure and feeding artery was remarkably higher at 7T than at 3T (internal structure: 7.83 ± 5.91 vs –3.17 ± 2.22, P = 0.009, feeding artery: 12.75 ± 4.22 vs 2.46 ± 3.89, P < 0.001) (Fig. 1). Figure 2 shows the comparisons of 2 patients with glioma. 7T CE-MPRAGE images could reveal the internal structure and feeding arteries more clearly than 3T images.DISCUSION AND CONCLUSION
This study performed a semi-quantitative assessment of CE-MPRAGE images for brain glioma at 7T and 3T. 7T achieved better visualization of tumor details (internal structure and feeding artery) and higher DCS. Visualizing internal structures helps explore the heterogeneity of tumors, which is of great significance in distinguishing the grade of tumors and improving the accuracy of biopsy. The visualization of feeding arteries can avoid bleeding during biopsy and reduce the occurrence of surgical accidents to a certain extent.Acknowledgements
NoneReferences
- Kraff O, Fischer A, Nagel AM, et al. MRI at 7 Tesla and above: demonstrated and potential capabilities. J Magn Reson Imaging. 2015;41(1):13-33.
- Mönninghoff C, Maderwald S, Theysohn JM, et al. Imaging of brain metastases of bronchial carcinomas with 7 T MRI - initial results. Rofo. 2010;182(9):764-772.
- Moenninghoff C, Maderwald S, Theysohn JM, et al. Imaging of adult astrocytic brain tumours with 7 T MRI: preliminary results. Eur Radiol. 2010;20(3):704-713.
- Akeson P, Nordström CH, Holtås S. Time-dependency in brain lesion enhancement with gadodiamide injection. Acta Radiol. 1997;38(1):19-24.
- Ellingson BM, Bendszus M, Boxerman J, et al. Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro Oncol. 2015;17(9):1188-1198.
- Springer E, Dymerska B, Cardoso PL, et al. Comparison of Routine Brain Imaging at 3 T and 7 T. Invest Radiol. 2016;51(8):469-482.
- Stahl R, Krug R, Kelley DA, et al. Assessment of cartilage-dedicated
sequences at ultra-high-field MRI: comparison of imaging performance and
diagnostic confidence between 3.0 and 7.0 T with respect to
osteoarthritis-induced changes at the knee joint. Skeletal Radiol.
2009;38(8):771-783.
Figures
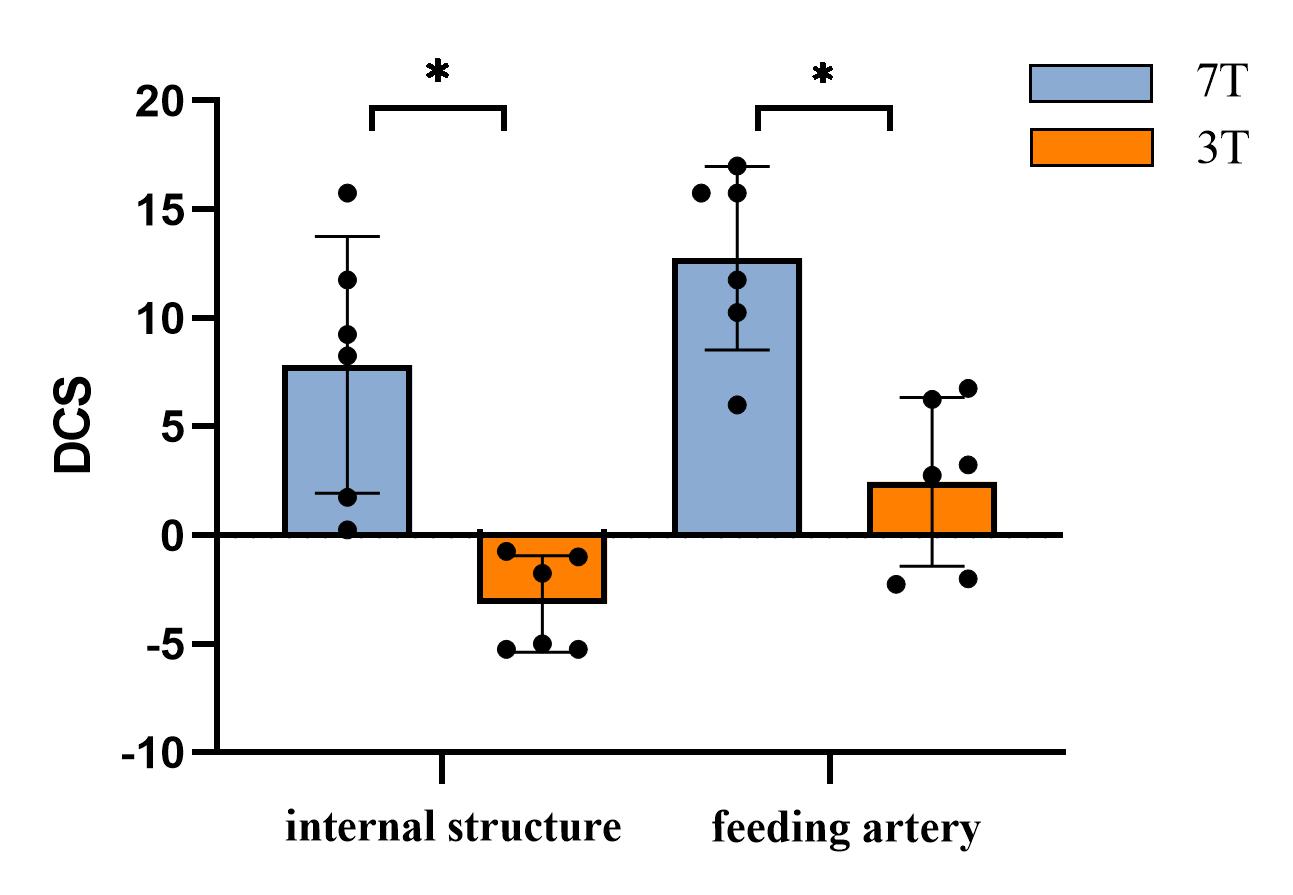
Figure
1. Mean diagnostic confidence scores
(DCS) of the tumor’s internal structure and feeding artery in 7T and 3T
magnetic resonance images. The bar and dot plots represent the mean score of
each category and exact data points. *Statistically significantly different
results, with P <0.05.
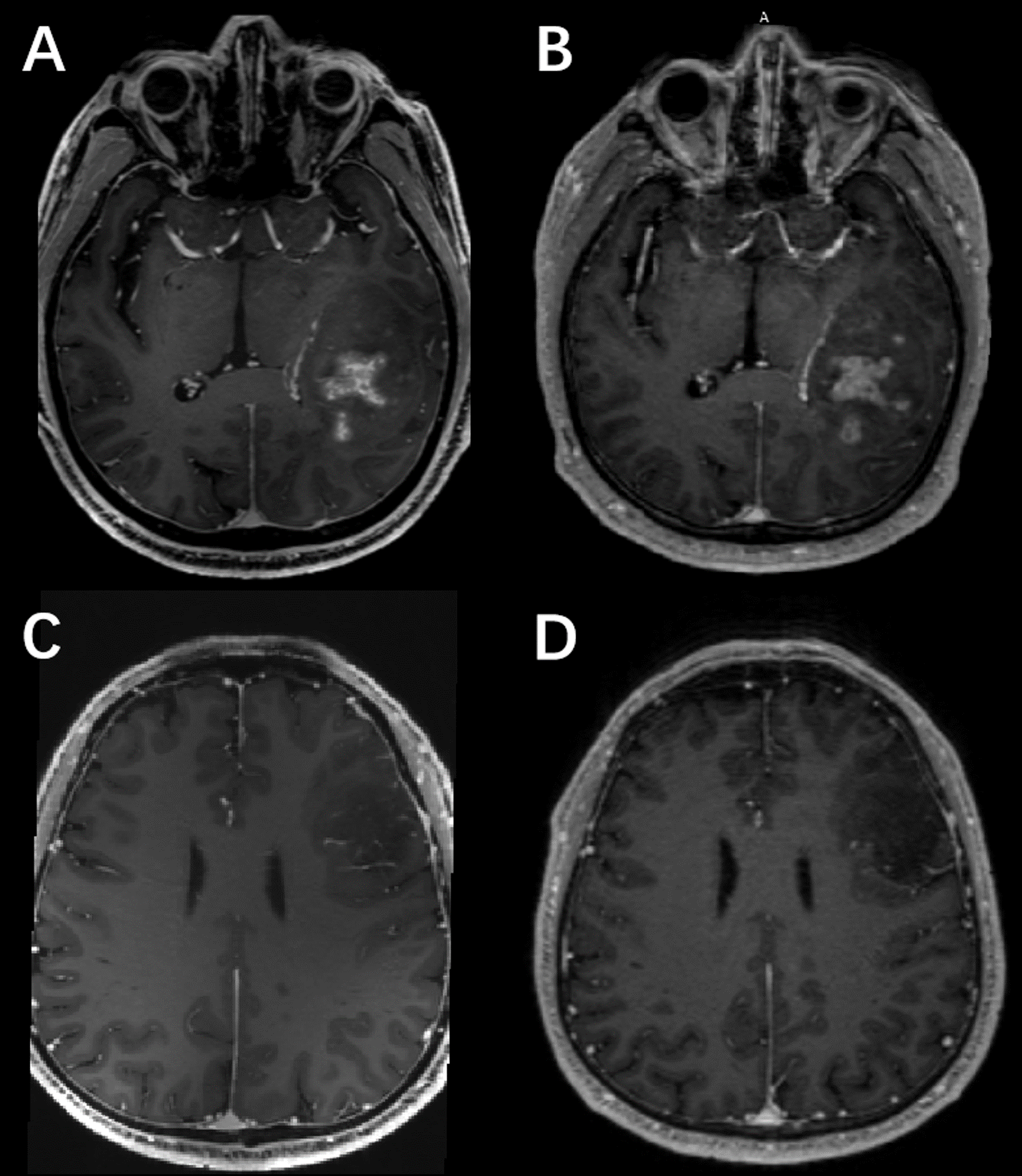
Figure
2. After
contrast agent application at 7T (A) and 3T (B) in a 47-year-old male patient
with oligodendroglioma (WHO grade 3), the 7T image provided greater visibility
of the internal structure of the lesion than the 3T image. After contrast agent
application at 7T (C) and 3T (D) in a 45-year-old male patient with astrocytoma
(WHO grade 2), the 7T image displayed greater visibility of the feeding artery
of the lesion than the 3T image.
DOI: https://doi.org/10.58530/2023/3215