3213
Advanced intraoperative image quality using multiple surface coils.
Pien E.J. Jellema1,2, Fredy Visser2, Niels Blanken3, Alberto de Luca2,4, Eelco W. Hoving1,5, Kirsten M. van Baarsen1,5, Maarten H. Lequin1,3, and Jannie Wijnen2
1Pediatric Neuro-Oncology, Princess Máxima Centre, Utrecht, Netherlands, 2Centre for Image Sciences, University Medical Centre Utrecht, Utrecht, Netherlands, 3Department of Radiology, University Medical Centre Utrecht, Utrecht, Netherlands, 4Department of Neurology, University Medical Centre Utrecht, Utrecht, Netherlands, 5Department of Neurosurgery, University Medical Centre Utrecht, Utrecht, Netherlands
1Pediatric Neuro-Oncology, Princess Máxima Centre, Utrecht, Netherlands, 2Centre for Image Sciences, University Medical Centre Utrecht, Utrecht, Netherlands, 3Department of Radiology, University Medical Centre Utrecht, Utrecht, Netherlands, 4Department of Neurology, University Medical Centre Utrecht, Utrecht, Netherlands, 5Department of Neurosurgery, University Medical Centre Utrecht, Utrecht, Netherlands
Synopsis
Keywords: Tumors, Surgery
Advanced intraoperative MRI (io-MRI) could provide additional guidance during pediatric neurosurgery. Currently, io-MRI sequences are acquired with two surface coils when using the DORO head-frame. We investigated if the addition of two surface coils and higher SENSE-factors would increase signal- and contrast-to-noise ratios (SNR & CNR), image quality, and decrease artefacts. The four coils set-up resulted in higher T1w SNR and CNR that was more homogeneously distributed. Image quality of T1w, T2w, and fiber-tracks did improve with four coils. Higher SENSE factors with four coils of most ASL and diffusion MRI images did not reduce EPI artefacts or improve image quality.Body of the abstract
IntroductionWith intraoperative MRI (io-MRI) resection control during surgery of pediatric brain tumors can be obtained. Currently this is mostly based on T1- and T2-weighted (T1w and T2w) MRI1. More advanced MRI sequences could potentially provide additional guidance in both the extent of resection and understanding the impact of the neurosurgical procedure on the tumor environment and brain of a child. For example, arterial spin labelling (ASL) can provide information on intraoperative cerebral perfusion2, whereas diffusion MRI (dMRI) fiber tractography can be used to update the anatomy of brain tracts during surgery1. When the DORO surgical head fixation frame2 is used only two surface coils can be used which limits the application of SENSE. Here we investigate using four surface coils for advanced io-MRI, compatible with the DORO frame, with increased SENSE factor to reduce EPI image distortions. We compare image quality, signal- and contrast-to-noise ratio (SNR and CNR) of T1w, T2w, ASL and dMRI acquired with two and four surface coils but with similar acquisition time and spatial resolution.
Methods
Study set-up
This study was approved by the local ethical review board. Two healthy volunteers (aged 24 and 28; one female) participated in this study after providing written informed consent. We obtained MR images with a 3T Philips Ingenia system (70cm bore) using two or four surface coils (Fig.1).
For the four coils set-up, the optimal positioning of the two overlapping surface coils with respect to each other was determined by measuring the S21 using a double pickup probe connected to a network analyzer. The optimal decoupling was achieved then when the neighboring elements were around 3cm at 30° in overlap.
The scan protocol consisted of T1w, T2w, ASL and dMRI sequences. The protocol with two coils was based on the clinical intraoperative protocol of our institution that was optimized for a total duration of ~20 minutes. The four coils protocol has the same acquisition time and resolution, but has been optimized for image quality using SENSE or compressed SENSE (Table 1).
Quantitative analysis
The T1w images were used to calculate the SNR and CNR. To this end, a dynamic noise scan was added to the T1w sequence where during the second dynamic the RF and gradient amplifiers were disabled. After brain extraction (BET FSL-toolbox), signal maps were registered to MNI space (FLIRT FSL-toolbox) and segmented into grey- and white matter (GM and WM) using FAST FSL-toolbox3. The noise maps were spatially smoothed with a standard deviation kernel of 9x9x9 voxels4. The GM and WM segments were used to deduct the corresponding noise voxels. SNR and CNR were calculated according to the following equations5:
SNR = S/σ
CNR = |μSWM - μSGM| / μ(σWM + σGM)
S: Signal
SWM, SGM: Signal white matter, signal grey matter
σ: Noise
σWM, sGM: Noise white matter, noise grey matter
μ: Mean
Qualitative analysis
A neuroradiologist (MHL) performed the preliminary qualitative assessment of the MR sequences for both set-ups. This included T1w and T2w images, an unquantified pcASL image, fractional anisotropy (FA) color-coded maps, and b0 maps without diffusion weighting. A dMRI expert (AL) preliminary assessed the corticospinal tract (CST) and arcuate fasciculus (AF, Fig.2). Overall image quality, anatomical details, grey-white matter contrast, image artefacts, and dMRI details were scored using a five-point Likert scale3 (Table 2).
Results
Quantitative analysis
Median GM SNR was higher for four coils (90.34 ±45.17, Fig.3A) than for two coils (66.32 ±31.64), similarly median WM SNR was higher for four coils (104.97 ±55.74, Fig.3B) than for two coils (77.63 ±39.86). CNR was also higher for four coils (15.82) than for two coils (12.34). All SNR distributions amongst the number of voxels revealed a skewed distribution. In both GM and WM the two coils set-up was more inhomogeneously distributed than the four coils set-up.
Qualitative analysis
Average scores of image quality of T1w and T2w images were higher for four coils. Image artefacts were equally scored for T1w, but slightly better scored for T2w images with four coils. ASL images and FA-color coded maps with the two coils were scored higher in image quality and had less artefacts than with four coils. No differences were found amongst the set-ups regarding b0 maps. DMRI details of CST and AF were higher scored with four coils than two coils.
Discussion
The set-up with four coils was higher in SNR, CNR, and more homogeneously SNR distributed over voxels. The T1w and T2w images were accordingly also scored higher when acquired with four coils. This could be explained by the larger amount of voxels that are more closely located to a surface coil compared to the two coils set-up.
All ASL and dMRI images were rated clinically acceptable. Quality of fiber tracks did improve with more coils. However, higher SENSE factors with four coils of most ASL and dMRI images did not reduce EPI artefacts or improve image quality. Varying coil positioning amongst participants may have resulted in varying image quality. For example, ASL images with four coils of the two participants were scored both highest and lowest. Qualitative assessment by a second independent neuroradiologist and inclusion of more participants may clarify our results.
Acknowledgements
No acknowledgement found.References
- Tejada, S., Avula, S., Pettorini, B., Henningan, D., Abernethy, L., & Mallucci, C. (2018). The impact of intraoperative magnetic resonance in routine pediatric neurosurgical practice—a 6-year appraisal. Childs Nerv Syst, 34, 617–626. https://doi.org/10.1007/s00381-018-3751-8
- Lindner, T., Ahmeti, H., Helle, M., Jansen, O., Fiehler, J., Dührsen, L., Synowitz, M., Kesari, S., & Ulmer, S. (2022). Measurements of Functional Network Connectivity Using Resting State Arterial Spin Labeling During Neurosurgery. World Neurosurg, 157, 152–158. https://doi.org/10.1016/j.wneu.2021.10.107
- Jacobs, S. M., Versteeg, E., van der Kolk, A. G., Visser, L. N. C., Oliveira, Í. A. F., van Maren, E., Klomp, D. W. J., & Siero, J. C. W. (2022). Image quality and subject experience of quiet T1-weighted 7-T brain imaging using a silent gradient coil. Eur Radiol Exp, 6, 1–9. https://doi.org/10.1186/s41747-022-00293-x
- Wiens, C. N., Kisch, S. J., Willig-Onwuachi, J. D., & McKenzie, C. A. (2011). Computationally rapid method of estimating signal-to-noise ratio for phased array image reconstructions. Magn Reson Med, 66, 1192–1197. https://doi.org/10.1002/mrm.22893
- Oliveira, Í. A. F., Roos, T., Dumoulin, S. O., Siero, J. C. W., & van der Zwaag, W. (2021). Can 7T MPRAGE match MP2RAGE for gray-white matter contrast? NeuroImage, 240, 1–9. https://doi.org/10.1016/j.neuroimage.2021.118384
- Guo, F., Leemans, A., Viergever, M. A., Dell’Acqua, F., & De Luca, A. (2020). Generalized Richardson-Lucy (GRL) for analyzing multi-shell diffusion MRI data. NeuroImage, 218, 1–16. https://doi.org/10.1016/j.neuroimage.2020.116948
- Zhang, F., Wu, Y., Norton, I., Rathi, Y., Golby, A. J., & O’Donnell, L. J. (2019). Test–retest reproducibility of white matter parcellation using diffusion MRI tractography fiber clustering. Hum Brain Mapp, 40, 3041–3057. https://doi.org/10.1002/hbm.24579
Figures
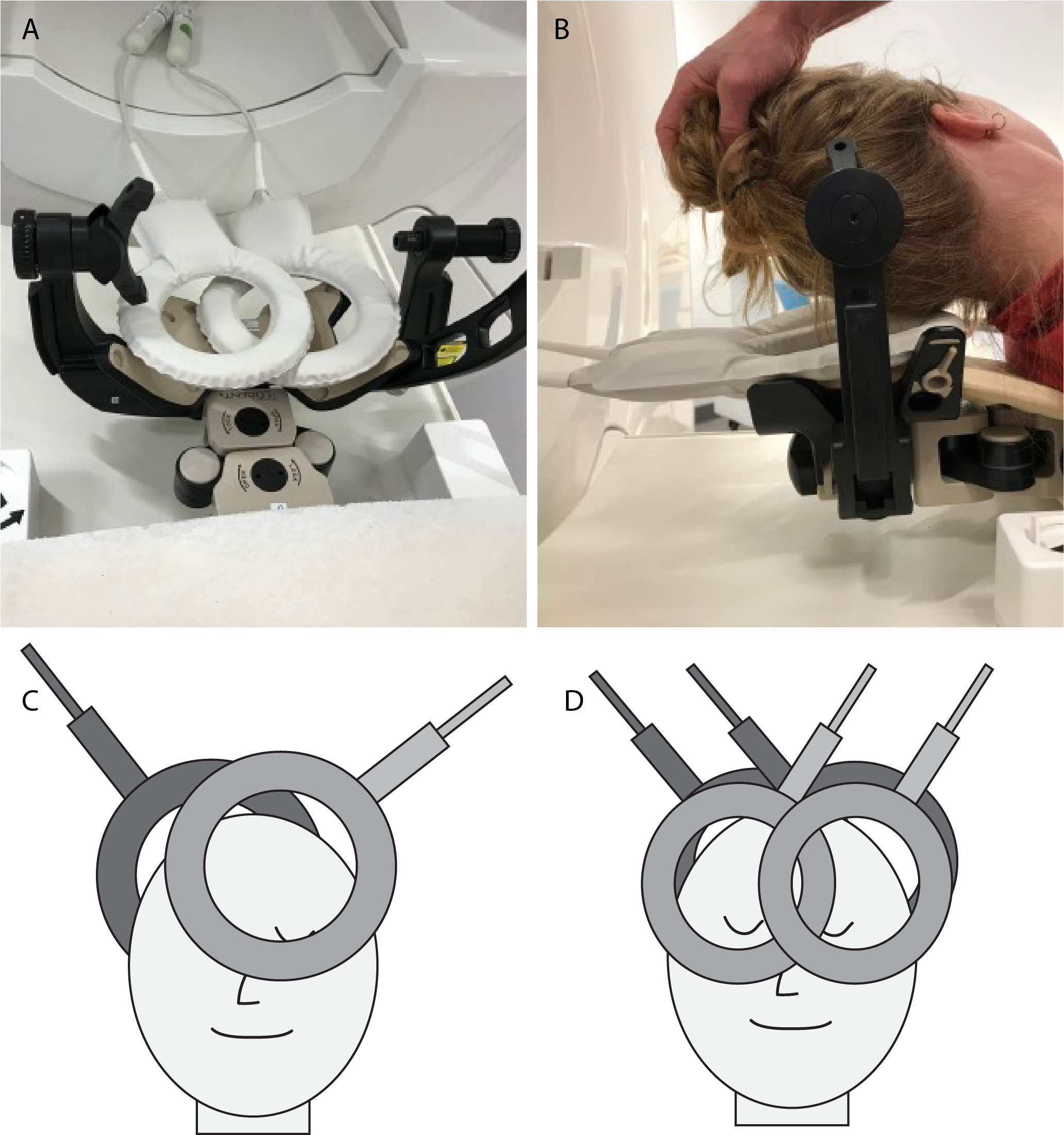
Fig.1 Set-up of surface coils used for intraoperative MRI acquisition. A, Two surface coils in the DORO surgical head-frame and neuronavigation matrix; B, Participant positioning within surgical head-frame; C, Set-up with two 20cm diameter coils; D, Set-up with four surface coils in overlap position; two 20cm and two 15cm diameter coils.
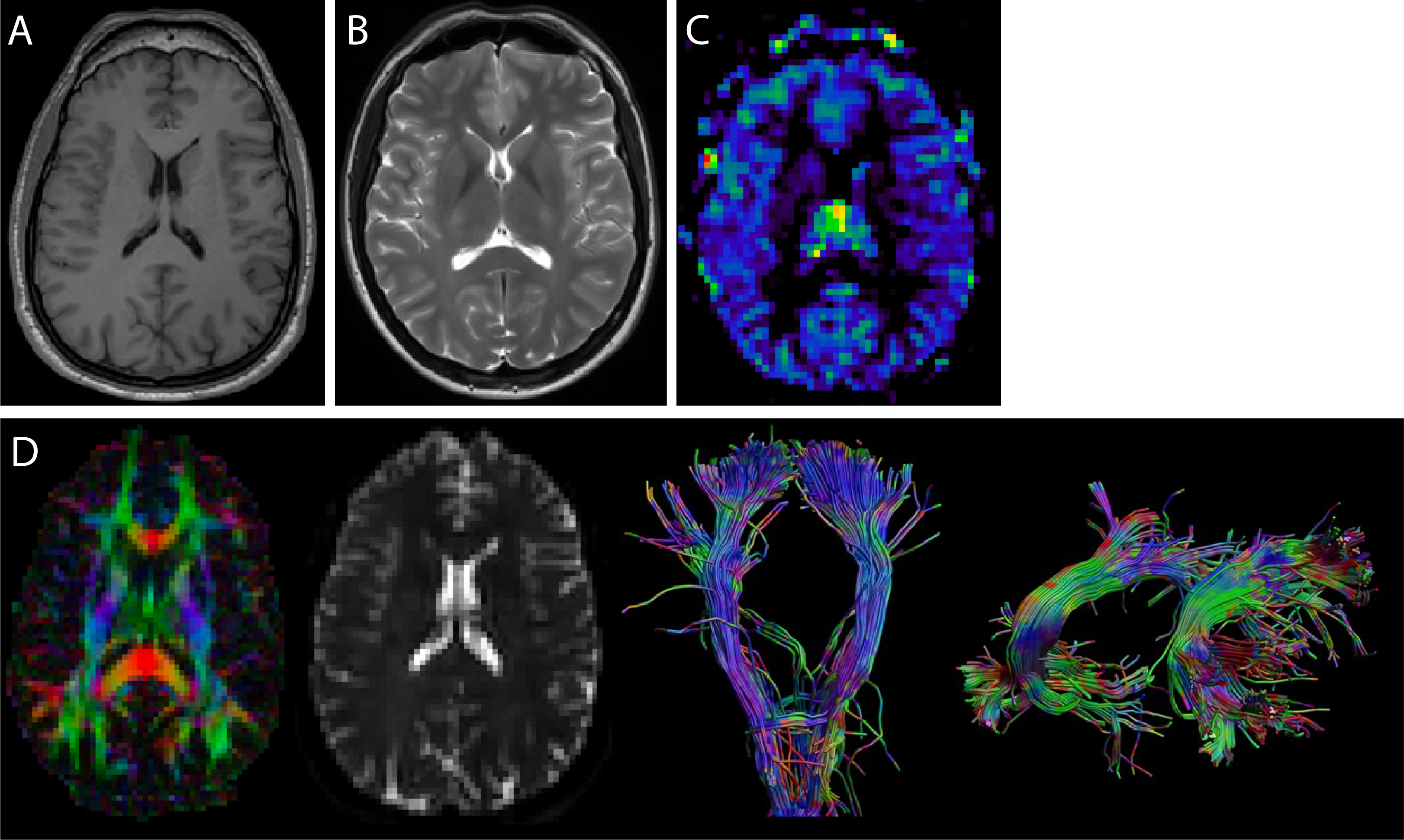
Fig.2 Axial slices of all sequences. A, T1w; B, T2w; C, Unquantified ASL perfusion map; D, FA color coded map (first), b0 map (second), Corticospinal tract (CST, third) Arcuate fasciculus (AF, fourth). Deterministic fiber tractography was performed on all sequences with a multi-shell spherical deconvolution approach6, using identical parameters (using all voxels as seed, step size 1mm, angle threshold 45°). The CST and AF were segmented using the WMA method7 and evaluated as proxy of image quality.
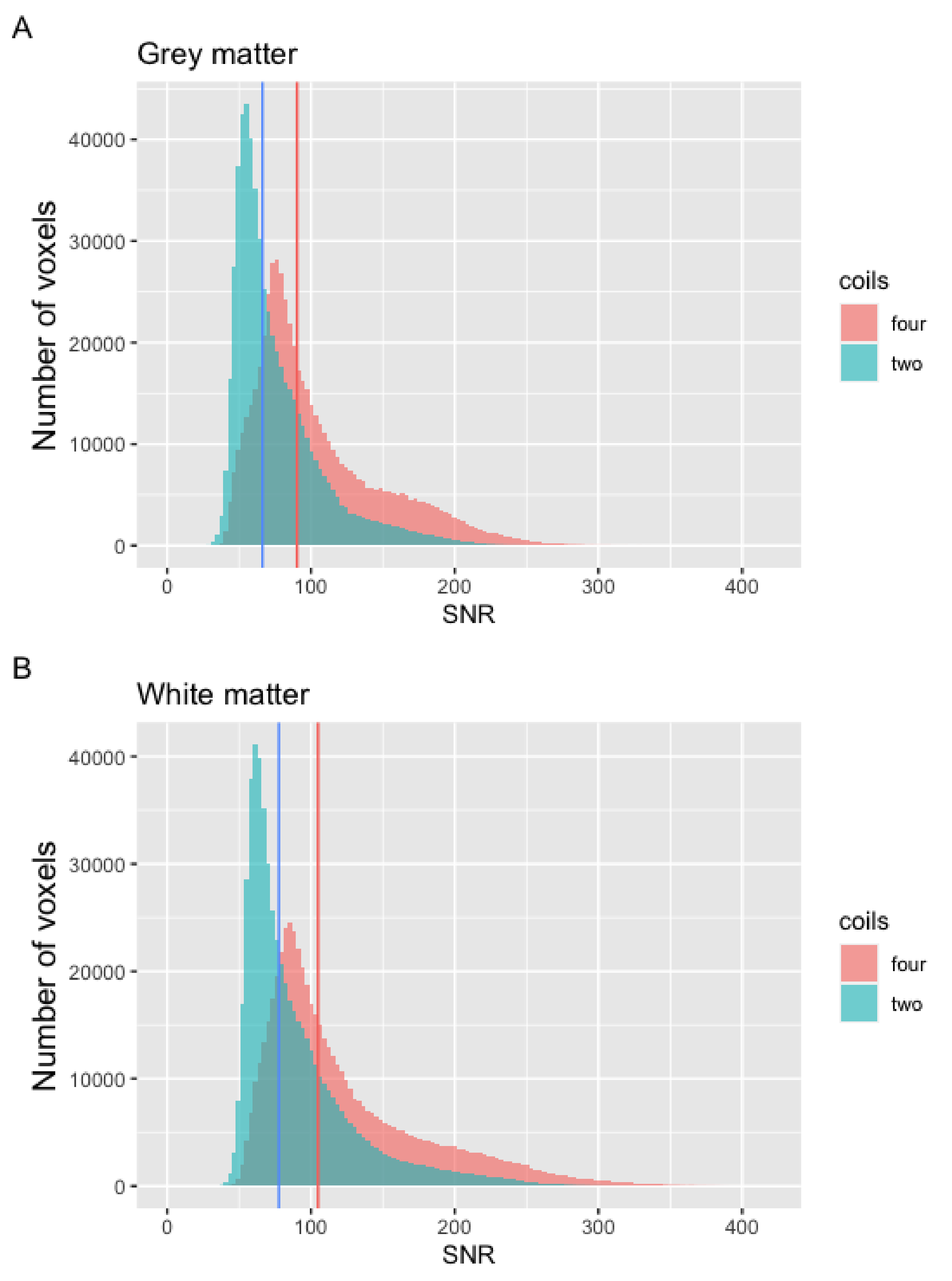
Fig.3 Distribution of signal-to-noise ratio (SNR) within voxels measured with two or four surface coils. A, Grey matter; B, White matter. Vertical lines depict median values: A, blue: 66.32; A, red: 90.34; B, blue: 77.63; B, red: 104.97.

Table 1. Imaging parameters of T1, T2, pseudo-continuous ASL (pCASL), and multi-shell diffusion MRI (dMRI) sequences. S = SENSE; CS = Compressed SENSE. Note that CS cannot be used in EPI sequences such as often used for ASL and dMRI.
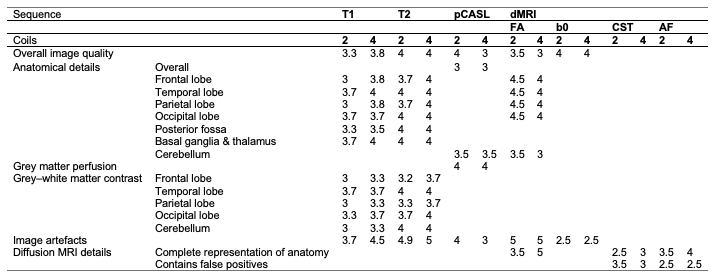
Table 2. Preliminary results of qualitative analysis of T1, T2, pseudo-continuous ASL (pCASL), and diffusion MRI (dMRI) sequences with two or four coils. Average scores on image quality, anatomical details, grey-white matter contrast using a 5-point Likert scale (1 = very poor, 2 = poor, 3 = acceptable, 4 = good, 5 = excellent). Image artefacts were scored using another 5-point Likert scale: 1 = severe, 2 = obvious, 3 = moderate, 4 = mild, 5 = none. FA = Fractional anisotropy; CST = Corticospinal tract; AF = Arcuate fasciculus.
DOI: https://doi.org/10.58530/2023/3213